
Abstract
Summary:
Despite the increase of HIV-1-associated Kaposi's sarcoma (KS), little is known about HIV-associated KS in the African setting, particularly among women. A descriptive study of the demographic, clinical, immunological and virological features of AIDS-associated KS from KwaZulu-Natal, South Africa was undertaken. Consecutively, recruited patients were clinically staged; CD4/CD8 cell counts, HIV-1 viral loads and clinical parameters were evaluated. Of the 152 patients (77 male and 75 female) 99% were black. Females were significantly younger (P = 0.02) and had poorer disease prognosis (odds ratio [OR] = 2.7, 95% confidence interval [CI] = 1.4-5.4, P = 0.003) and were more likely to have extensive cutaneous KS when compared with males (OR = 3.1, 95% CI = 1.4-6.7, P = 0.003). One-third of patients had coexisting HIV-related disease, most commonly tuberculosis, and these were more frequent in females (56.7 vs. 43.3%). In conclusion, HIV-associated KS in South Africans has an equal female-to-male ratio. Females are younger and have more severe disease than males.
Introduction
Services for the treatment and care of HIV-1 in Africa are being scaled-up as a result of the renewed global commitment to control the AIDS pandemic. Simple, affordable approaches are needed to identify those patients who are most likely to benefit from these intervention efforts. In South Africa, patients with Kaposi's sarcoma (KS), an AIDS-defining disease, are eligible for antiretroviral therapy (ART) and, because of the highly visible nature of their skin lesions, can be easily diagnosed, referred and enrolled into the national treatment programme. However, most of our knowledge about the clinical presentation, pathogenesis and therapeutic response of KS is based on studies conducted in men and in other geographic settings. This is because of the fact that, before the emergence of HIV-1/AIDS, KS was primarily a disease affecting men in countries around the Mediterranean (Italy, Greece, Middle East) and in specific regions of sub-Saharan Africa, including the Rift Valley and a narrow belt of land extending westward from Uganda to Cameroon. 1 3 In addition, in the first decades of the AIDS epidemic in developed countries, KS was described predominantly in men who had sex with men.
In sub-Saharan Africa, where the seroprevalence of human herpes virus (HHV)-8 (the causative agent of KS) is similar in men and women,1,4 and where the AIDS epidemic has been expanding at an alarming rate,5,6 the dynamics of KS disease and its geographic distribution, have changed dramatically over the past 10-15 years. In countries with longstanding AIDS epidemic such as Uganda and Zimbabwe, the incidence of KS has increased 20-fold to become the most common cancer in men and the second most common in women. 7 9 In South Africa, before 1993, approximately 100 new cases of histologically diagnosed KS cases were reported to the National Cancer Registry each year 10 with KS accounting for 0.3% of female and 0.7% of male cancer patients. 4 Since 1993, the incidence of KS in South Africa has doubled in men and increased seven-fold in women, in association with a corresponding decline in the male-to-female ratio from 7:1 in 1988 to 2:1 in 1996.1,4 Despite this major shift in gender, few studies have examined the clinical and biological characteristics of AIDS/KS, particularly in women. With the exception of two recent reports, one from Zimbabwe and the other from South Africa,11,12 most studies of female KS have been conducted in the US and Europe in intravenous drug users, or in female partners of bisexual men. 13 15 At present, little is known about KS in African women with heterosexually acquired HIV-1, or about the factors fuelling the rapid expansion of AIDS/KS in sub-Saharan Africa.
KwaZulu-Natal (KZN) has the highest HIV-1 prevalence and incidence rates in South Africa with an estimated 1.8 million cases and an antenatal HIV-1 seroprevalence rate of 39.1%. 6 Adult seroprevalence rates for HHV-8, the causative agent of KS, have ranged from 38% to 75%, with the majority of seropositive persons being co-infected with HIV-1. 16 Dual infection with HIV-1 and HHV-8 increases the risk of tumour development. As a result, approximately 50% of dually infected patients develop KS within 10 years. 17 To better understand the rapidly emerging AIDS/KS epidemic in sub-Saharan Africa and its gender-related differences, we conducted a comprehensive study of the clinical, virological and immunological characteristics of the disease among 152 highly active antiretroviral therapy-naïve, KS-treatment-naïve men (n = 77) and women (n = 75) from KZN. The study serves as a baseline prior to the introduction of ART, and provides essential data on the demographic and clinical patterns of AIDS/KS in a region with a high prevalence of HIV-1/HHV-8 co-infections.
Methods
The study was a cross-sectional analysis conducted over a period of one year from January to December 2002. Consecutively, patients recruited with AIDS/KS to the Dermatology Unit at King Edward VIII Hospital in Durban, KZN were seen and evaluated. Following voluntary counselling, consenting patients with biopsy-proven KS were tested for HIV-1. Those who were seropositive were assessed for: demographic data (age, gender, race), route of HIV-1 transmission, clinical staging of KS into good and poor prognosis categories according to AIDS Clinical Trial Group (ACTG) criteria, 18 presence of other co-morbid conditions, blood count, renal and liver function tests, CD4+ and CD8+ T-cell counts and HIV-1 viral loads (VL). The ACTG system uses clinical criteria, CD4 count and systemic symptoms to stage patients. Cutaneous disease was categorized as localized or generalized. KS lesions confined to one anatomical area were classified as local and lesions involving two or more sites as disseminated or extensive. 19 Visceral disease was assessed by endoscopy and bronchoscopy in symptomatic patients only. The study was approved by the Ethics Committee of Nelson R Mandela School of Medicine.
HIV-1 antibody testing was performed using the Nuclisens Vironostika Improved Kit (Organon Teknika, Boxtel, Netherlands). CD4+ and CD8+ T-cell counts were performed on a Coulter XL Flow Cytometer using a single platform Beckman Coulter TetraOne protocol. HIV-1 VLs were measured using the Nuclisens HIV-1 QT kit.
Data were entered into Epi-Info (version 6.04d) (CDC, Atlanta, USA) and analysed using Stata version 8 (Stata Corporation, TX, USA). Analyses included χ2 tests to determine associations between opportunistic infections, demographic, virological (VL) and immunological markers between males and females. A χ2 test for trend was conducted to investigate the relationship between degree of immune suppression and gender.
Results
A total of 152 African patients (151 black, 1 white) with HIV-1 KS were evaluated. With the exception of a single homosexual man infected with subtype B, all patients were infected with HIV-1 subtype C and all reported of having acquired their HIV-1 through heterosexual contact. No patient had been previously treated with ART. The ratio of male (n = 77) -to-female patients (n = 75) was 1:1, with women being significantly younger (mean age of 34, standard deviation [SD] = 8.86) than men (mean age 37, SD = 7.94) (P = 0.02) (Table 1). Age group distribution patterns (Table 2) indicated that the number and proportion of AIDS/KS cases in young women <25 years of age were substantially higher than those observed for men in the same age group (n = 9 (81.8%) for women; n = 2 (18.2%) for men) (Figure 1). Compared with men, AIDS/KS was also more common among young women of 26-30 and 31-35 years of age (57.9% vs. 42.1% and 52.8% vs. 47.2%, respectively). These changes were associated with a shift in the female-to-male sex ratio from 4.5:1.0 in patients <25 years of age to 0.4:1.0 in patients between the ages of 45 and 50 years. In contrast, in the older age groups (36-40, 41-45 and 46-50 years), the number and proportion of KS cases among HIV-1-infected men outnumbered those in women. As shown in Figure 1, the proportion of KS cases increased from 12.0% (n = 9) in women <25 years of age to a peak level of 29.3% (n = 22) in women between the ages 26 and 30 years. Thereafter, there was a gradual decline in the number and relative percentage of KS to levels of 25.3% (n = 19), 16.0% (n = 12), 6.6% (n = 5), 4.0% (n = 3) in women aged 31-35, 36-40, 41-45 and 45-50 years of age, respectively. In men, the proportion of AIDS/KS cases increased progressively with age from 2.6% in men <25 years of age to 24.7% in men between the ages of 36 and 40 years, and then declined thereafter. In addition to presenting with KS at an earlier age, women had more severe clinical manifestations and a poorer prognosis when compared with HIV-infected men with KS (Table 3). When classified into ‘good’ and ‘poor’ risk groups using the ACTG clinical staging system for KS, 63.6% of women and only 36.4% of men were found to have a ‘poor’ disease prognosis (odds ratio [OR] = 2.7, 95% confidence interval [CI] = 1.4-5.4, P = 0.003). This finding applied to essentially all age groups. As shown in Figure 2, more women in age groups 26-30, 31-35, 36-40 and >41 years had a poor prognosis when compared with men of the same age. Women also had more disseminated cutaneous KS lesions involving an increased number of lesions at multiple anatomical sites, while the lesions in men were more localized (OR = 3.1, 95% CI = 1.4-6.7), P = 0.003]. Overall, 37 (24.3%) patients (19 [51.4%] male; 18 [48.6%] female) had visceral lesions in either the lung or gastrointestinal tract (Table 3). The mean peripheral blood CD4+ T-cell count for the entire cohort (available for 145 patients) was 218 cells/mm3 (range: 1-1406, 95%CI = 181-253). Despite the observed differences in age, disease severity and prognosis, no gender-specific differences were observed in CD4+ T-cell counts, CD8+ T-cell counts or plasma HIV-1 VL. Males had a mean of 230 cells/mm3 (range: 8-875, 95% CI = 191-268) and women, 205 cells/mm3 (range: 1-1406, 95% CI = 142-267) (P = 0.49). The mean CD8+ T-cell counts were also similar for the two groups: 1250 cells/mm3 (range: 154-3686, 95% CI = 1071-1430) for males and 1129 cells/mm3 (range: 130-4699, 95% CI = 942-1316) for females (Table 1). Similarly, there was no significant association between gender and differences in log10 HIV-1 VL (P = 0.46). The mean HIV-1 VL for the entire cohort was 5.08 log10 (range: 3.43-6.34, 95% CI = 4.98-5.18) when compared with 5.07 log10 (range: 3.67-6.04, 95% CI = 4.93-5.21) and 5.1 log10 (range: 3.43-6.34, 95% CI = 4.94-5.25) copies/mL of plasma for males and females, respectively. Statistical analyses, performed separately within each group, revealed significant correlations between the severity of KS and the degree of immune suppression as measured by CD4+ T-cell levels (χ2 test, P < 0.001) and between poor disease prognosis (as determined by ACTG staging) and immune suppression. The latter relationship was highly significant (P < 0.0001) and linear in nature, and when controlled for gender using a Mantel-Haenszel test, was found to be stronger among females when compared with males (OR = 0.18, 95% CI = 0.1-0.3, P < 0.001). Females with poor prognosis were more likely to have CD4+ T-cell count <200 cells/mm3 when compared with males (OR = 2.2, 95% CI = 1.0-4.20, P = 0.03). A comparison of the severity of KS lesions indicated that females had more extensive cutaneous disease when compared with males (OR = 3.1, 95% CI = 1.4-6.7, P = 0.003) (Table 3).
Patient characteristics and clinical information
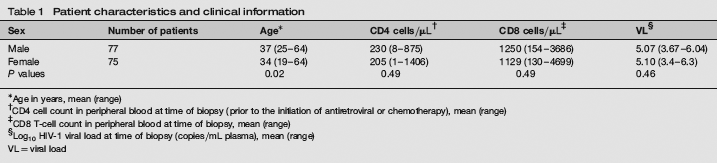
Age in years, mean (range)
CD4 cell count in peripheral blood at time of biopsy (prior to the initiation of antiretroviral or chemotherapy), mean (range)
CD8 T-cell count in peripheral blood at time of biopsy, mean (range)
Log10 HIV-1 viral load at time of biopsy (copies/mL plasma), mean (range)
VL = viral load
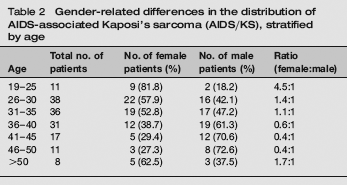
Gender-related differences in the distribution of AIDS-associated Kaposi's sarcoma (AIDS/KS), stratified by age
Gender-related differences in the clinical presentation of AIDS-associated Kaposi's sarcoma (AIDS/KS) (n = 152)
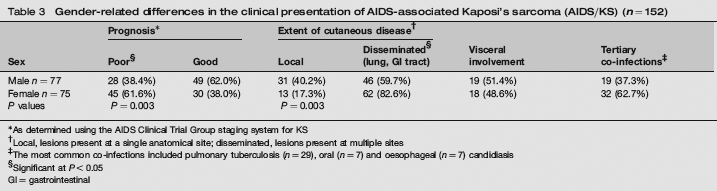
As determined using the AIDS Clinical Trial Group staging system for KS
Local, lesions present at a single anatomical site; disseminated, lesions present at multiple sites
The most common co-infections included pulmonary tuberculosis (n = 29), oral (n = 7) and oesophageal (n = 7) candidiasis
Significant at P < 0.05
GI = gastrointestinal

Age distribution of AIDS-associated Kaposi's sarcoma (AIDS/KS) stratified by gender, expressed as a percent of the number of males (n = 77) and females (n = 75) studied. Women under the age of 35 accounted for 30.8% of all HIV-1/KS cases. In addition to being present in young women in their late teens and early 20s, KS was also clearly present among women in their late-20s and early to late-30s, with peak prevalence occurring in women from 26 to 30 years of age. In men, AIDS/KS was most prevalent among males between the ages of 36 and 40

Number of AIDS-associated Kaposi's sarcoma (AIDS/KS) patients with good versus poor disease prognosis, stratified by age and gender. The majority of women across all age groups (excluding women aged 19-25) had a ‘poor’ disease prognosis, while the majority of men with AIDS/KS were classified as having a ‘good’ prognosis as defined by the AIDS Clinical Trial Group clinical staging system
Fifty-one patients (33.6%) had concurrent co-infections. These tertiary infections were more common in females [n = 32 (62.7%)] when compared with males [n = 19 (37.3%)] (Table 3). Tuberculosis (TB) was the commonest, present in 30 (19.7%). Of those with TB, 17 (56.7%) were female and 13 (43.3%) male. This was followed by oral candidiasis in seven (4.6%) and oesophageal candidiasis in another seven patients (4.6%). With the exception of a TB patient with papulonecrotic tuberculid, all of the remaining TB patients (n = 29) had pulmonary TB.
Discussion
This study provides a detailed description of the clinical, virological and immunological characteristics of AIDS/KS in a population of ART-naïve men and women from South Africa. Our study differs from previous North American and European studies in several important ways including, the high proportion of females, the route of transmission (heterosexual vs. parentral), the subtype of HIV-1 (C vs. B) and the high versus low prevalence of concurrent tertiary infections such as TB 20 and candidiasis. Our study also measured the extent of KS disease directly (level of cutaneous and visceral involvement), rather than relying on the reporting of nonspecific symptoms such as fever, diaphoresis, weight loss, etc. 11
The proportion of women with HIV-1-related KS (ratio of 1:1) was substantially higher that that reported for American, European and other African population groups. 11 16 In a recent study of 107 HIV-1-infected patients from Brazil, for example, men still accounted for 94.4% of all KS cases (ratio of 18:1). 21 Studies from Tanzania reported a disproportionate increase in female KS cases, and a shift in the male-to-female ratio from 4:1 pre-AIDS to 1.6:1.0 in the interval between 1990 and 1992. 22 In contrast to AIDS/KS, endemic KS in Tanzania continues to be a male-dominated disease with 100% of cases occurring in men. 23 A sex ratio of 3:1 was recently reported in Zimbabwe, 11 a country that has experienced a 20-fold increase in KS, and a ratio of 2.8:1 was reported in a study from South Africa published in 2000. 24 The reason for the near equivalent distribution of KS cases among men and women in our study is not known, but may be a reflection of the fact that our study was conducted at a slightly later time point (2002) when the incidence of female KS had increased even further. Also of note, is the fact that the prevalence and incidence of HIV-1 in KZN are among the highest in sub-Saharan Africa, with young women bearing the major impact of the burden. 25 Finally, as this was not a population-based study, there may have been a referral bias favouring women being referred and seen in the Dermatology Clinic. If this does represent a broader trend, it may lead, ultimately, to a reversal in the AIDS/KS gender ratio, with a predominance of females.
Of equal importance was the unequal distribution of AIDS/KS among different age groups. The finding that KS occurs at an earlier age in women when compared with men has been reported previously in smaller retrospective studies in Europe and the USA.13,14 Our studies, showing that the proportion of AIDS/KS cases was highest among women in their mid-20s, confirms and expands this knowledge to include young African women with heterosexually acquired subtype C HIV-1 infection. Also of considerable interest was the finding that the age-specific distribution pattern for female KS was essentially identical to that previously reported for HIV-1, on its own. In past studies conducted in KZN, the prevalence (and incidence) of HIV-1 increased in young mothers between the ages of 21 and 25, and then levelled off and declined thereafter, in women >30 years of age. 25 Taken together, these data suggest that the risk of developing female KS, at least in KZN, is closely related to the epidemiology (and/or transmission) patterns of HIV-1.
The finding that, at diagnosis, women had more extensive KS disease is consistent with studies from Zimbabwe and Italy showing that women with AIDS/KS are more symptomatic, 11 have more advanced disease and a more aggressive clinical presentation and disease course 14 relative to men. The reason for the increased severity of KS in HIV-1-infected women is not known, but does not appear to be related to virological or immunological differences since the men and women in our study had similar mean VL and mean CD4+ T-cell counts. The lack of a gender-related correlation between disease severity and CD4+ T-cell count is in agreement with the Zimbabwean study 11 but at variance with the data from Italy. Italian investigators found that, relative to men, women with KS were more immune-deficient. 14 Despite the lack of a difference between men and women, we found that within each gender group, there was a statistically significant relationship between lower CD4+ T-cell counts and more advanced KS disease, and between lower CD4+ T-cell counts and poor disease prognosis, suggesting that immune suppression may play a role in KS progression, but that this role may not necessarily be gender-related. Carefully designed longitudinal studies are needed to define more clearly the relationships between gender, immune suppression and clinical disease.
The wide variation in CD4+ T-cells counts observed in our study (from 1 to 1406 cells/mm3) and the finding that 21% of patients had CD4+ T-cell levels >350 cells/mm3 (38% >200 cells/mm3) suggests that, as previously reported,12,26 in African populations, severe immune suppression is not a prerequisite for the development of KS lesions. Although the reasons are not known, higher than expected CD4+ T-cell counts in African patients has been reported previously. 27 In Uganda, investigators found that, despite having a higher mean CD4+ T-cell relative to patients in the USA and Europe 28 31 African patients with an AIDS-defining condition had a shorter survival time.
Whether the differences observed among different studies are because of variation in treatment, chronic immune stimulation, route and timing of transmission and/or viral subtypes among different population groups remains to be established.
Additional studies are needed to better understand the factors contributing to the rapidly emerging AIDS/KS epidemic in sub-Saharan Africa, including the role of female sex hormones 32 and parity 33 in promoting AIDS/KS pathogenesis. Such studies may have important implications, not only for the prevention and treatment of KS in young women (and men), but also for the timing, monitoring and assessment of these interventions and for policy and decision-making. As previously reported, in the African setting, great care must be taken to accurately diagnose and differentiate between KS- and TB-induced pulmonary diseases. 34 Given that TB may coexist with AIDS/KS in 20% of patients, and that the diagnosis of this condition may influence both the timing and choice of ART, it is recommended that all AIDS/KS patients receive a clinical evaluation and sputum examination for the detection of acid-fast bacilli, and that those with symptomatic lung disease be ruled out for TB.
One of the limitations of our study is that it was an analysis of a convenience sample of a clinic population and might not represent the more generalized population of patients with HIV disease and KS in South Africa. The study design limits comments of prevalence and incidence of KS. However, this limitation does not detract from the main finding that women younger than 26 years of age appear to bear a substantial burden of both the AIDS and the KS epidemics in South Africa. To more precisely estimate this and more fully understand the relationship of ACTG clinical staging, immunosuppression and outcome, carefully designed population-based longitudinal studies will be needed.
In summary, our observations strengthen and extend previous studies regarding the changing dynamics of AIDS-KS in Africa. The study highlights special attributes of female KS, including younger age at diagnosis, apparent more aggressive disease course and co-morbidities and finally draws attention to the urgent need to intensify efforts aimed to preventing transmission of HIV to young women, if we are to successfully control HIV-1/AIDS and AIDS/KS in sub-Saharan Africa.
Footnotes
Acknowledgements
This work was supported by a Dermatological Society of South Africa Research Grant, Wellcome Trust Grant 061238, NRF Thuthuka Grant GUN 2054349 and an ACRiA Grant