
Abstract
This case report documents that highly active antiretroviral therapy (HAART) can lead to the regression of Kaposi's sarcoma (KS) lesions in the auditory canal of an HIV-infected male from Chennai, India. In resource-limited settings where administering anti-KS chemotherapeutic agents may not be feasible, HAART alone can be an option in HIV-infected individuals with KS.
Keywords
INTRODUCTION
Although the incidence of Kaposi's sarcoma (KS) has dramatically decreased since the 1980s, 1 it has remained the most common AIDS-related malignancy since the beginning of the HIV/AIDS pandemic. 2 Highly active antiretroviral therapy (HAART), has been shown to lead to KS regression. 3–5 Although the factors that lead to AIDS-associated KS growth are not fully understood, it is probably most likely in patients with depleted CD4+ levels, 1 high viral load and uncontrolled herpes virus 8 viraemia. This case report documents that HAART alone can lead to the regression of KS lesions in the left auditory canal of a HIV-infected male from Chennai, India.
CASE REPORT
A 30-year-old HIV-infected male presented to the clinic with blurring vision, cough, fever, papular lesions over the face and with a mass lesion in the left auditory canal (Figure 1).

Left auditory canal prior to HAART with Kaposi's sarcoma lesions and Molluscum contagiosum
He was subsequently investigated in the clinic and diagnosed with pulmonary tuberculosis, molluscum contagiosum over the face and cytomegalovirus (CMV) retinitis on the left eye. At the time of presentation, his CD4+ cell count was 10 cells/μL; weight 46 kg. A biopsy was taken from the left ear by the clinic's ENT consultant and sent for histopathological examination, which showed proliferation of spindle-shaped vascular epithelium consistent with KS (Figures 2 and 3).
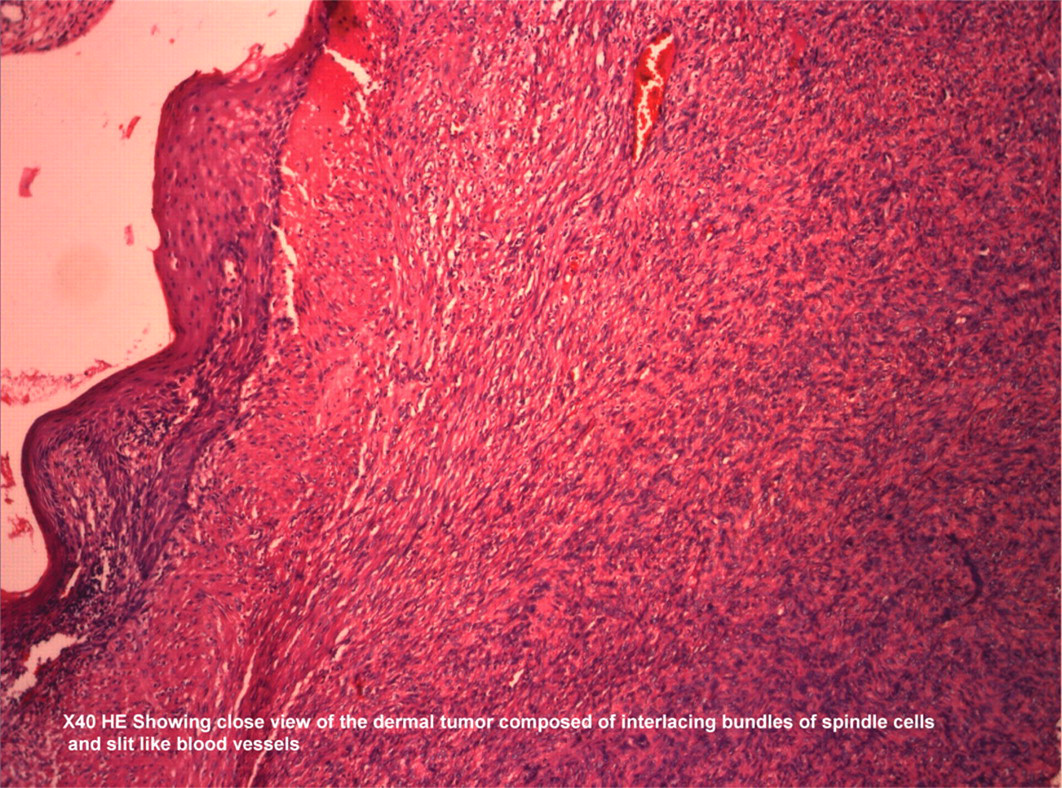
Histopathological slide composed of interlacing bundles of spindle cells

Histopathological slide consisting of spindle cells of nodular Kaposi's sarcoma
The patient was initiated on antituberculosis therapy (ATT) for his pulmonary tuberculosis, ganciclovir for his CMV retinitis and cryotherapy over the face for molluscum contagiosum. Subsequently, he was initiated on HAART consisting of two nucleoside reverse transcriptase drugs, lamivudine (3TC) and stavudine (d4T), and one non-nucleoside reverse transcriptase drug, efavirenz.
The patient's clinical symptoms subsequently improved after initiating treatment. The lesions over his face regressed. However, as a result of immune reconstitution following the initiation of HAART, he developed immune reconstitution vitritis (IRV) in the left eye. The patient continued on HAART and his CD4+ cell count after three months rose to 316 cells/μL with a weight gain of over 20 kg to 74.7 kg. Follow-up examination of his auditory canal showed thorough regression of the KS lesions in the left auditory canal (Figure 4). This finding was additionally confirmed via computed tomography. The patient continued on HAART and CD4 count increased to 510 cells/μL. Upon further follow-up, the lesions completely regressed. The patient remains on close follow-up to date.

Regression of Kaposi's sarcoma lesions in the left auditory canal following HAART
DISCUSSION
We report on an interesting case of KS regression in the auditory canal of an HIV-infected Indian male after initiation of antiretroviral therapy. KS was first reported among HIV-infected Indian patients in the mid-1990s in two case reports from Chennai and Mumbai. 6,7 In the era of HAART, studies have documented the regression of KS following the initiation of HAART. 3–5 This case report highlights that HAART can independently prevent the progression of malignancies like KS in patients symptomatic with HIV.
The introduction of HAART has led to dramatic reductions in morbidity and mortality due to HIV both in resource-limited settings. 8 This case highlights that HAART can lead to the regression of AIDS-associated KS. Paclitaxel, a common chemotherapeutic agent used either alone or in combination with other medications for AIDS-associated KS, can have potentially dangerous drug–drug interactions with various components of HAART regimens, leading to potentially life-threatening toxicities. 9 In resource-limited settings, methods of KS treatment, including radiotherapy, chemotherapeutic agents and biological response-modifiers (such as INF-α) are not widely accessible. However, when life-threatening visceral or cerebral lesions are present, there are no substitutes for chemotherapeutics, which highlights the need for an expanded treatment formulary in resource-limited settings.
This patient with severe immune suppression due to HIV presented with multiple opportunistic infections and later improved with appropriate opportunistic infection therapeutic management. This patient who never received therapy specifically targeted at his auditory KS, had a thorough regression of his lesions following HAART. Lower CD4 count has been associated with the development of KS. 1 His immunological recovery was evident in his increased CD4 cell count. However, he later developed IRV due to the immune reconstitution following HAART. Some HIV-infected individuals experience clinical deterioration after initiating antiretroviral therapy that is believed to be a result of the restored immune system to mount an exuberant inflammatory response.
Although HAART has been shown to lead to the regression of KS, most of these studies have involved protease inhibitor-based therapy. 3,4 A case report from an African setting documented a patient initiated on two NRTI and one NNRTI-based HAART, who then had complete AIDS-associated KS remission. 10 A more recent study has documented that HAART leads to the remission of AIDS-associated KS independent of protease inhibitor-based therapy regimens. 5 In resource-limited settings, antiretroviral strategies with combinations of nucleoside analogues and non-nucleoside inhibitors of HIV reverse-transcriptase are generally used, with protease inhibitor (PI) therapy being saved for second-line regimens. This case report provides further evidence that non-PI containing HAART regimens can be effective in leading to complete AIDS-associated KS regression.
Footnotes
ACKNOWLEDGEMENTS
The authors thank Dr Srinivas, pathologist, and all the clinical staff at the YRG Centre for AIDS Research and Education, VHS, Chennai, India, for facilitating their study.