
Abstract
Summary
An HIV-infected man receiving antiretroviral therapy—who also had lupus-like vasculitis and membranous glomerulonephritis (treated with prednisolone and azathioprine), beta-thalassaemia minor trait and post-radiotherapy functional asplenia (mimicking sickle cell disease-induced hyposplenism)—developed focal soft issue and bone infection caused by Salmonella enteritidis at the site of previous mycobacterial infection.
INTRODUCTION
Recurrent bacteraemia is an AIDS-defining illness. Salmonella enteritidis and S. typhimurium are the two most common serotypes of Salmonella spp. infection causing bacteraemia in patients with HIV infection. 1,2 Localization of infection following Salmonella spp. bacteraemia develops in 5–10% of patients 3 and in HIV-infected patients may occur without preceding/coincidental gastrointestinal symptoms. 4 In the HIV-infected individual local non-typhoid Salmonella spp. infection can involve any organ system. Soft tissue infection, including pyomyositis, psoas abscess and abscesses at the site of intravenous injection 3,5–7 , arthritis and osteomyelitis involving the parietal bone have been reported. 3,8 We describe an HIV-infected patient with S. enteritidis focal infection arising at the site of previous mycobacterial infection. In addition to underlying HIV infection the patient had multiple other risk factors for non-typhoidal Salmonella spp. infection.
CASE REPORT
A 44-year-old man presented with a swelling at the left anterior border of the sternum. Ziehl–Neelsen staining of a percutaneous needle biopsy of the tissue mass showed scanty acid and alcohol-fast bacilli (AAFB) and granulomata. The patient had long-standing HIV infection and seven years previously he had received splenic radiotherapy as treatment for refractory immune thrombocytopenia. Highly active antiretroviral treatment had been commenced six years ago; on an antiretroviral regimen of lopinavir/ritonavir, efavirenz and emtricitabine. The HIV viral load (VL) was undetectable and the CD4 count fluctuated between 60 and 160 cells/mm3. In addition, the patient had hepatitis C infection and biopsy-confirmed lupus-like vasculitis with membranous glomerulonephritis; the latter diagnoses requiring long-term prednisolone (30 mg/day) and azathioprine. The patient also had beta-thalassaemia minor trait.
After completing six months of directly observed antituberculosis treatment the patient represented with a two-week history of a gradually enlarging sternal swelling at the same anatomical site. There was no history of recent trauma, fever, gastrointestinal or systemic upset. On examination, the patient was apyrexial; there was a 3 × 3 cm fluctuant mass at the lower left sternal border without overlying skin change, or regional lymphadenopathy and without signs of active lupus. A chest radiograph was normal, as was the full blood count, renal and liver function tests and C-reactive protein; the CD4 count was 60 cells/mm3 (9.1% of total lymphocyte count) and the HIV VL was undetectable. Blood, stool and urine cultures were all negative for bacteria (including mycobacteria).
Thoracic magnetic resonance imaging showed a soft tissue collection lying anterolateral to the left of the sternum, extending into the costochondral junction. A small focus of osteomyelitis was noted (Figure 1). Histological examination of samples obtained by ultrasound-guided aspiration and biopsy of the collection showed granulation tissue: staining for AAFB and fungi was negative. Warthin–Starry staining identified a collection of bacilliform organisms (Figure 2). Culture of the aspirate grew S. enteritidis, sensitive to fluoroquinolones. After treatment with oral ciprofloxacin of 750 mg twice a day for six weeks there was resolution of the mass. The patient remained on long-term prophylaxis with ciprofloxacin.
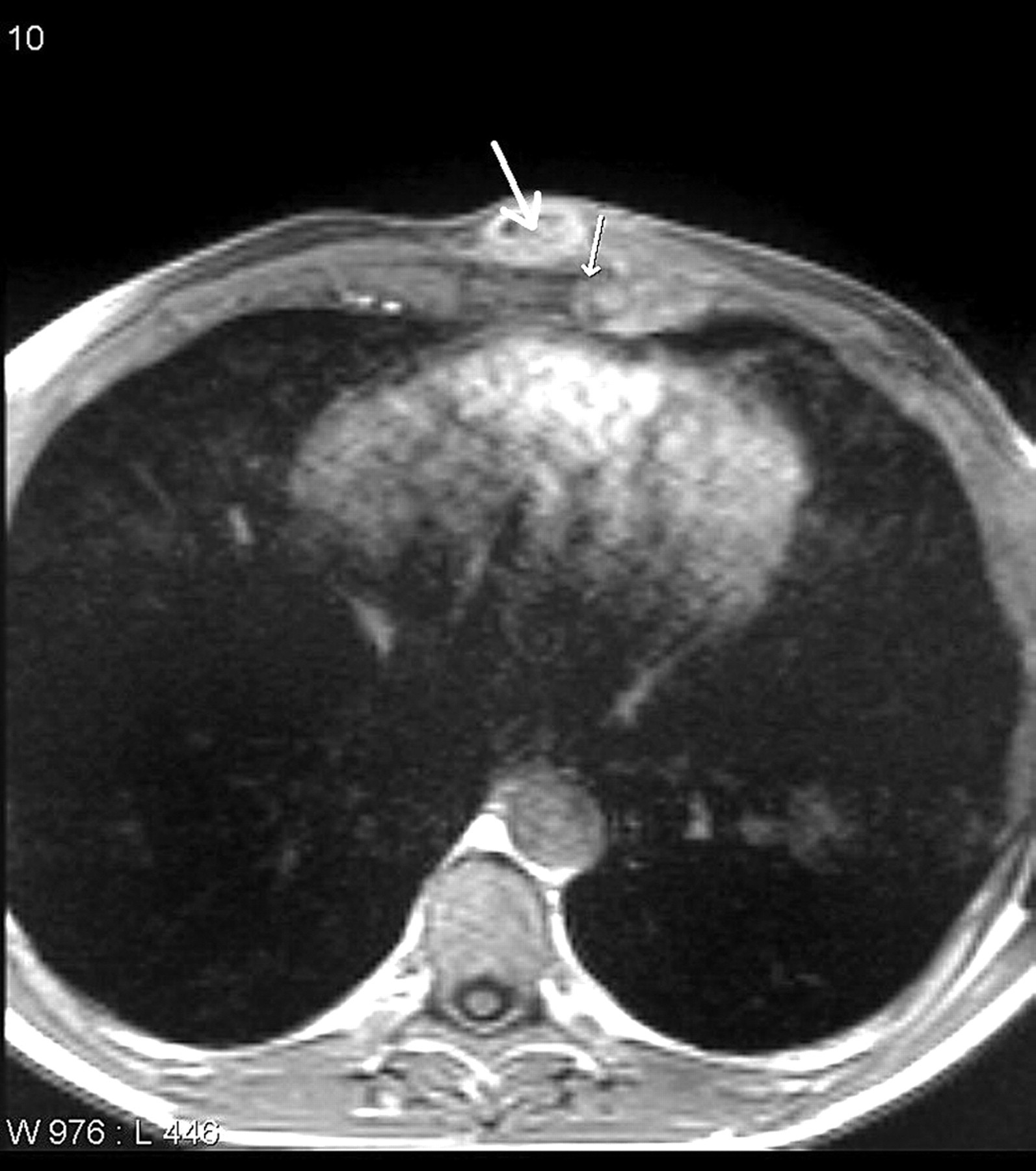
T1-weighted axial gadolinium-enhanced magnetic resonance imaging scan of thorax. There is an ovoid collection of pus (thick arrow) lying anterolaterally to the sternum and extending to the costochondral junction. There is a focus of osteomyelitis lying deep to the collection (thin arrow)
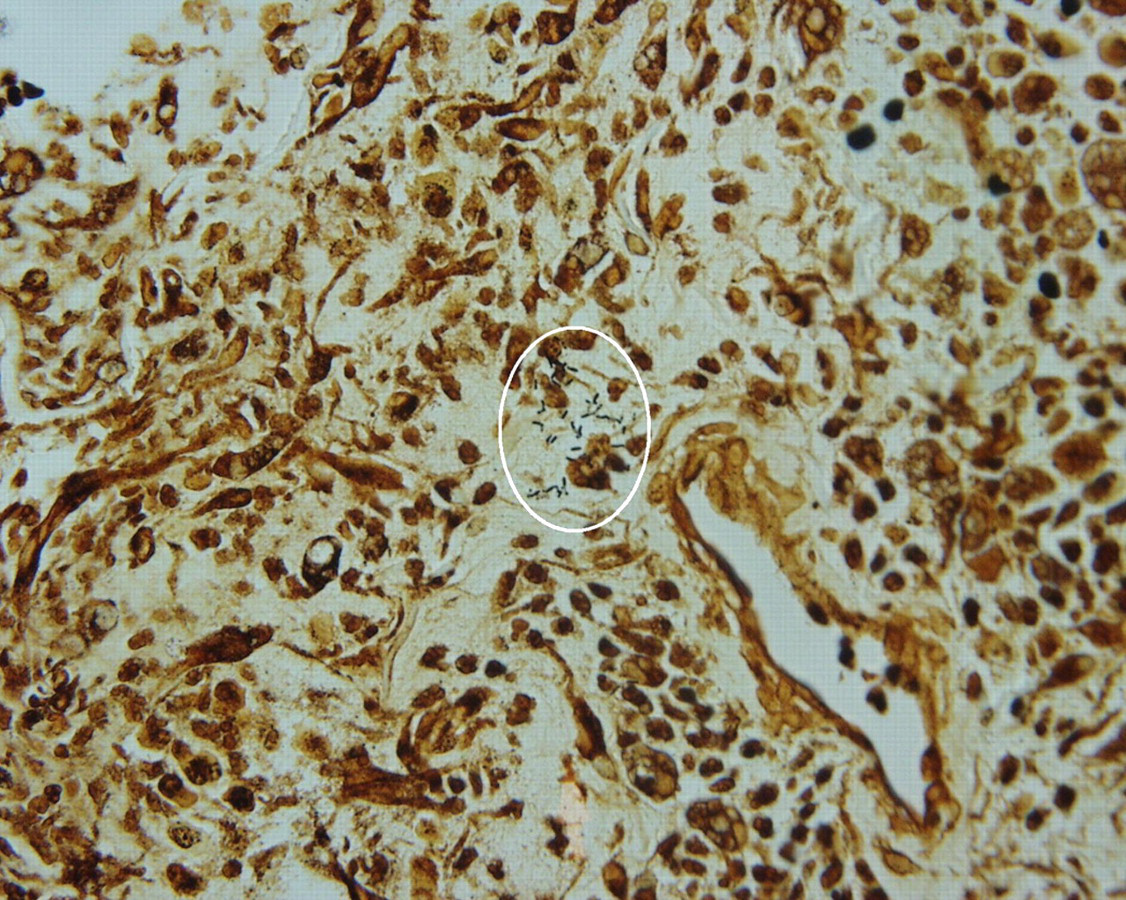
Biopsy of sternal mass. Warthin–Starry stain; original magnification × 40. There is a focus of bacilliform organisms (circled)
DISCUSSION
This patient who presented with focal S. enteritidis infection in soft tissue and bone in the context of HIV infection 3,5 had several unique features, as additional immunosuppression induced by lupus-like syndrome 9 and its treatment, functional asplenia secondary to radiotherapy (mimicking sickle cell disease-induced hyposplenism) 10 and underlying beta-thalassaemia traits were present. 11 In this patient, these disparate factors contributed to defective cell-mediated immunity. As a consequence there was impaired ability to contain and eradicate Salmonella spp. infection.
Salmonella spp. are able to survive and replicate within macrophages and this crucial attribute allows them to disseminate within the human host. 12 Previous trauma is a well-recognized predisposing factor for localization of Salmonella spp. infection. 5 As granulomata and granulation tissue contain numerous macrophages, we postulate that in our patient S. enteritidis-infected macrophages were preferentially recruited to the site of the previous sternal mycobacterial granulomatous infection, where subsequently clinically-apparent infection was established.
This case has several important messages for clinicians caring for HIV-infected individuals. First, it serves to underscore the importance of using multiple imaging modalities in order to localize infection in the immunosuppressed HIV-infected patient. Secondly, it demonstrates the importance of including general medical causes of immunosuppression and their treatment in the differential diagnosis and aetio-pathogenesis of HIV-infected patients with unusual clinical presentations. Thirdly, it demonstrates the importance of identifying a specific aetiology, so that targeted antimicrobials may be used in patients with HIV infection, minimizing the risk of empirical therapy causing complex drug–drug interactions with antiretroviral therapy. 2 Finally, the case highlights the need for long-term antibiotic prophylaxis in this patient group. 1