
Abstract
HIV-positive women may be reluctant to attend gynaecology or family planning clinics for fear of divulging their condition. Therefore, a referral clinic was opened within the HIV clinic. Retrospective case-note reviews of 197 new patients revealed 109 with a variety of medical gynaecology conditions (menorrhagia being the commonest) and 88 sought contraception. The full range of contraceptives was used, including Mirena for the treatment of menorrhagia as well as contraception and the combined pill adjusted for interaction with liver enzyme-inducing antiretroviral drugs. The acceptance of contraceptive advice and gynaecological evaluation by the patients has resulted in improved reproductive health services for these HIV-positive women. In centres with large cohorts of HIV-positive women, this type of one-stop specialist clinic will be very effective in providing high-quality reproductive health care and hence, this type of clinic is recommended for such centres.
Keywords
Introduction
World Health Organization estimates that 50% of all adult HIV infections are in women; they are predominantly infected by heterosexual transmission. There may also be a trend towards multiple infections with sexually transmitted infections (STIs). In London as a whole, the highest incidence of HIV and other STIs (judged by statistics from GU medicine clinics) is in south London. Among the patients seen in our clinic over the last 10 years, there have been 1166 HIV-positive women of whom 954 were in the reproductive age groups. Of these, 300 were pregnant. At least 12 pregnancies were unplanned and were terminated. The majority were Black African. The HIV-infected women may avoid attending contraception or gynaecology clinics for fear of divulging their condition. But if their condition is not divulged, subsequent management may be compromised.
Therefore, we set up a specialist dedicated Family Planning and Medical Gynaecology Referral Clinic in the HIV clinic aiming to serve these women in a one-stop clinic to improve their reproductive and sexual health.
Objective
To identify their gynaecological problems; To identify the contraception methods suitable for these women; To assess the improvement in their reproductive health care.
Method
A retrospective case-note review of all patients evaluated between 1 September 2004 and 31 July 2007.
Results
A total of 197 patients attended, some required both gynaecology and contraceptive measures. Ages ranged from 14 to 52 years (mean 31 years). The majority were Black Africans (para 0-3). They were at various stages of HIV infection and treatment, with the CD4 count of 47-1132 (mean 476).
One hundred and nine patients had gynaecological problems, 35 menorrhagia, seven vulval lumps, two endometriosis, five fertility issues, one vaginal cyst, three genital ulcers, 12 fibroid uterus, five adenomyosis, 12 amenorrhoea, three recurrent vaginal discharge, two polycystic ovary syndrome (PCO), seven pelvic inflammatory disease, three vulval intraepithelial neoplasia (VIN) and 12 others (Figure 1). Of the nine endometrial biopsies, all were normal except for one complex endometrial hyperplasia.
Gynaecological conditions identified PCO = polycystic ovary syndrome; PID = pelvic inflammatory disease; VIN = vulval intraepithelial neoplasia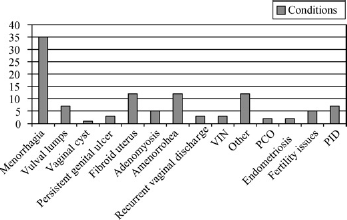
Eighty-eight patients sought contraception. Eighteen opted for intrauterine devices (IUDs), 23 Mirena, 12 Depo-Provera, seven barrier methods, 13 combined oral contraceptive pill (COC), two tricycling pill, five implanon, four sterilization and four cerazette (Figure 2).
Pie diagram depicting the different methods chosen IUD = intrauterine device; COC = combined oral contraceptive pill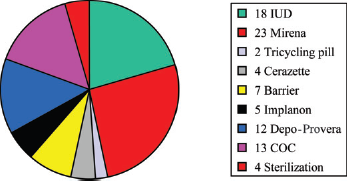
Uptake of the service was 100% and immediate. This clearly indicates improved reproductive health care for these HIV-positive women.
Discussion
Considerations in the management of patients who do not wish to conceive include the stage of HIV infection, CD4 count, liver enzyme-inducing drugs, family wishes, pill burden and adherence, concomitant diseases, osteoporosis risk and cultural considerations. Treatments for reproductive health needs may interact with HIV management.
Contraception
In our HIV population, IUDs (Copper T and Mirena) are very acceptable and are adopted by the majority of patients. Both are effective in women on highly active antiretroviral therapy (HAART). IUDs may be considered for the majority of patients and may be extremely beneficial because of reduced pill burden and instant reversibility. Mirena also reduces bleeding in those with painful and heavy periods and is thought to be effective with liver enzyme-inducing products. 1 Depo-provera was the second commonest. This product is thought to cause some reduction in bone mineral density as does HIV and its treatment. Patients to be given this treatment should be chosen carefully and need follow-up. Where a family is complete, permanent methods (for the male, vasectomy and for the female, sterilization) are appropriate.
The major issue with the use of combined oral contraceptive pill in HIV-positive patients is interaction with medications that lower the efficacy of the pill.2,3 Such patients must be advised to use condoms at all times along with the pill with double the dose or tricycling . Products such as implanon are available but their interactions with liver enzyme-inducing drugs are expected to be similar to those of the COC Postpartum, with no breast feeding, early contraception is vital.
Patients not on liver enzyme-inducing drugs can use any methods of contraception unless contraindicated for other reasons. All patients should continue with condoms to increase the efficacy of contraception, avoid disease transmission and prevent acquisition of new STIs.
Gynaecology
In our clinic, the commonest gynaecological problems have been menorrhagia, amenorrhoea, fibroid uterus and premalignant lesions of the lower genital tract. Compared with seronegative women, HIV-seropositive women are at increased risk of some menstrual changes, although the absolute frequency of most abnormalities is low. Higher CD4 counts and HAART protect against incidental abnormalities. 4 In AIDS patients, chronic illness and weight loss may cause women to become amenorrhoeic; the most common menstrual problem reported by HIV-positive women is amenorrhoea. It is more frequent among women with CD4 cell counts below 50. Probably, problems with a woman's immune system and irregularities due to HIV cause changes in her hormones resulting in menstrual problems. Vaginal candidiasis is much more common in HIV-positive women who have low T-cell counts. Lower genital tract precancerous lesions (cervical intraepithelial neoplasia [CIN] and VIN) are high in this group of women.
Conclusion
The acceptance of contraceptive advice and gynaecological evaluation by our patients attending the one-stop clinic has resulted in improved reproductive health services for our HIV-infected women.
Our experience suggests that in centres with large cohorts of HIV-positive women, this type of one-stop specialist clinic will be very effective in providing high-quality reproductive health care and hence, we recommend this type of clinic for such centres.