
Abstract
Antioxidants significantly inhibit oxidative processes. The study seeks to determine the activity of endogenous antioxidants and CD4+ T-cell expression in HIV-serodiscordant-heterosexual partners. The case-control study had the following groups; A- (13 serodiscordant-seronegative subjects), B- (13 serodiscordant-seropositive subjects) and C/control- (13 healthy volunteers). CD4+ T-cell expression was determined using a FACScan (fluorescent activated cell sorting) flow cytometer. CAT (catalase), superoxide dismutase, glutathione peroxidase (GHPX) and glutathione S-transferase (GST) activities were assayed using spectrophotometer. The activities of SOD, GHPX, GST and CAT were significantly (P < 0.05) increased by 164.7% (0.090 ± 0.032), 126% (662 + 96), 355.2% (22.023 ± 1.4) and 119.1 % (2.76 ± 0.10), respectively, in group A when compared with B. The mean CD4+ T-cell (1348 ± 142) showed a significant (P < 0.05) increase by 237% when compared with group B (400 ± 182). Conversely, group B revealed a significant (P < 0.05) decrease in activity by 86.5% (CAT), 76.5% (SOD), 106.8% (GHPX) and 81.8% (GST) when compared with C. CD4+ T-cells in groups A and C (1390 ± 190) did not show any significant decrease (3.11 %). The antioxidant activity showed a positive correlation (P < 0.01, r = 0.89) with their respective CD4+ T-cells in groups A and C. Group B showed same positive correlation (P < 0.01, r = 0.76). These results show that high activity of endogenous antioxidants may have a protective role on CD4+ T-cells, which limits HIV infection.
Introduction
There are individuals who have been exposed to HIV multiple times but who either remain uninfected or if they are infected, progress more slowly to AIDS. It is logical that differences in immune system1,2 and viral fitness3–5 may play a role in the genetic variation to HIV infection. However, none of these conclusions describe holistically the non-susceptibility of such individuals of black African origin to HIV infection. The essence of the study is to determine the implication of endogenous antioxidants in HIV-resistant individuals of black African origin.
It has been proposed that CD4+ T-cells are depleted by apoptosis. The T-cells are primed to undergo apoptosis upon cross-linking of CD4 by gp 120 (a HIV protein required for binding to target host cell), 6 subsequent activation by conventional antigens or super antigens induces apoptosis in these T-cells. Chronic oxidative stress (OS) with a constant generation of free radicals affects the immune system's fight against HIV by enhancing HIV replication through the activation of nuclear factor kappa binding (NF-kB) and genes (tumour necrosis factor [TNF]) which further promote OS and apoptosis of CD4+ T-cells.
The free radical, H2O2 plays a central role in activating NF-kB. However, HIV co-infection with mycoplasma has been noted to result in the release of H2O2 from T-cells.7,8 Without a sufficient supply of antioxidants, the activity of NF-kB may become excessive and further promotes HIV replication. At a medium level of OS cells have been shown to undergo a halt on cell growth and differentiation. 9 At this level the redox-sensitive transcription factor NF-kB and activator protein-1, are activated to induce stress protein synthesis through antioxidant responsive dements on stress protein genes. Factors involved in apoptotic pathways are also activated and the cell may undergo the characteristics changes associated with apoptosis. 10 A high OS level is characterized by the pathological changes of free radical damage, thus the cell undergoes death marked by necrosis. 11
However, response to ROS (reactive oxygen species) at cellular level occurs through antioxidant responsive elements and oxidative stress response genes. Antioxidants are groups of substances which, when present at low concentrations, in relation to oxidizable substrates, significantly inhibit or delay the oxidative processes while often being oxidized themselves. 12
The glutathione system (reduced glutathione [GSH], glutathione peroxidase [GHPX], glutathione reductase [GSH] and glutathione S-transferase [GST]) is a key defense against H2O2 and other peroxides. 13 GSH apart from being an antioxidant may have antiviral properties 14 depending on its concentration. GHPX (EC 1.11.1.19) catalyzes the reduction of a variety of hydroperoxides (ROOH and H2O2) using GSH, thus protects mammalian cells against oxidative damage. However, GST provides a different agent of free radical attack. They catalyze the addition of tripeptide glutathione to endogenous and xenobiotic substances thus increasing their solubility.
Superoxide dismutase (SOD) (EC.1.15.1.) destroys the free radical superoxide by converting it to peroxide that can in turn be destroyed by catalase or GHPX. Cells acutely infected with HIV have been reported to express less SOD and to lose their ability to induce antioxidant enzymes in response to TNF. 15
Catalase (EC 1.11.1.6) is so efficient an antioxidant that it cannot be saturated by H2O2 at any concentration. 16 It protects the cells from H2O2 generated within them.
Available evidence on serodiscordant-HIV infection in sexual partners excludes antioxidants as a possible agent for non-susceptibility in the seronegative partners. However, several explanations already reported on serodiscordant-HIV infection does not holistically explain this phenomenon especially its occurrence in the black African population.
The study therefore, tends to indicate the role of endogenous antioxidants in HIV-resistant individuals of Nigerian origin.
Methods
Study population
The case-control study had 39 samples comprising 13 serodis-cordant partners (26) and 13 healthy normal individuals of average age 36 ± 6. They were assigned into three groups; A (serodiscordant-seronegative), B (serodiscordant-seropositive) and C (healthy seronegative individuals). Groups B and C served as positive and negative controls, respectively.
Sample collection and identification
HIV-serodiscordant partners recruited for this study were from the following centres; Braithwait Memorial Hospital (BMH), Port Harcourt, River State, voluntary confidential counselling and testing centre Uyo, Akwa Ibom State and Winners medical research and diagnostic laboratory Abuja. The partners were recruited from those undergoing HIV screening for the first time, either as a pre-requisite for marriage consummation or for medical diagnosis. Also from individuals who on routine HIV-status check-up (in which case they were requested to bring along their sexual partners for HIV screening). In all the partners, sexual activity was confirmed through oral discussion and counselling. Venepuncture heparin anticoagulated peripheral blood samples from a total of 39 individuals were obtained after informed consent according to the Nigerian National Ethics and Operational Guidelines for Research on Human subjects (NNECGRHS). All of the partners had had an unprotected sexual relationship for at least six months and presented no other risk factor than sexual exposure to the HIV-infected partner. Also they had not been on any antiretroviral therapy.
HIV screening and confirmation
The samples (plasma) collected were screened at various centres mentioned earlier to detect antibodies for HIV-1 and 2 using the determine test kit (Abbot determine HIV-1/2 kit, Abbot, Japan) and confirmation by enzyme immunoassay method (ImmunoComb 11, version 434/Eb, Organic, Israel).
Classification and staging of HIV disease
Group B (serodiscordant-seropositive) was categorized according to the 1993 Centers for Disease Control and Prevention, 17 and clinical staging by World Health Organization HIV-staging system. 18
Determination of CD4, CD8 and CD3 T-lymphocytes
CD4, CD8 and CD3 lymphocytes were determined using a FACScan (fluorescent activated cell sorting) flow cytometer (Becton Dickson Immunocytometry systems, San Jose, CA, USA). A three-tube two-colour panel assay was used. The tubes contain the reagents, flourescein, isothiocynate (FITC), FITC-mouse immunoglobulin, PE-mouse immunoglobulin and phycoerythrin for CD3, CD4, CD8 and CD45. Fifty micro-litre of whole blood and 20 μL of monoclonal antibodies were added to a tru-count tube. It was incubated for 20 minutes for 450 μL of lysing reagent (FACS lysing solution) was added. All tubes were analysed using a FACScan flow cytometer. The two-colour data were analysed using Cell Quest software and attractors for the three-colour data.
Biochemical assay
Blood samples collected from the partners were centrifuged at 10,000 g for five minutes and the plasma collected was used for the assay. Plasma activity of catalase was assayed using the method of Cohen. 19 The purple colour of potassium permanganate is bleached by H2O2 when excess permanganate is added to the reaction mixture. The absorbance was read at 480 nm and the result expressed as a function of first-order reaction rate constant (K). SOD activity was based on the method of McCord and Fridovich. 20 GSH was assayed by the method of Boveris and Chance. 21 Assay of GHPX activity was based on the method formulated by Wendel 22 where the rate of β-NADPH consumption was monitored as a measurement for the rate of GSSG - formation during GSHPX reaction. The rate of decrease in absorption of β-NADPH at 340 nm was monitored and the result were expressed in units/millilitre of enzyme. GST activity was assayed in form of its ability to conjugate glutathione with 1-chloro -2, 4 dinitrobenzene as described by Habig. 23
Statistical analysis
Data were analysed with a computer using SPSS version 10.0 (SPSS, Chicago, IL, USA) software package. Differences between means were assessed using analysis of variance (ANOVA). The acceptable level of significance was P < 0.05. Correlations were evaluated by Spearmen's correlation.
Results
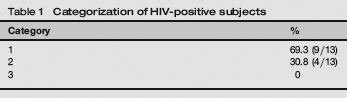
The category (Table 1) and clinical disease stages (Table 2) of the index, partner in group B (serodiscordant-seropositive) subjects’ show that 69.3% of the positive partner were at category 1, 30.8% at category 2. None was under category 3. However, 61.5% were at clinical stage 1 where 38.5% were at stage 2. None of the partners were at stages 2 and 4.
Categorization of HIV-positive subjects
Clinical staging of HIV-positive subjects

Table 3 shows the level of expression of CD4, CD8 and CD3 T-lymphocytes. In group A (serodiscordant-seronegative), the mean CD4+ T-cell count showed a significantly (P <0.05) increased levels of expression by 237% change when compared with group B (serodiscordant-seropositive partner). Comparison of groups A and C did not show any significant statistical decrease (3.1% decrease). The CD3+ T-lymphocyte count in group A significantly increased by 243.9% when compared with that of group B (P <0.05) but insignificantly increased (22.9%) when compared with the counts in group C. Similarly, CD8+ T-cells were significantly (P < 0.05) increased by 142.5% on comparison with groups B and C (seronegative healthy control subjects) by 69%.
Expression of CD4 CD8, and CD3 Positive T-lymphocytes
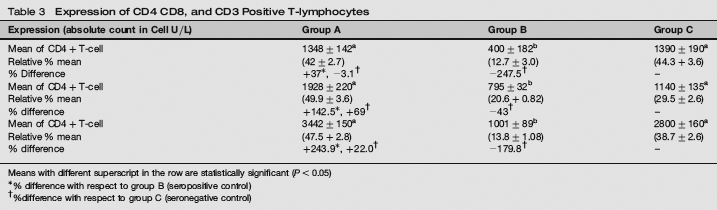
Means with different superscript in the row are statistically significant (P< 0.05)
%difference with respect to group B (seropositive control)
%difference with respect to group C (seronegative control)
In Table 4, the plasma level of the antioxidant enzymes; catalase, SOD, GHPX and GST indicates a significant (P < 0.05) increase in activity by 119.0%, 164.7%, 126% and 355.2%, respectively in group A when compared with group B. Comparison of groups A and C similarly revealed a significant (P < 0.05) increase in the activity of catalase (17.5%), SOD (50%) and GST (150.3%). GHPX insignificantly (P > 0.05) increased by 9.6% in A over B. However, group B revealed a significant (P < 0.05) decrease in activity by 86.5% (catalase), 76.5% (SOD), 106.8% (GHPX) and 81.8% (GST) on comparison with group C.
Plasma activity of antioxidant enzymes in the serodiscordant-seropositive (A) serodiscordant-seronegative (B) and seronegative normal individual (C)

SOD = superoxide dismutase; GST = glutathione S-transferase; GHPX = glutathione peroxidase
Means with different superscript in the row are statistically significant (P < 0.05)
% difference with respect to group B (seropositive control)
% difference with respect to group C (seronegative control)
Groups A and C showed a positive correlation (P < 0.01, r = 0.90) with their respective CD4 + T-cells and the antioxidant enzymes, CAT, SOD, GHPX and GST. Similarly, the antioxidant enzymes and CD4+ T-cell in group B showed a positive correlation (P < 0.01, r = 0.76).
Discussion
Many works have been reported on antioxidants in HIV-infected persons, but this study was done on serodiscordant-heterosexual partners. To our knowledge, this investigation is the first to show such high level of activity of endogenous antioxidants in HIV-seronegative-serodiscordant heterosexual partners in a Nigerian population.
Sixty-nine percent of the seropositive-serodiscordant subjects that were at category 1 (CD4 = >500 cell/UL) and the 30.1% on category 2 (CD4 = >200-499 cells/UL), indicate that 69% of the individuals were at acute (primary) HIV infection stage and that both HIV stages of these seropositive subjects are capable of transmitting HIV to their sexual partners. These stages of HIV infection has a very high transmission rate, thus indicating that their seronegative partners actually were exposed to adequate HIV environment, which have the threshold to infect cells. In several studies, it was noted independently that when the index partner is in the acute/ primary phase of infection, the recipient partner remains at a much higher risk of acquiring HIV infection.24,25
The low CD4+ T-cell (helper/inducer cell) count in group B is indicative of an immunocompromised status. This could be due to the inability of the antioxidants to protect the CD4 T-cells from HIV attachment and/or attack, since cross-linking of HIV glycoprotein and CD4 T-cells produces oxidants and/ or apoptotic death of the CD4 T-cells. The observed increase (277%) of CD4 T-cells in the seronegative partners (group A) suggests that the immune strength of this group is untempered and intact. Other investigators have reported that the probability of HIV-1 transmission per sexual contact is higher among people who are immunocompromised.26,27 Our result concurs with the report of their studies.
The high increase (142.5%) of CD8 + T-cell in the serodiscordant-seronegative partners suggests that the expression of high CD8+ T-cells could, in part, be responsible for preventing and/ or controlling HIV infection since CD8 T-cells (suppressor cells) can liberate soluble factors with antiviral activity (MlP-lα, MIP-l-β [macrophage inflammatory protein] RANTES [regulated on activation, normal T expressed and secreted]) to mediate the destruction of HIV. 28 Previous studies have suggested that these chemokines bind to CCR5 co-receptor and decrease or inhibit the ability of HIV to gain entry into susceptible cells. 29 The low expression of CD8 T-cell may suggest an impaired function of the CD8 + T-cell to proliferate in response to T-cell receptor. From the results of the study, low CD4 + T-cell is linked to low endogenous antioxidant status.
Lledias and Hansberg 16 noted that catalase is so efficient an antioxidant that it cannot be saturated with H2O2 at any concentration. It is known that H2O2 plays a central role in activating NF-kB (NF-kB activates HIV replication). The decrease in catalase activity (119.1%) in the seropositive subjects indicates an impaired function of catalase to decompose the H2O2 being generated in the course of HIV infection. Conversely, the high catalase activity in the seronegative partners indicate an effective antioxidant protection of the cell from H2O2-induced replication of HIV virus. 30
The SOD activity was found to show a 164.7% decrease in activity in the seropositive subjects with respect to their seronegative partners. Flores 15 noted that cells which produce HIV regulatory protein (Tat) have decreased expression of SOD RNA levels and show evidence of oxidative stress. However, Tat is a transcriptional transactivator protein essential for HIV-1 replication. 31 The decreased level of SOD in the seronegative partner may have resulted from the action of HIV-Tat in down-regulating the activity of SOD and maintaining an oxidatively stress status, which poise the cell for active HIV proliferation or transcription. These oxidative conditions may alter the cellular phenotype thus favouring viral replication and survival. Furthermore, the low level of SOD may possibly reflect the perturbed metabolism of a dying virus-infected cell. Since the activity of Tat is linked to cellular redox state, the result of high SOD activity obtained in the seronegative partners suggests that SOD was able to interfere with the function of HIV Tat protein leading to suppressed HIV replication. The high SOD-Tat activity may have resulted in increased chemokines (MlP-lα, MIP-β and RANTES)32,33 These chemokines are ligands for the CCR5 co-receptor, which the virus uses for entry. Their introduction at high levels blocks the HIV entrance32,33
The results of the study on the glutathione system shows that GHPX and GST activities were significantly increased in the seronegative subjects by 126% and 150%, respectively, over those of the their seropositive partners. The down-regulation of SOD by Tat is accompanied by a decreased glutathione content (decreased GSH: GSSG ratio). 34 Such an imbalance in the antioxidant defense system enhances the susceptibility of cells towards the cytotoxic action of TNF. 35 In line with these reports, the result of this investigation on the glutathione system suggests that in the seropositive subjects possibly HIV-Tat protein may have inhibited SOD, a synthesis which consequently led to increased superoxide anion concentration. The decrease of GST in the seropositive subjects may indicate a low production of GST (GST dysfunction). This, however, shows the inability of the enzyme to conjugate GSH with other exogenous electrophils such as those produced during infection. Conversely, in the seronegative partner, the high glutathione level may have reduced the infectivity of the virus as noted by Pagamara, 14 possibly through the suppression of the non-immunosuppressive HIV proteins; gp 120, p24, gag and viral infectivity factor. This suppressed expression of the gp 120 (major envelopes glycoprotein rich in intrachain disulphide bonds) interferes with the late stage of virus replication and is sensitive to the effect of a reducing agent such as GSH. This was supported by the already established fact that glutathione inhibits the reverse transcriptase process and its expression and blocks in a concentration-dependent manner, the activation of essential protein-splitting enzymes, such as HIV proteases. 36
The positive correlation of CD4 + T-cells and antioxidants indicate a linear relationship which suggests that increase in antioxidant levels may be responsible for the increased CD4 T-cells found in the seronegative partner, whereas decreased antioxidants led to lower CD4 T-cell expression. Gougeon and Montagnier 6 reported that T-cells are primed to undergo apoptosis upon cross-linking of CD4 + cell by gp 120. The cross-link creats an electron-deficient free radical in the CD4 cells, which requires the action of an antioxidant, this may explain the low CD4 cells found in the seropositive partner.
This study thus suggests that endogenous antioxidants (catalase, SOD, GST and GHPX) may be linked to the seronegative status of exposed HIV heterosexual partners.