
Abstract
The aim of this work was to study the human papillomavirus (HPV) type-distribution in condylomata acuminata (CA) of mainland China and to estimate the potential role of HPV prophylactic vaccines for CA in mainland China. Forty-three studies using polymerase chain reaction to detect HPV were included in this meta-analysis, and totally 5247 CA cases and 436 controls were included. The overall and type-specific prevalence of HPV 6, 11, 40, 42, 43, 44 were estimated using non-conditional logistic regression model. Overall HPV prevalence was 84.2% and 4.6% for CA and controls, respectively. Estimated HPV types 6, 11, 40, 42 positive fractions in CA were 54.9%, 41.1%, 2.7% and 2.0%, respectively, and exactly 0% for HPV types 43 and 44. HPV 6 and/or 11-positive fractions were 83.0% in mainland China. Thus, prophylactic HPV vaccine has the potential to protect up to 83% of CA cases in mainland China.
Introduction
An infectious aetiology of human genital cancer has been widely discussed.1,2 Condylomata acuminata (CA), commonly known as genital warts, is the most common benign tumour in the anogenital region. 3 They are proliferative lesions of genital epithelium, and human papillomavirus (HPV) is the main aetiological agent of CA. 4 The majority of CA contains HPV 6 or HPV 11 genomes. HPV 6 has been detected approximately three times more often than HPV 11 in these lesions. 5 Together, HPV types 6 and 11 have been detected in up to 95% of CA cases. 6
A wide variety of treatments for CA are in use, but therapeutic failures and recurrence after initial clearance are seen with all the treatments. 7 Psychological stress is often greater than the morbidity of the disease in CA patients. Consequently, HPV infection is a major public health burden, and successful prevention of CA is crucial. Nowadays, HPV prophylactic vaccines have been successfully developed and may be available in China in the near future, which may improve the prospects for the future prevention of CA. For cervical cancer and its precursor lesions, we have had lots of information on HPV type-distribution.8–11 Nevertheless, there is limited knowledge on HPV type-distribution of CA in China. The purpose of this meta-analysis is to understand the overall and type-specific HPV prevalence of CA and to estimate the effect of prophylactic vaccines on CA in mainland China.
Materials and Methods
Study selection criteria
Published material was extracted from the citations listed in Medline and China National Knowledge Infrastructure. Key search terms included: CA, genital warts, HPV, China and polymerase chain reaction (PCR). In this meta-analysis, we searched for the articles that were published either in the Medline database or in the CNKI from January 1990 to December 2006. All the included studies were limited to the following inclusion criteria: (1) study subjects were from mainland China, (2) CA cases and controls were diagnosed by histology, clinic or cytology; (3) at least 20 specimens of CA cases and/or controls were tested: (4) a clear description of the use of PCR-based assay to identify HPV DNA; (5) at least HPV 6 and 11 were reported in the HPV DNA typing results; (6) publication with the largest sample size was selected if the data or data subsets were published in more than one article.
Data abstraction
The following key variables were extracted from each study: (1) overall and genotype-specific prevalence of HPV infection; (2) geographic regions; (3) types of CA specimens for HPV DNA testing (fresh/fixed biopsies or exfoliated cells); (4) PCR primers used to detect HPV; (5) type of diagnosis for CA and control (histology, clinic or cytology). Geographic areas of mainland China were divided into north and south of the Yangtze River. Detailed information on all the included studies is presented in Appendix A.
Estimation of the overall and type-specific prevalence
HPV prevalence data were expressed as the percentages of HPV DNA positive CA among all the HPV DNA tested for CA. Multiple infections were separated into constituent types. Thus, the type-specific-HPV prevalence included either single or multiple infections. Type-specific prevalence was recorded for six common CA-associated HPV types (6, 11, 40, 42, 43 and 44) reported in the included articles. Type-specific HPV prevalence was calculated only for the studies that tested specific HPV types, and therefore the sample size varied between the type-specific analyses.
Statistical analyses
Sources of variation in the overall HPV prevalence were investigated by unconditional multiple logistic regression analysis and adjusted using four potential confounding factors (geographical region, type of specimen for HPV DNA testing, PCR primer and diagnostic method of specimens). All the statistically significant variables were included in the final logistic model. Adjusted HPV prevalence and 95% confidence intervals were calculated by adjusting the statistically significant variables. P values for comparing the stratified HPV prevalence were calculated using Chi-square tests.
Results
Studies included
A total of 5247 CA cases from the 43 identified studies were included in this meta-analysis. CA cases were stratified into the following different subgroups: (1) geographical region (1092 north, 4155 south); (2) type of specimen (4764 fresh/fixed biopsies, 483 exfoliated cells); (3) PCR primer (4659 type-specific (TS)-primer, 588 Universal-primer); (4) diagnostic method (1556 histology, 3691 clinic). Ten studies presented HPV prevalence data of the control group and totally 436 controls (312 healthy people, 107 pseudo-condyloma, six common warts and 11 other warts) were included.
meta-analysis of the overall HPV prevalence
A total of 4405 (84.0%) CA specimens were tested positive for HPV DNA. All the four potential confounding factors (geographical region, type of specimen for HPV DNA testing, PCR primer and diagnostic method of specimens) were introduced into the final unconditional multiple logistic regression model. According to this model, the overall adjusted HPV prevalence was 84.2% (84.1–84.3%). In the control group, the overall adjusted HPV prevalence was 4.6% (4.3–4.8%).
The overall adjusted HPV prevalence of CA varied geographically from 89.7% in the north to 82.8% in the south (P < 0.01). In the control group, HPV prevalence ranged from 7.5% in the north to 1.4% in the south (P < 0.01). HPV DNA was significantly less likely to be detected in the specimens diagnosed by clinic (82.3%) than the specimens diagnosed by histology (88.8%) (P < 0.01). For PCR primers, no difference was found between the type-specific PCR primers and universal primers to amplify HPV DNA (P = 0.187). Adjusted HPV prevalence between different types of specimens did not differ significantly (P = 0.325) (Table 1).
Odds ratios (ORs) and 95% confidence intervals (CIs) for overall human papillomavirus (HPV) prevalence in condylomata acuminata (CA) cases according to different stratified variables

Stratified HPV prevalence was statistically significant, P < 0.01
PCR = polymerase chain reaction
meta-analysis of the HPV type-specific prevalence
In CA cases, the most common HPV types identified were, in the order of descending HPV prevalence, HPV 6, 11, 40 and 42. There were no specimens positive for HPV types 43 and 44 for all the included articles (Table 2).
Type-specific human papillomavirus (HPV) prevalence of condylomata acuminata (CA) and controls
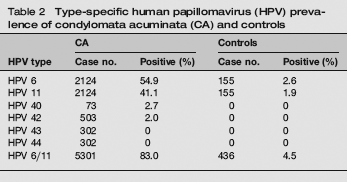
HPV type-specific prevalence of CA was shown in Table 2. HPV 6 and 11 were the predominant HPV types in CA, 54.9% and 41.1%, respectively. HPV 6 and/or 11 positive fraction was 83%. All the other four kinds of HPV types detected in this meta-analysis accounted for <5% of CA. Type-specific HPV prevalence varied between geographic regions. HPV 6 was the most common genotype in both of the regions ranging from 60.0% in the north to 53.4% in the south, and HPV 11 varied from 51.7% in the north to 38.2% in the south. HPV 40 (2.7%) and 42 (2.0%) were detected only in the south (Table 2).
The potential effect of prophylactic HPV vaccine for the prevention of CA could be estimated by HPV 6 and/or 11 positive fraction. In this meta-analysis, HPV 6 and/or 11 positive fraction varied between geographic regions. It was higher in north China (89.0%) than in south China (82.3%) (Figure 1).

Human papilomavirus-type-specific prevalence stratified by geographic regions
Discussion
CA are frequently observed lesions in sexually active individuals. Previous studies, as well as the present study, have demonstrated the presence of HPV type 6 or 11 DNA in the majority of CA. More than four-fifths of CA cases included in this meta-analysis were diagnosed positive for HPV 6 and/or 11 DNA. Other HPV types detected in this meta-analysis (40, 42, 43, 44) collectively accounted for 4.7% of CA.
Overall HPV prevalence
In this meta-analysis, the overall HPV prevalence was 84.2%, which might be underestimated. The reasons may be that some of the included studies may use less-sensitive PCR, and some CA-related low-risk HPV types were not reported in this meta-analysis, such as HPV types 53, 54 12 and 70. 13
HPV prevalence in the south of China was lower than that in the north. This geographic difference may be related to the complex interplay between different HPV genotypes, variants with host immunogenetic factors and/or lifestyles of the subjects. The demonstration of regional variation in the proportion of positivity for HPV 6 and/or 11 suggests that the effect of HPV prophylactic vaccines on CA will, at least to some degree, vary between regions.
Type-specific HPV prevalence
As many of the included studies tested for only a subset of HPV genotypes, this analysis was unable to estimate how often each HPV infection was found alone. Prevalence reported for each individual HPV genotype included those found in multiple infections.
Up to 60% of the included prevalent CA specimens were HPV 6 and/or 11 type-specific. Thus, we presented HPV type-specific prevalence with HPV 6 and/or 11 separately and combined. Because very few studies provided information about HPV 40, 42, 43 and 44 and the number of cases was relatively small, HPV 40, 42, 43 and 44 positive fractions here are only for reference. In this meta-analysis, there were no positive CA specimens containing HPV types 43 or 44 DNA, consistent with the findings reported by Lörincz et al. 14 Brown et al. 12 reported that after HPV types 6 and 11, HPV types 53 and 54 were the most frequently detected low-risk HPV types of CA, but we are unable to draw any conclusions about these two subtypes as none of the articles included in our meta-analysis reported results for them.
Study strengths and limitations
This meta-analysis included a large number of articles from China. Thus, it can give us a reasonably comprehensive overview of the overall and type-specific HPV prevalence of CA in China. Each HPV test used well-validated PCR primers known to amplify a broad spectrum of HPV genotypes. However, even these well-validated primers cannot amplify all the genotypes with exactly the same sensitivity 15 and such differences remain a potential source of variation in the detection of genotypes between studies.
The included studies have substantial variation in the overall HPV prevalence, which reflects the study-specific variations in the reliability and validity of histological or clinical diagnosis. All the included CA specimens were diagnosed in different hospitals, and the diagnostic standards for CA may be different.
HPV infection has a very high prevalence rate in adolescent girls and young women. Burk et al. 16 found that 36% of women 25 years of age or younger are HPV-positive compared with less than 3% of women 45 years of age and older. Most of the studies included in our meta-analysis did not publish results by sex and age, and we were unable to adjust for variations of sex and age in overall HPV prevalence.
In summary, this meta-analysis showed that the overall HPV prevalence of CA was 84.2%. Of all the CA cases included, HPV 6 and/or 11 accounted for 83%, and HPV types 40, 42, 43 and 44 for 4.7%. Our findings suggest that prophylactic HPV vaccines may potentially prevent up to 83% of CA in mainland China.
Footnotes
APPENDIX Table format of summary data
Condylomata acuminate
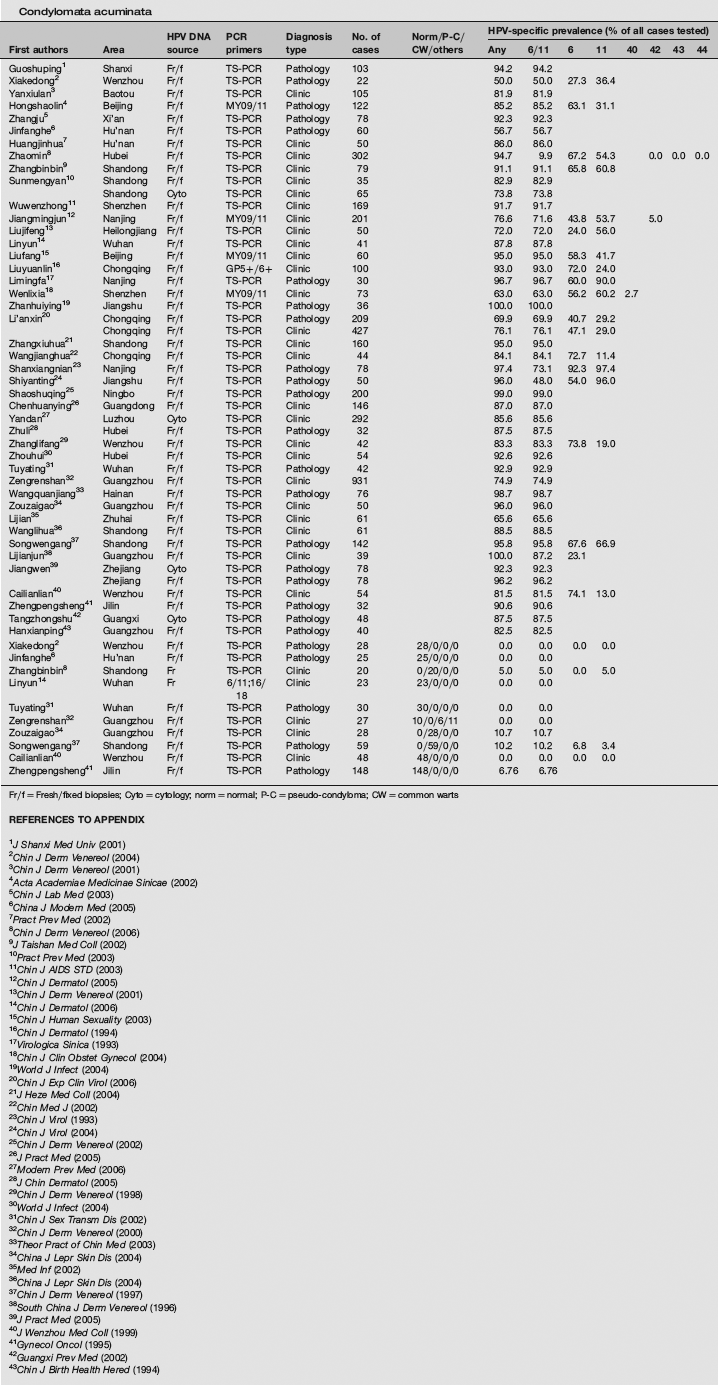
| First authors | Area | HPV DNA source | PCR primers | Diagnosis type | No. of cases | Norm/P-C/CW/others | HPV-specific prevalence (% of all cases tested) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Any | 6/11 | 6 | 11 | 40 | 42 | 43 | 44 | |||||||||
| Guoshuping 1 | Shanxi | Fr/f | TS-PCR | Pathology | 103 | 94.2 | 94.2 | |||||||||
| Xiakedong 2 | Wenzhou | Fr/f | TS-PCR | Pathology | 22 | 50.0 | 50.0 | 27.3 | 36.4 | |||||||
| Yanxiulan 3 | Baotou | Fr/f | TS-PCR | Clinic | 105 | 81.9 | 81.9 | |||||||||
| Hongshaolin 4 | Beijing | Fr/f | MY09/11 | Pathology | 122 | 85.2 | 85.2 | 63.1 | 31.1 | |||||||
| Zhangju 5 | Xi'an | Fr/f | TS-PCR | Pathology | 78 | 92.3 | 92.3 | |||||||||
| Jinfanghe 6 | Hu'nan | Fr/f | TS-PCR | Pathology | 60 | 56.7 | 56.7 | |||||||||
| Huangjinhua 7 | Hu'nan | Fr/f | TS-PCR | Clinic | 50 | 86.0 | 86.0 | |||||||||
| Zhaomin 8 | Hubei | Fr/f | TS-PCR | Clinic | 302 | 94.7 | 9.9 | 67.2 | 54.3 | 0.0 | 0.0 | 0.0 | ||||
| Zhangbinbin 9 | Shandong | Fr/f | TS-PCR | Clinic | 79 | 91.1 | 91.1 | 65.8 | 60.8 | |||||||
| Sunmengyan 10 | Shandong | Fr/f | TS-PCR | Clinic | 35 | 82.9 | 82.9 | |||||||||
| Shandong | Cyto | TS-PCR | Clinic | 65 | 73.8 | 73.8 | ||||||||||
| Wuwenzhong 11 | Shenzhen | Fr/f | TS-PCR | Clinic | 169 | 91.7 | 91.7 | |||||||||
| Jiangmingjun 12 | Nanjing | Fr/f | MY09/11 | Clinic | 201 | 76.6 | 71.6 | 43.8 | 53.7 | 5.0 | ||||||
| Liujifeng 13 | Heilongjiang | Fr/f | TS-PCR | Clinic | 50 | 72.0 | 72.0 | 24.0 | 56.0 | |||||||
| Linyun 14 | Wuhan | Fr/f | TS-PCR | Clinic | 41 | 87.8 | 87.8 | |||||||||
| Liufang 15 | Beijing | Fr/f | MY09/11 | Clinic | 60 | 95.0 | 95.0 | 58.3 | 41.7 | |||||||
| Liuyuanlin 16 | Chongqing | Fr/f | GP5 + /6+ | Clinic | 100 | 93.0 | 93.0 | 72.0 | 24.0 | |||||||
| Limingfa 17 | Nanjing | Fr/f | TS-PCR | Pathology | 30 | 96.7 | 96.7 | 60.0 | 90.0 | |||||||
| Wenlixia 18 | Shenzhen | Fr/f | MY09/11 | Clinic | 73 | 63.0 | 63.0 | 56.2 | 60.2 | 2.7 | ||||||
| Zhanhuiying 19 | Jiangshu | Fr/f | TS-PCR | Pathology | 36 | 100.0 | 100.0 | |||||||||
| Li'anxin 20 | Chongqing | Fr/f | TS-PCR | Pathology | 209 | 69.9 | 69.9 | 40.7 | 29.2 | |||||||
| Chongqing | Fr/f | TS-PCR | Clinic | 427 | 76.1 | 76.1 | 47.1 | 29.0 | ||||||||
| Zhangxiuhua 21 | Shandong | Fr/f | TS-PCR | Clinic | 160 | 95.0 | 95.0 | |||||||||
| Wangjianghua 22 | Chongqing | Fr/f | TS-PCR | Clinic | 44 | 84.1 | 84.1 | 72.7 | 11.4 | |||||||
| Shanxiangnian 23 | Nanjing | Fr/f | TS-PCR | Pathology | 78 | 97.4 | 73.1 | 92.3 | 97.4 | |||||||
| Shiyanting 24 | Jiangshu | Fr/f | TS-PCR | Pathology | 50 | 96.0 | 48.0 | 54.0 | 96.0 | |||||||
| Shaoshuqing 25 | Ningbo | Fr/f | TS-PCR | Pathology | 200 | 99.0 | 99.0 | |||||||||
| Chenhuanying 26 | Guangdong | Fr/f | TS-PCR | Clinic | 146 | 87.0 | 87.0 | |||||||||
| Yandan 27 | Luzhou | Cyto | TS-PCR | Clinic | 292 | 85.6 | 85.6 | |||||||||
| Zhuli 28 | Hubei | Fr/f | TS-PCR | Pathology | 32 | 87.5 | 87.5 | |||||||||
| Zhanglifang 29 | Wenzhou | Fr/f | TS-PCR | Clinic | 42 | 83.3 | 83.3 | 73.8 | 19.0 | |||||||
| Zhouhui 30 | Hubei | Fr/f | TS-PCR | Clinic | 54 | 92.6 | 92.6 | |||||||||
| Tuyating 31 | Wuhan | Fr/f | TS-PCR | Pathology | 42 | 92.9 | 92.9 | |||||||||
| Zengrenshan 32 | Guangzhou | Fr/f | TS-PCR | Clinic | 931 | 74.9 | 74.9 | |||||||||
| Wangquanjiang 33 | Hainan | Fr/f | TS-PCR | Pathology | 76 | 98.7 | 98.7 | |||||||||
| Zouzaigao 34 | Guangzhou | Fr/f | TS-PCR | Clinic | 50 | 96.0 | 96.0 | |||||||||
| Lijian 35 | Zhuhai | Fr/f | TS-PCR | Clinic | 61 | 65.6 | 65.6 | |||||||||
| Wanglihua 36 | Shandong | Fr/f | TS-PCR | Clinic | 61 | 88.5 | 88.5 | |||||||||
| Songwengang 37 | Shandong | Fr/f | TS-PCR | Pathology | 142 | 95.8 | 95.8 | 67.6 | 66.9 | |||||||
| Lijianjun 38 | Guangzhou | Fr/f | TS-PCR | Clinic | 39 | 100.0 | 87.2 | 23.1 | ||||||||
| Jiangwen 39 | Zhejiang | Cyto | TS-PCR | Pathology | 78 | 92.3 | 92.3 | |||||||||
| Zhejiang | Fr/f | TS-PCR | Pathology | 78 | 96.2 | 96.2 | ||||||||||
| Cailianlian 40 | Wenzhou | Fr/f | TS-PCR | Clinic | 54 | 81.5 | 81.5 | 74.1 | 13.0 | |||||||
| Zhengpengsheng 41 | Jilin | Fr/f | TS-PCR | Pathology | 32 | 90.6 | 90.6 | |||||||||
| Tangzhongshu 42 | Guangxi | Cyto | TS-PCR | Pathology | 48 | 87.5 | 87.5 | |||||||||
| Hanxianping 43 | Guangzhou | Fr/f | TS-PCR | Pathology | 40 | 82.5 | 82.5 | |||||||||
| Xiakedong 2 | Wenzhou | Fr/f | TS-PCR | Pathology | 28 | 28/0/0/0 | 0.0 | 0.0 | 0.0 | 0.0 | ||||||
| Jinfanghe 6 | Hu'nan | Fr/f | TS-PCR | Pathology | 25 | 25/0/0/0 | 0.0 | 0.0 | ||||||||
| Zhangbinbin 8 | Shandong | Fr | TS-PCR | Clinic | 20 | 0/20/0/0 | 5.0 | 5.0 | 0.0 | 5.0 | ||||||
| Linyun 14 | Wuhan | Fr | 6/11;16/ 18 | Clinic | 23 | 23/0/0/0 | 0.0 | 0.0 | ||||||||
| Tuyating 31 | Wuhan | Fr/f | TS-PCR | Pathology | 30 | 30/0/0/0 | 0.0 | 0.0 | ||||||||
| Zengrenshan 32 | Guangzhou | Fr/f | TS-PCR | Clinic | 27 | 10/0/6/11 | 0.0 | 0.0 | ||||||||
| Zouzaigao 34 | Guangzhou | Fr/f | TS-PCR | Clinic | 28 | 0/28/0/0 | 10.7 | 10.7 | ||||||||
| Songwengang 37 | Shandong | Fr/f | TS-PCR | Pathology | 59 | 0/59/0/0 | 10.2 | 10.2 | 6.8 | 3.4 | ||||||
| Cailianlian 40 | Wenzhou | Fr/f | TS-PCR | Clinic | 48 | 48/0/0/0 | 0.0 | 0.0 | 0.0 | 0.0 | ||||||
| Zhengpengsheng 41 | Jilin | Fr/f | TS-PCR | Pathology | 148 | 148/0/0/0 | 6.76 | 6.76 | ||||||||
Fr/f = Fresh/fixed biopsies; Cyto = cytology; norm = normal; P-C = pseudo-condyloma; CW = common warts
J Shanxi Med Univ (2001)
Chin J Derm Venereol (2004)
Chin J Derm Venereol (2001)
Acta Academiae Medicinae Sinicae (2002)
Chin J Lab Med (2003)
China J Modern Med (2005)
Pract Prev Med (2002)
Chin J Derm Venereol (2006)
J Taishan Med Coll (2002)
Pract Prev Med (2003)
Chin J AIDS STD (2003)
Chin J Dermatol (2005)
Chin J Derm Venereol (2001)
Chin J Dermatol (2006)
Chin J Human Sexuality (2003)
Chin J Dermatol (1994)
Virologica Sinica (1993)
Chin J Clin Obstet Gynecol (2004)
World J Infect (2004)
Chin J Exp Clin Virol (2006)
J Heze Med Coll (2004)
Chin Med J (2002)
Chin J Virol (1993)
Chin J Virol (2004)
Chin J Derm Venereol (2002)
J Pract Med (2005)
Modern Prev Med (2006)
J Chin Dermatol (2005)
Chin J Derm Venereol (1998)
World J Infect (2004)
Chin J Sex Transm Dis (2002)
Chin J Derm Venereol (2000)
Theor Pract of Chin Med (2003)
China J Lepr Skin Dis (2004)
Med Inf (2002)
China J Lepr Skin Dis (2004)
Chin J Derm Venereol (1997)
South China J Derm Venereol (1996)
J Pract Med (2005)
J Wenzhou Med Coll (1999)
Gynecol Oncol (1995)
Guangxi Prev Med (2002)
Chin J Birth Health Hered (1994)
Acknowledgements
We are grateful to all of the authors who made detailed data available for this meta-analysis and to my colleagues for their helpful comments. We acknowledge the support of Merck Company.