
Abstract
This case is about an HIV seropositive young woman referred for the treatment of severe menorrhagia causing anaemia due to adenomyosis where the levonorgestrel-releasing intrauterine system (Mirena®) proved useful in treating her heavy periods and also provided effective contraception without interference from the liver enzyme-inducing effects of antiretroviral medications.
Case Report
A 29-year-old HIV-positive woman was referred to the special clinic providing medical gynaecology and contraception for HIV-positive women for contraceptive advice and management of menorrhagia.
She had been suffering from painful heavy periods for the last two years lasting seven days in a regular 29–30 day cycle. There was a history of dyspareunia. She used condoms for contraception. She had been given oral iron therapy for the anaemia and tranexamic acid 1 g three times daily plus mefenamic acid 500 mg three times daily for dymenorrhoea and menorrhagia without relief. Microgynon 30 in a tricycling regime had then been tried, also unsuccessfully. In fact, her bleeding had become continuous with the COC (combined oral contraceptive) and hence she had stopped it. She had been diagnosed HIV-positive four years previously and was currently taking antiretroviral medication consisting of Combivir (zidovudine 300 mg and lamivudine 150 mg) one every 12 hours and nevirapine (200 mg every 12 hours).
In the special clinic on per abdominal and vaginal examination the uterus was found to be uniformly enlarged to a size of 14 weeks gestation, mobile, firm and non-tender. There was no adnexal mass, tenderness or cervical excitation. A high resolution transvaginal ultrasound scan, undertaken to identify any distortion of the uterine cavity and exclude endometrial or fibroid polyps, revealed an enlarged uterus with asymmetrically thickened, irregular, cystic myometrium suggestive of adenomyosis (Figure 1). There was no distortion of the uterine cavity. Endometrium and ovaries were normal. Haemoglobin was 8.4 g/dL and platelet count 26 × 109/L. It was concluded that the cause of her anaemia, menorrhagia and dysmenorrhoea was adenomyosis.
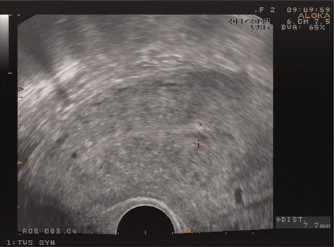
Ultrasound scan picture of adenomyosis
The treatment of her menorrhagia, any contraceptive measures and the antiretroviral treatment had to be compatible. The options for management were discussed with her including both surgical and medical treatments. Surgical options were dismissed as she wished to retain her fertility. As her antiretroviral medications included a liver enzyme-inducing drug (nevirapine), which reduces the efficacy of the combined oral contraceptive pill due to drug interaction, medical options for contraception were limited. The only contraceptive options were Depo-Provera or Mirena or barrier methods. Depo-Provera was ruled out as she was averse to injections. The only remaining option was the levonorgestrel-releasing intrauterine system (LNG-IUS licensed in the UK as Mirena® [Bayer Schering Pharma AG, Newsbury, Berks RG14 1JA, UK]). Given the properties of the latter as symptomatic treatment for menorrhagia as well as contraception, it seemed the ideal choice and one which she accepted and which was then inserted.
During follow-up, she reported less bleeding and pain. Her Hb had risen to 15 g/dL at four months follow-up. At later follow–up she remained happy with the Mirena®.
Discussion
Adenomyosis is relatively uncommon in such a young woman. It is most common in multiparous women in their late 40s and presents with menorrhagia, dysmenorrhoea, enlarged uterus and dyspareunia. It is a form of endometriosis in which endometrium appears as enclosures in the muscular layer of the uterine wall. In that age range it is a relatively common condition (16–39% based on unselected hysterectomy patients) and has to be considered in the evaluation of any women with abnormal bleeding. The aetiology and pathogenesis are poorly understood. There is some evidence that women who have had caesarean sections are more prone to adenomyosis. A number of factors may be implicated in its causation, such as immunological factors, oestrogen sulphatase activity, tenascrin as a fibronectin inhibitor, angiogenesis and growth factors, such as EG-VEGF (endocrine gland-derived vascular endothelial growth factor), and GM-CSF (granulocyte/macrophage colony stimulating factor). 1 However, American data suggest that in black Americans symptomatic essential adenomyosis occurs earlier and that dilatation and curettage may have an aetiological role. 2 Although merely speculative, it could be argued that the patient's previous pregnancy and its termination together with her caesarian section and ethnic origin may have constituted four contributory factors in the development of her condition.
In the past hysterectomy was the mainstay of treatment and diagnosis of adenomyosis and it clearly deals effectively with the condition especially the bleeding. Excision of localized adenomyosis, gonadotrophin-releasing hormone agonist treatment, endometrial ablation, uterine artery embolization have been tried with varying results.
However for younger patients, these alternatives might involve all or some loss of the capacity to conceive and hence none of the procedures would have been appropriate in the case of this patient who was anxious to preserve her fertility.
The LNG-IUS, based on the steady release of a low concentration of progesterone for contraceptive purposes, can also be used so as to allow a treatment providing symptomatic relief for menorrhagia (and dysmenorrhoea 3 although not licensed for this condition in the UK). It avoids the need for surgical intervention, preserves fertility and provides satisfaction with treatment and improvement in health-related quality-of-life from this treatment reportedly similar to those from hysterectomy. 4
This case was complex because treatment for the HIV, the anaemia and its cause and the contraceptive means had to be compatible. The patient's almost continuous bleeding with the use of COC could be attributed to the interaction between it and her antiretroviral medication (nevirapine). Some antiretroviral medications especially protease inhibitors and non-nucleoside reverse transcriptase inhibitors may reduce the efficacy of some contraceptive products due to their liver enzyme-inducing property. 5
For contraception, therefore, long-acting, reversible contraceptives which would not interact with liver enzyme-inducers had to be considered. Implants are expected to be less effective when used with the liver enzyme-inducing medications. Injectable contraceptives that might have been suitable were Depo-Provera or Noristerat. But she had ruled out all three as she was injection averse. The options left were IUCD (intrauterine contraceptive device) and IUS (intrauterine system). The possible side-effects of heavier periods and aggravated dysmenorrhoea with an IUCD precluded this as a choice for this patient.
That left the LNG-IUS, also useful for reducing bleeding and for those with painful periods and because of its primary endometrial action, thought to be effective even in the presence of liver enzyme-inducing products. 6 As a contraceptive, it is long-acting and fully reversible. The menstrual pattern and fertility return to normal soon after the removal of the LNG-IUS. The first months of use are often associated with irregular, scanty bleeding which usually resolves spontaneously.
Conclusion
In this case, the LNG-IUS was a very effective, quickly reversible, fertility-conserving treatment for menorrhagia and also an effective contraceptive so that the aims of contraception and management of heavy and painful bleeding were achieved with a single product.