
Abstract
An HIV-positive man with hepatitis B co-infection, naïve to highly active antiretroviral therapy, with a CD4 of 594 copies/mL and HIV-1 viral load of 140,070 copies, presented with right-sided facial weakness and hearing loss. He had been treated for secondary syphilis three months earlier when his rapid plasma reagin (RPR) result was 1:16, this had fallen to neat. At presentation, his RPR had risen to 1:16 again. A magnetic resonance imaging scan showed enhancement of the internal auditory canal and right cochlea. His cerebrospinal fluid examination was normal. He was treated with acyclovir and prednisolone before the syphilis serology was known. He was then treated for syphilis with doxycycline. He made an excellent recovery.
Keywords
Introduction
The prevalence of syphilis in the general population is increasing and is higher among the HIV-positive population. Otosyphilis in the general population is relatively rare and can occur in congenital, secondary or neurosyphilis. However, there are reports that substantiate the rapidly progressive and aggressive behaviour of neurosyphilis, including otosyphilis in the presence of HIV infection.1,2 We report one case of a patient with HIV, recent infection with syphilis and sudden hearing loss.
Case Report
A homosexual man in his 30s with stable HIV and hepatitis B co-infection, presented with a one week history of right-sided facial weakness, right-sided hearing loss as well as vertigo and tinnitus. His CD4 count was 594 mm and his HIV viral load was 140,070 copies/mL. He was antiretroviral naïve. Clinical examination revealed right-sided lower motor neurone facial nerve paresis and sensorineural deafness. He had no other abnormal clinical signs. A possible diagnosis of Ramsay Hunt syndrome was made and he was given a 10 day course of high-dose acyclovir and prednisolone.
A magnetic resonance imaging scan of his head two weeks later showed enhancement of the right internal auditory canal and cochlea (Figure 1a and b). The results of his cerebrospinal fluid (CSF) analysis are as follows: opening pressure 21 cm water, glucose 2.4, protein 0.4, red blood cells 199, white blood cells 7.0, no pus, no organisms. Rapid plasma reagin (RPR) negative. Polymerase chain reaction for herpes viruses was negative.
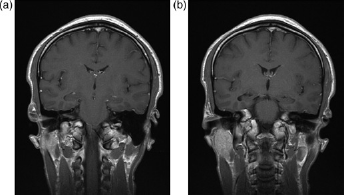
(a) Coronal T1 postgadolinium images show avid enhancement of both facial and vestibulocochlear nerves within the right internal auditory canal (arrow); (b) Enhancement is also seen with the right cochlea (arrowhead)
Three months before presentation he had been treated for secondary syphilis with one injection of 2.4 MU i.m. benzathine penicillin, when he presented with a maculopapular rash and lymphadenopathy. The results of his syphilis serology at that time were as follows: RPR 1:16, enzyme immunoassay positive, Treponema pallidum particle agglutination assay positive. One month later on repeat testing, his RPR became clear. In January 2007 (five months later), at the time of his presentation with hearing loss and facial nerve weakness, his RPR had risen to 1:16 (Table 1).
Syphilis serology from October 2005 to January 2007

At the time of review with the results of his syphilis serology, our patient already reported a 60% improvement in his facial nerve palsy and hearing.
He declined further treatment with benzathine penicillin; therefore, he was treated with doxycycline 100 mg t.i.d for four weeks.
Discussion
Since the Health Protection Agency started surveillance in 1997, 5452 cases have been seen up to the end of 2005. The incidence is highest in London (13.1 cases per 100,000 population). Diagnoses in men increased 20-fold and 45% of the cases in men who have sex with men, were also infected with HIV. Forty-five percent of infections are thought to have been the result of oral sex. 3
Otosyphilis is diagnosed by a combination of clinical findings, positive serum serology and exclusion of other causes of deafness. Symptoms include progressive and sudden unilateral or bilateral deafness, tinnitus, vertigo and disequilibrium. In a case review published in 1992, five out of 18 patients with otosyphilis had normal CSF analysis. 4 Therefore, CSF abnormality is not a prerequisite for diagnosis, although in the same paper, it was postulated that patients with an abnormal CSF should be given prolonged treatment and follow-up.
In the ear, syphilis causes bone osteotitis with involvement of the membranous labyrinth in later stages. Mononuclear cell infiltration and infiltrative endarteritis are found in other organs which are affected by syphilis and in the ear, this causes destruction of bone, with severe inflammation – gumma are formed. 5 Endolymphic hydrops also occurs.
In HIV-positive patients, Smith et al. 2 described how the depressed immune status of HIV-positive patients, may hasten the development of otosyphilis as it does in neurosyphilis by reactivation of dormant treponemes in the temporal bone. In HIV-positive patients, there may be a higher rate of neurological involvement in syphilis with unusual manifestations, a higher rate of treatment failure with benzathine penicillin, more frequent serological relapses and a lower rate of treponeme elimination. 1 It has also been suggested that a longer course of penicillin is important to prevent relapse in neurosyphilis. 5 Other studies have found that HIV-positive patients respond to standard syphilis treatment just as well as HIV-negative patients. 6
Our patient had previously been treated for secondary syphilis with standard treatment for early syphilis, but had possible reactivation 1 or become reinfected.
A literature search for treatments for otosyphilis revealed a range of different treatment modalities and duration. Steroids were used in some cases, and as a prolonged course in a subset. Treatment with penicillin was continued for up to 74 days in patients with a positive CSF (Patients who had had symptoms for the longest pretreatment had the worse prognosis 4 ).
Clinical response to treatment is quite variable. A case report of an HIV-positive man with otosyphilis who was treated with a long regimen of 33 days of antibiotics, resulted in an improvement in his hearing at six months, but mild imbalance remained. 7 Clinical response to treatment in Gleich's study was variablewith improved hearing in 31% of cases, although vertigo improved in 11%. 4 The largest case review of 85 patients with otosyphilis was published in Thailand in 2005. In this study treatment resulted in improvement of hearing in 93% of cases in the short term and 91% in the long term. 8 Otosyphilis is an important and potentially reversible cause of deafness.
Erratum – Correction to authors’ names
Christina Stefanaki, Ilias Katzouranis, Eirina Lagogianni, Maria Hagjivassiliou. Electra Nicolaidou, Antonios Panagiotopoulos, Vassilis Anyfantakis, George Bethimoutis, Rallis Eustathios, Christina Antoniou and Andreas Katsambas. Comparison of cryotherapy to imiquimod 5% in the treatment of anogenital warts. Int J STD AIDS 2008;
The name of one of the authors of this paper was inserted incorrectly, as Rallis Eustathios. Please note that the correct name should have been Eustathios Rallis.
We also point out that Maria Hadjivassiliou's name should be spelt as is given here.
Footnotes
Acknowledgements
We wish to thank Dr Cindy Sethi, GU Medicine Consultant (St Thomas's Hospital), Dr Mary O'Riordan, SHO GUM (King's College Hospital), Professor P Easterbrook, Professor of Epidemiology and Infectious Diseases (King's College Hospital), Mr Terry Nunn (Principal Audiologist) and Dr Michael Aboud (Spr) St Thomas's Hospital.