
Abstract
This unlinked anonymous study aimed at determining the prevalence of HIV among sexual health clinic attenders having blood samples taken for syphilis and/or hepatitis B serology in six major New Zealand cities over a 12-month period in 2005–2006. Overall, seroprevalence was five per 1000 (47/9439). Among men who have sex with men (MSM), the overall prevalence and that of previously undiagnosed HIV were 44.1 and 20.1 per 1000, respectively. In heterosexual men, the overall prevalence was 1.2 per 1000 and in women 1.4 per 1000. HIV remains to be concentrated among homosexual and bisexual men. Comparison with a previous survey in 1996–1997 suggests an increase in the prevalence of undiagnosed HIV among MSM and also an increase in the number of MSM attending sexual health clinics. The low prevalence of HIV among heterosexuals suggests no extensive spread into the groups identified at risk of other sexually transmitted infections.
INTRODUCTION
In New Zealand, as in many developed countries, the prevalence of HIV infection in the general population remains to be very low. Hence, to detect early changes in the pattern of spread it is helpful in studying sentinel populations such as people attending sexual health clinics who are likely to have been practising sexual behaviours that put them at increased risk of HIV infection. 1,2 This also enables monitoring of HIV in subgroups whose behaviour puts them at higher risk of sexual transmission. Surveillance of HIV based on named testing can give a misleading picture as people who agree to be tested generally have a lower prevalence than those who decline. 3–5 For this reason, the use of unlinked anonymous testing, in which blood collected for another purpose is anonymized and unlinked before testing, is recommended by the World Health Organization for public health surveillance of HIV infection. 6
The New Zealand AIDS Epidemiology Group (AEG) has carried out two unlinked anonymous prevalence surveys of HIV infection in sexual health clinics in 1991–19927 and 1996–1997 (unpublished). These studies confirmed that the most affected group was men who have sex with men (MSM), and that prevalence among heterosexual men and women was low (<0.1%). Since the second survey in 1996–1997, the survival of people with HIV had improved. In addition, from 2000 to 2006 there has been an increase in the annual number of people being diagnosed with HIV in New Zealand. 8 Together these changes would have resulted in an increase in the prevalence of diagnosed HIV. Since 2000, most of the increase in MSM diagnosed with HIV has been among those infected in New Zealand, while that among heterosexual men and women has been among people infected in countries where HIV prevalence is high. 9
A repeat unlinked anonymous study was undertaken during 2005–2006. The aims were to (a) determine the current prevalence of HIV among attenders at sexual health clinics in New Zealand who had blood taken for syphilis and/or hepatitis B serology; (b) compare this with the two previous similar studies; and (c) estimate the proportion of HIV infections not being diagnosed by voluntary named testing.
METHODS
The study population involved new clients presenting at New Zealand public sexual health clinics in Auckland, Hamilton, Tauranga, Palmerston North, Wellington and Christchurch over a 12-month period in 2005–2006, having blood taken for syphilis and/or hepatitis B serology. Clients who returned for a repeat visit in the same clinic within the study period were included only once. Those who attended solely for an HIV test were excluded as they would not be considered part of a usual sexually transmitted disease clinic population.
Comparison data of the baseline population, which included all sexual health clinic attenders, both new and follow-up visits, for any reason, were obtained from the Institute of Environmental Science and Research Limited (ESR) 2005 Annual Report. 10
Eligible participants had a data collection form attached to their notes (Figure 1). This had the same number, obscured by latex scratch-off material at the top and bottom, the lower one being detachable. When blood was taken, the detachable portion of the form was sent to the laboratory with the specimen and standard request form. The upper section of the clinical records, containing demographic, behavioural and diagnostic questions, was completed and sent to the study coordinator, with the number still obscured.
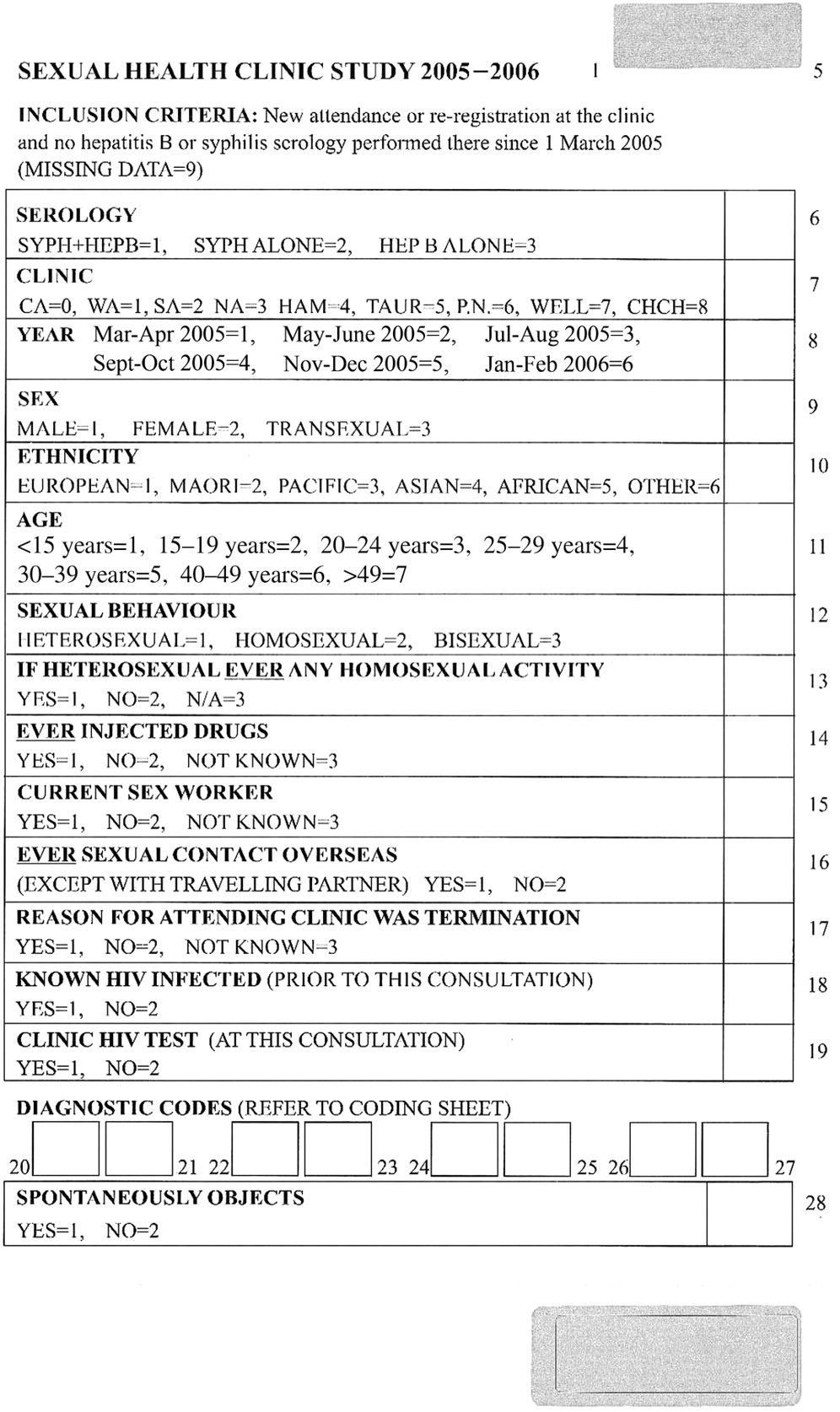
Data collection form
In the local laboratory, blood was centrifuged and if an adequate quantity was present 250–500 µL of serum were placed in a separate tube for HIV serology. The section of the data collection form stapled with the clinic request was attached to this sample, and was the only form of identification. These samples were then sent to the only laboratory that has undertaken HIV testing for this study.
Testing was performed on a pool made up of 10 specimens using Murex HIV AG/AB combination antibody screen. If the pool was negative, all the specimens were assumed to be negative. If the pool was positive, each individual specimen was tested and any individual positive sample was re-tested using the Western blot technique.
The worksheets were forwarded to the study coordinator who checked them to ensure that the study numbers had remained obscured. The scratch-off material covering the numbers was removed from both the data collection forms and laboratory work sheets and information entered onto a computer.
Ethical and legal issues
The usual amount of blood was taken for clinical syphilis or hepatitis B serology testing. Individual consent to use the residual blood after it had been anonymized was not sought. However, notices in several languages were posted in the waiting rooms of clinics. Anyone who spontaneously objected to their blood being included in the study had this recorded on the collection form and the blood was not tested. Voluntary named HIV testing was available at the clinic through a separate system.
The study was approved by the New Zealand Multiregion Ethics Committee.
Statistical analysis
Confidence intervals (CI) for proportions were calculated using exact methods, and proportions and trends were compared using χ 2 tests. 11
RESULTS
Sample
A data collection form and linked blood sample were obtained from 9439 people. In addition, 23 blood samples were not tested because of insufficient serum (11), tube leakage (six) or haemolysis (six); no data form were received for 108 samples; the sample could not be matched to any data form for 28 and a data collection form but no serum was received for 153 people. Two people objected to the study and were excluded. Thus, results were available for 9439 (96.8%) of the 9753 people. Sex, age group and sexual behaviour of these 9439 people are shown in Table 1.
Sex, age and sexual behaviour of study participants
Base population
A total of 63,223 clients were seen in sexual health clinics in the six centres in 2005. This number included all new and follow-up visits. Overall, 44.5% were males and 55.5% were females. Three-quarters of the females (72.7%) and half of the males (51.6%) were aged less than 30 years. The ethnicity of clients was European (67.6%), Maori (15.5%), Pacific (4.3%) and other/unknown (12.6%). The study sample was very similar to the base population on all demographic characteristics except for a small under-representation of women aged less than 20 years.
HIV prevalence
Overall, 47 of the 9439 people (5.0 per 1000; 95% CI 3.7–6.6) were found to be infected with HIV. Of these 47, 27 were already known to be infected. Among the men who had sex with men (MSM) – those whose current sexual behaviour was reported as either homosexual or bisexual – the overall prevalence and prevalence of previously undiagnosed HIV were 44.1 and 20.1 per 1000, respectively (Table 2). For the heterosexual men, the overall prevalence and that of previously undiagnosed HIV were 1.2 and 0.4 per 1000, respectively; and for the heterosexual women 1.4 and 0.6 per 1000. None of the 146 women who had sex with women were infected.
Overall HIV prevalence, and prevalence of previously undiagnosed HIV, by sex and sexual behaviour
CI = confidence interval
*MSM (men who have sex with men) are men whose behaviour was reported as either homosexual or bisexual
†WSW (women who have sex with women) are women whose behaviour was reported as either homosexual or bisexual
There was no HIV infection among the 298 females, 32 males and 13 trans-sexual current sex workers. The upper limit of 95% CI was 12.3 per 1000 for females, 115.3 per 1000 for males and 283.8 per 1000 for trans-sexual sex workers. The prevalence among those who reported ever injecting drugs but who did not report any current or past homosexual activity was 3.2 per 1000 (95% CI 0.1–17.6).
Among MSM, both the overall prevalence and prevalence of previously undiagnosed HIV were highest among those aged 30–49 years, and those attending Auckland clinics (Table 3). The numbers with a non-European ethnicity were too small to allow meaningful comparisons.
Overall HIV prevalence, and prevalence of previously undiagnosed HIV among men who have sex with men (MSM)
CI = confidence interval
Among those who reported only heterosexual activity, HIV prevalence was low (six men and five women) and was not limited to any specific ethnic or age group. Specifically, there were five Europeans, one Maori, one Pacific and two each of Asian and African ethnicity. Four were aged between 20 and 29 years, four between 30 and 39 years, and three between 40 and 49 years. Of these 11, 10 people with HIV reported having had sex overseas, compared with 34% of all heterosexual men and women. Nine of these 11, and all of the previously undiagnosed, were in Auckland.
Clinical HIV testing
Table 4 shows clinical HIV testing by sex, sexual behaviour, age group, region and ethnicity. Overall, three-quarters of those enrolled in the study had a clinical test for HIV. There were no consistent patterns of testing by age. Testing was lower in the Auckland clinics. Among the heterosexuals, HIV testing was highest among those of ‘other’ ethnicity and lowest among Pacific people.
Demographic characteristics of men and women who had a clinical test for HIV for whom a data collection form was received*
*Data exclude transsexuals, and those whose sexual behaviour and sex was not stated
Of all 20 previously undiagnosed HIV infected people, 16 were MSM; 12 (75.0%) of them had a clinical HIV test at that visit. This is slightly lower than the 84.2% test uptake among the uninfected MSM. Of the four previously undiagnosed heterosexuals, one of the two women, but neither of the two men had a clinical test.
Changes over time
With each subsequent unlinked anonymous study more centres were included. The numbers in the major sexual behaviour groups in each study are shown in Table 5. The numbers enrolled from the Auckland and Christchurch clinics dropped between the 1991–1992 and 1996–1997 studies, although the sexual behaviour in these two studies was similar. While the size of the samples in these clinics was similar in the 1996–1997 and 2005–2006 studies, the proportion of MSM increased markedly from 3.0% to 9.6%. This rise was predominantly made up of an increase in men with reported homosexual rather than bisexual behaviour. The number enrolled from the Wellington and Hamilton clinics increased by 50% from the 1996–1997 to 2005–2006 study, and the proportion of MSM here increased from 5.9% to 7.7%.
Numbers enrolled from participating sexual health clinics by study year*†
*Percentages do not add up to 100% as for some people this information was not available
†Excludes WSW
In Table 6, the prevalence of previously undiagnosed HIV in the three studies is shown. Tests for heterogeneity show no statistically significant differences by the year of study for any of the sexual behaviour groups, although the relatively small number of infected people means that there was relatively little statistical power to detect changes. What was striking in this analysis, however was the increase in the number of infected MSM, a reflection of the increase in MSM enrolled in 2005–2006.
Comparison of prevalence of previously undiagnosed HIV by sexual behaviour, centre involved and study year (per 1000)
A&C = Auckland and Christchurch; A,C,H&W = Auckland, Christchurch, Hamilton and Wellington; MSM = men having sex with men
*P value for test for heterogeneity
Over the three studies, there was a progressive statistically significant increase in the proportion having clinical HIV tests among all groups (Table 7). In both the 1996–1997 and the 2005–2006 studies, the proportion undergoing clinical HIV testing was higher in all the clinics combined than in Auckland and Christchurch.
Comparison of rates of clinical testing for HIV by sexual behaviour, centre involved and study year
A&C = Auckland and Christchurch; A,C,H&W = Auckland, Christchurch, Hamilton and Wellington; MSM = men having sex with men
*P value for test for trend
† P value for test for heterogeneity
DISCUSSION
This study shows that in New Zealand sexual health clinic attenders, HIV remains to be concentrated among homosexual and bisexual men. Among such MSM, the overall prevalence of HIV was 44.1 per 1000, and the prevalence of previously undiagnosed HIV was 20.1 per 1000. Hence, approximately one in 50 such men had previously undiagnosed HIV, with a higher proportion in Auckland than elsewhere. HIV infection was most common in men aged 30–49 years. The small number of infected non-European MSM precluded any useful comparison by ethnicity. Most (75.0%), but not all, of the previously undiagnosed MSM were tested for HIV at that attendance, although this was slightly more common among the uninfected.
There were only 11 heterosexual men and women with HIV; an overall prevalence of 1.3 per 1000, and the prevalence of previously undiagnosed HIV of 0.5 per 1000, with a similar prevalence of men and women. All major ethnic groups found in the New Zealand population – European, Maori, Pacific, Asian and African – were represented in this small number. There were only four previously undiagnosed heterosexual men and women, only one of whom had a clinical HIV test at that attendance, although the overall rate of HIV testing among heterosexual men and women was 71% and 75%, respectively.
The major strength of this study was that it allowed the measurement – in an ethically acceptable way – of the true HIV prevalence in this sentinel population and hence has provided valid insights into the characteristics of infected people, the problem of undiagnosed infection and possibly of trends over time.
It was not possible to be sure of what proportion of new attenders had blood drawn for syphilis and/or hepatitis B serology, as this information could only be provided by two centres. In these clinics, about half in one, and 20% in the other, of attenders had blood taken. The overall policy of the clinics was to offer blood tests to all new attenders, however our definition of new attender was restricted to the study period; hence, not all our new attenders would be expected to have blood taken. Moreover, clients referred from other providers were less likely to be tested. While this suggests that we might have underestimated the number of all attenders with undiagnosed HIV, the demographic features of the study sample were comparable with the overall sexual health clinic population except for a lower proportion of women aged less than 20. As well as this, the proportion of the study sample with gonorrhoea, chlamydia, genital herpes or genital warts was higher in the study than reported for all attenders (data not shown); hence, the study sample was at least at as high risk as sexual health clinic attenders as a whole. More importantly, the proportions of the study sample in 1991–1992, 1996–1997 and 2005–2006 with any STI diagnosis were similar in Auckland and Christchurch and increased in the other two centres.
To determine whether the results allow conclusions to be drawn about the patterns of HIV occurrence over time is complicated. The issues are (a) the comparability of the study samples; (b) the changes in survival from HIV such that the prevalence of known HIV would be expected to increase; and (c) changes in HIV testing patterns. Across the clinics, the criteria for inclusion remained the same over time, and the proportion of the sample that had a diagnosis of any STI was very similar across the three times in Auckland and Christchurch; hence comparability is likely for these centres. As prevalence of known infections was expected to increase from 1996–1997 to 2005–2006, most of the importance can be laid on trends in undiagnosed HIV infection. 12 As clinical testing in sexual health clinics also increased across the latter time periods, if the incidence of HIV infection had remained constant between these periods, the prevalence of undiagnosed infection would have been expected to decrease. In fact, the prevalence of undiagnosed infection increased among MSM in Christchurch and Auckland, from 18.9 to 24.1 per 1000, although not significant (P = 0.70). Overall, this suggests that the incidence of HIV among MSM has increased, although with such a small number it is not possible to be sure.
A striking change between the 1996–1997 and 2005–2006 studies was the increase in the numbers and proportion of attenders whose behaviour was reported as homosexual or bisexual. In the four centres involved in both studies, this went up from 3.7% to 9.1%. While it is possible that MSM in the earlier studies were not identified, this seems unlikely in the context of a sexual health clinic attendance, and if it had occurred, it should have resulted in a spuriously high HIV prevalence previously among heterosexual men that was not seen. An increase in numbers of MSM could have occurred through a lowered threshold for MSM to attend for a sexual health check, but as the proportion of MSM who had a bacterial STI was higher in the latest study, this explanation also looks unlikely. While possibly more MSM were being serologically tested for syphilis in view of the increased number of cases, the rise in syphilis cases had not been limited to MSM; so any increased testing should have applied to all. 13
The two most likely reasons for an increase in MSM attenders are that there has been a real increase in men having sex with other men in the population, or that risk behaviour among MSM has increased resulting in more men seeking health checks. While these reasons cannot be examined in this study, or directly in New Zealand, in two population-based UK studies of sexual behaviour undertaken in 1990 and 2000, an increase in men reporting any same sex experience in the previous five years was found. 14 Although increased willingness to report this behaviour due to a more liberal social environment might have been a factor, the authors believed that ‘some increase in the population numbers of MSM and/or the prevalence of risk behaviour among MSM is overwhelmingly likely’. Similar findings of an increase in the number of MSM are said to have been found in the US. 15 Behavioural surveillance among sentinel populations of MSM in Australia 16 and the UK 17 (this was only started in New Zealand in 2002) also found an increase in STI risk behaviour from 1996 to 2001. Interestingly, in comparable HIV prevalence studies undertaken in UK sexual health clinics outside London, a steady increase in the number of MSM was noted between 1996 and 2005. 18 Because of the increase of MSM in the sample, the increase in the prevalence (as a proportion) of undiagnosed HIV among MSM was accompanied by a more major increase in the prevalence of HIV as a number. That is, the increase in Auckland and Christchurch was from 18.9 to 24.1 per 1000 but from 3 to 13 new diagnoses.
Overall, the findings pointing to an increase in incidence of HIV among MSM are consistent with those from national surveillance of a sustained increase in the number of new diagnosis of HIV among MSM in New Zealand since 2000. 19
The low prevalence detected among heterosexuals across all ethnic groups is reassuring. Even among the groups with the lowest rate of clinical testing, where there remains concern for a major increase in infections, the true prevalence was very low.
IMPLICATIONS
The increase in prevalence of undiagnosed HIV among MSM is compatible with an increase in clinical diagnoses and a real increase in HIV incidence in this group. This indicates a need for further HIV prevention that should focus on men aged in their 30s and 40s.
While the rates of clinical testing have increased since the last study in 1996–1997, they remained low among Pacific people and in Auckland clinics. It was also found that those most at risk of HIV are less likely to be tested. The Auckland clinics have responded by changing their policy and making HIV testing the normal standard of care. The Ministry of Health has also developed new recommendations for HIV testing which include testing for all persons seeking assessment for sexually transmitted infections. 20
The study showed a marked increase, both in total numbers and proportion, of MSM attending sexual health clinics. Whether this reflects an increase in MSM in the population or an increase in sexual risk behaviour, or both, is not certain and needs to be explored in further studies. Improved surveillance of other STIs in MSM would help to determine whether sexual risk behaviour is increasing.
While the prevalence of HIV among heterosexual men and women in this study was low, with the increasing number of heterosexuals being diagnosed with HIV in recent years this situation could change rapidly. Repeating this unlinked anonymous survey will be necessary not only to assess the extent of spread within the heterosexual community but for the ongoing monitoring of overall HIV prevalence in New Zealand.
Footnotes
ACKNOWLEDGEMENTS
This study was funded by the New Zealand Ministry of Health. We would like to thank Ms Helen Brady for the sample testing and all the staff of the sexual health clinics and laboratories for their assistance in making this study possible.