
Abstract
A retrospective analysis of patients, who have been on long-term suppressive therapy for recurrent episodes of herpes simplex (HSV) in a university hospital, was performed and the findings were documented and orchestrated into bar graphs. The study involved patients between the years 2000 and 2007, both inclusive. The results were compared with the British Association for Sexual Health and HIV guidelines. Eighty-two percent (57) had had the infection for at least 12 months at the start of therapy and 78.2% (54) had at least six recurrences per year before the start of treatment. Indeed, only four patients (5.8%) had a treatment interruption at 12 months or less; also only 11 patients (15.9%) had less than six outbreaks per year at the start of treatment. The former is not in-line and the latter is in-line with the guidelines.
INTRODUCTION
Herpes simplex virus (HSV) infection is the most common ulcerative sexually transmitted disease (STD) in the UK, accounting for 10% of new diagnoses made in genitourinary (GU) medicine clinics in 2006 (HPA). 1
In 2006, there were 21,698 cases of primary HSV in the UK. 1
British Association for Sexual Health and HIV (BASHH) guidelines, 2 revised in 2007, recommend an aciclovir dose of 400 mg twice daily (b.i.d.) or 200 mg four times a day (q.i.d.) as the accepted long-term suppressive therapy for HSV. 2 Valaciclovir 500 mg is the only approved drug for once daily (o.d.) dosing.
BASHH guidelines stipulate that long-term prophylaxis of HSV is recommended only in those who have had a minimum of six recurrences per annum. 2 Also recommended, in the guidelines, is that antiviral therapy should cease after 12 months and then recurrence frequency should be re-assessed with patients experiencing unacceptably high rates of recurrence restarting suppressive therapy. The minimum period following discontinuation of treatment should include two outbreaks. 2
METHODS
This is a retrospective questionnaire-based study from all records of those on long-term HSV prophylaxis and attending a GU medicine clinic between years 2000 and 2007, both inclusive. Thus, a given patient could be starting therapy, or otherwise could have been on prophylaxis for a period of up to seven years.
Age, gender, HSV type, history of sexually transmitted infection (STI) screens being carried out, sites of infection, % culture positive, length of history before starting therapy, number of outbreaks per annum before treatment, planned treatment interruption ever, timings of interruptions details, outbreaks per annum off-treatment, breakthrough outbreaks ever details, number of outbreaks per year in last 12 months, total length of treatment, immunosuppressed percentage, percentage on valaciclovir or aciclovir were all tabulated and recorded (see Results).
RESULTS
A total of 69 patients were included in the study ranging in age from 19 to 62 years with a mean age of 37.2 years and a median of 32.5 years; 44.1% (30) were males and 55.9% (39) were females. Most of the patients (90%) had an STI screen at any time, while 10% (7) did not have a screen. Of those who did not have a screen, five of them refused screening. Among those who had a screen, only 63.2% (43) had a positive culture for HSV. Type 2 herpes simplex was cultured in 49.3% (34) of the cases with type 1 making up 8.7%; the remainder were untyped. The commonest site of infection was the genital area (75.4%) with the buttocks being the second commonest site (8.75%); genitals and buttocks affected = 4.3%; ano-genital = 7.2%; limbs affected = 1.4%.
Most of our patients (75.4%) had had the infection for 12 months or more at the outset, only 7.2% (5) had had it for less than six months, and with 13% between six and 12 months; 78.2% (54) had suffered at least six or more recurrences of the infection at the outset (Figure 1). There were no planned drug interruptions in 78.2% (54); 10.1% had interruptions for more than two years; 8.7% had an interruption between one and two years and 5.8% had it at less than one year (Figure 2).
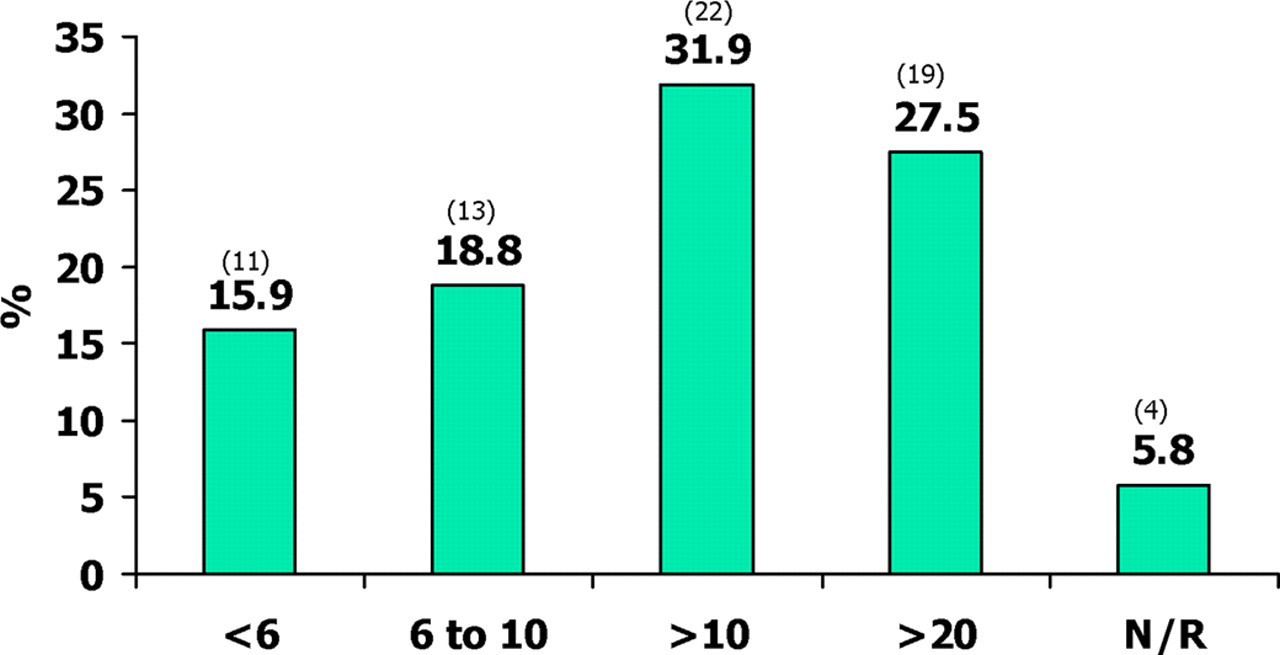
Percentages of total with numbers of outbreaks per year before treatment
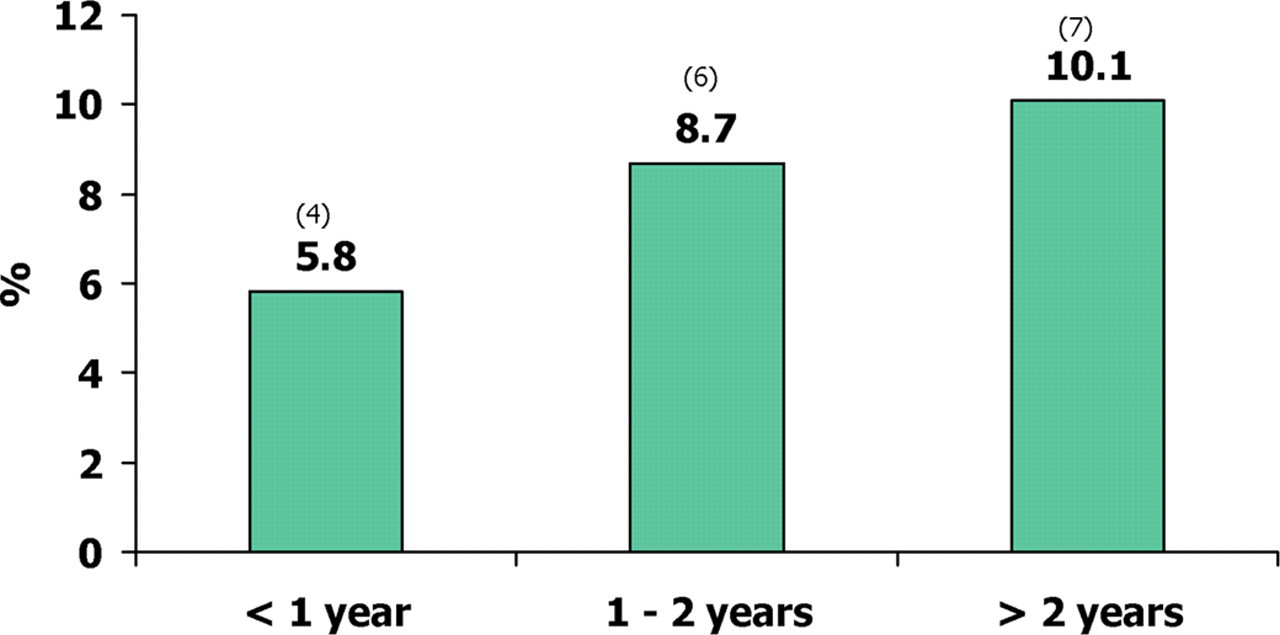
Percentages of total having treatment interruptions at fixed intervals in three categories of time periods
In all, 46.4% (32) report on treatment outbreaks with 21.7% reporting an outbreak of one episode in the last 12 months.
In all, 33.3% (23) had been on treatment for less than a year; 27.5% for between one and two years and 20.3% for three to five years and 15.9% for more than five years (Figure 3).
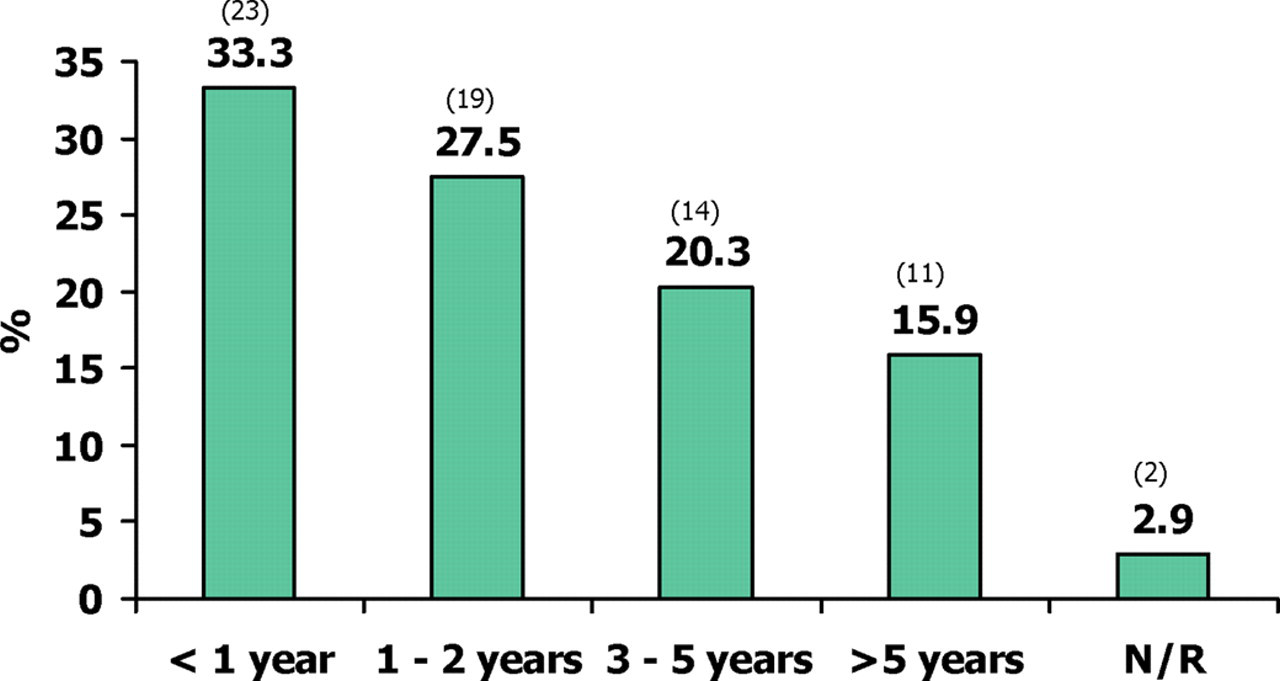
Percentages of total, as at 2008, with periods of treatment altogether in five categories
Immunosuppression due to any source was found in 11.8% with all the cases due to HIV or steroid concomitant therapy.
As recommended by BASHH, 94.1% were on aciclovir 400 mg b.i.d., the rest were on valaciclovir 500 mg per day. One patient recorded intolerance to aciclovir.
DISCUSSION
Primary psychological factors such as extreme anxiety and fear prejudiced against the patients, with less than six outbreaks per annum, having aciclovir withheld at the start. Patients expressed severe reservations about ceasing prophylaxis on a trial basis after a 12-month prophylactic period. Indeed, a total of only four patients had a treatment interruption in the period of 12 months or less. Subjectively, on prolonged discourse with patients, the longer the history of HSV in total, or the older the patients at initial consultation, the less likely they are to be compliant with planned strategic treatment interruption at 12 months as recommended by BASHH guidelines. 2 Indeed, in this cohort, we have prescribed long-term suppressive therapy for up to seven years without untoward events. In particular, there is no evidence of HSV resistance in our cohort.
As supported by our audit, viral culture is not a sensitive tool for the detection of HSV. A better tool is polymerase chain reaction with improved sensitivity of 57% compared with 34% for viral culture. 3