
Abstract
Disseminated mucocutaneous herpes simplex virus (HSV) infection in an immunocompetent person is quite rare. A 19-year-old healthy Japanese woman presented with painful, umbilicated vesicles and pustules on her genital region, both nipples and on the forearm 10 days after the last sexual contact with her partner who had cold sore at that time. Tzanck test and biopsy confirmed the diagnosis of disseminated mucocutaneous HSV infection. She did not have any visceral HSV disease. Skin lesions improved after treatment with acyclovir and erythromycin for seven days. We propose that like herpes gladiatorum, HSV dissemination in this case was acquired by close body contact.
INTRODUCTION
Disseminated mucocutaneous herpes simplex virus (HSV) infection is an uncommon complication of primary HSV infection. It is usually seen in immunocompromised patients, newborn babies, pregnant women or in patients with skin barrier disorders such as atopic dermatitis or Darier's disease, but the manifestation of this disease in an immunocompetent person is quite rare. Herein, we report a case of non-fatal disseminated mucocutaneous HSV-1 infection in a non-pregnant, immunocompetent woman.
CASE REPORT
A 19-year-old Japanese woman admitted to our hospital with painful lesions on her genital region, both nipples and on the forearm, arising a week before. She did not have any particular past medical history. Her last sexual contact was with her partner 10 days before admission. Her partner had cold sore at that time. Physical examination upon admission showed many pustules with crusts on both sides of the nipples and areolae (Figure 1A). Swelling of the vulva with numerous pyogenic erosions and ulcers was observed (Figure 1B) and umbilicated pustules were also observed on her chest and forearm (Figure 1C). Tzanck test from the chest pustule revealed giant cells with neutrophils. Skin biopsy performed from the forearm lesion revealed multinucleated keratinocytes with inclusion body in the epidermis associated with infiltration of lymphoid cells in the dermis (Figure 2A). Immunohistochemical studies showed that these giant cells stained positively with anti-HSV-1 antibody (Figure 2B). Laboratory tests at admission revealed a WBC count of 12,000/mm3 and C-related protein of 3.9 mg/dL. Liver and renal functions were normal. The serological test for HSV-immunoglobulin (Ig)G and IgM were negative. These findings led to the diagnosis of disseminated primary mucocutaneous HSV infection. Treatment was started with acyclovir (5 mg/kg every 8 hours) and erythromycin (500 mg every 6 hours) for seven days. Her skin lesions improved and the WBC count became normal 10 days after admission.
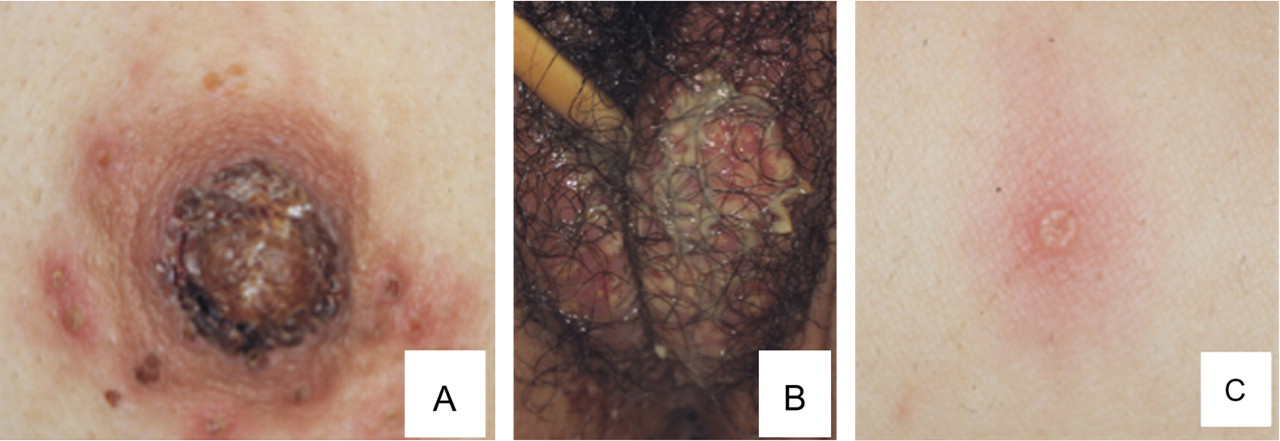
Clinical features. (A) Many pustules with crusts on both sides of the nipple and areola. (B) Swelling of the vulva with numerous pyogenic erosions and ulcers. (C) Umbilicated pustules on the chest and forearm
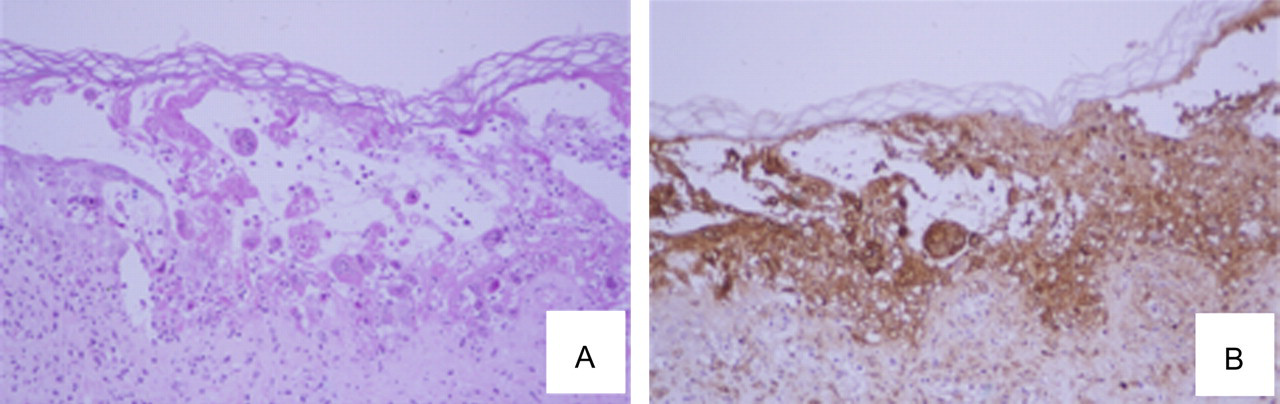
(A) Biopsy specimen from the forearm lesion revealed multinucleated giant cells with inclusion bodies in the epidermis associated with infiltration of lymphoid cells in the dermis (haematoxylin–eosin stain, ×40). (B) Immunohistochemical staining against HSV-1 (×40)
DISCUSSION
HSV-1 and HSV-2 are large double-stranded DNA viruses and belong to the Herpes viridae family. HSV-1 infection is mainly acquired during childhood and its primary infection and reactivation usually causes limited oral or labial disease. On the other hand, HSV-2 is the main cause of genital herpes and is transmitted by sexual contact. 1 Although dissemination of mucocutaneous HSV infection is a rare condition, impairment of the skin barrier function or systemic immune deficiency are causes of clinical manifestation.
Dissemination of HSV from the primary site of infection associated with pre-existing skin disorders such as atopic dermatitis, Darier's disease and mycosis fungoides is known as Kaposi's varicelliform eruption or eczema herpeticum. 2 Dissemination of HSV in eczema herpeticum is usually limited in cutaneous lesions and is controllable by anti-herpes virus agents like acyclovir or valacyclovir, but in some cases, it may progress to fulminating, life-threatening infections and can have severe complications, including herpes keratitis, disseminated infection with visceral involvement, and in some cases with fatal outcome. 3
Disseminated mucocutaneous HSV infection is also observed in patients with underlying immunocompromised conditions like haematopoietic disorders, after bone marrow or solid organ transplantation, 4 usage of steroids, other immunosuppressive drugs and biologics, 5 or in newborn babies as neonatal herpes. 6 In these cases, association of visceral diseases such as encephalitis, hepatitis and pneumonia caused by HSV are sometimes problematic because of the fatal outcome.
Sometimes, disseminated HSV infection occurs during pregnancy. 7,8 The disseminated HSV disease in pregnancy generally occurs in the second or third trimester. It is preceded by a flu-like prodrome, and the clinical presentations are encephalitis, hepatitis, pharyngitis and disseminated skin lesions. About half of the reported cases were reported to be fatal. 8 The cause of dissemination could be explained by the alterations of cellular and humoral immunity during pregnancy.
In the present case, disseminated mucocutaneous HSV infection occurred in a non-pregnant, immunocompetent woman without a history of any primary skin disease. These clinical settings resembled those that are present in the case of herpes gladiatorum, which is a widespread primary inoculation of the HSV infection in athletes with skin abrasion and which occurs by contact with active HSV lesions of others. 9 In herpes gladiatorum, the location of the skin lesions differs markedly from the usual orolabial site of HSV-1 infection. In our case, close body contact with a partner who had herpetic lesion might be a cause of the disseminated skin disease. Nowadays, a delay in the acquisition of oral HSV-1 infection early in life in developing countries results in susceptibility to genital HSV-1 infection at the initiation of sexual activity. 1 Clinicians should be aware of the possibility of disseminated cutaneous HSV infection in healthy adults by sexual contact.