
Abstract
We describe a 37-year-old woman who presented with a painless vulval lump of eight months duration. Excision biopsy revealed a benign lesion thought to be derived from mammary-like glands, which are well-documented in the anogenital region but under-recognized among genitourinary medicine practitioners. Our case highlights the importance of having a low threshold for biopsy of atypical vulval lesions.
CASE REPORT
A 37-year-old woman self-referred to the genitourinary (GU) clinic with history of a genital lump, which had slowly grown in size over eight months. Apart from occasional bleeding, she did not have any symptoms from the lump. She had been married for eight years with no extra-marital sexual contact. There was no previous history of sexually transmitted infections and she did not have any significant past medical history.
Clinical examination revealed a pea-sized nodule, about a centimetre in size, in the periclitoral region (Figure 1). The nodule was firm, non-tender with a slightly erythematous surface. There was no regional lymphadenopathy. Examination of the vagina and cervix was normal and a sexual health-screen was negative. It was difficult to make a clinical diagnosis, as the lump did not have features typical of any of the common vulval lesions, such as warts, molluscum or retention cysts. A biopsy was felt appropriate to ascertain the diagnosis.

Vulval lump with shiny, erythematous appearance
Histopathologically, the lump showed skin with an underlying lesion composed of well-defined apocrine type glands with an inner cuboidal secretory layer and an outer layer of cells probably representing myoepithelial cells (Figure 2). There was no evidence of epithelial atypia or malignancy in the lesion. The lesion was considered to be a tumour of anogenital mammary-like glands based on the histological appearances, which were highly reminiscent of benign nipple adenoma of the breast. The patient was referred to the gynaecologist for complete excision of the lump.
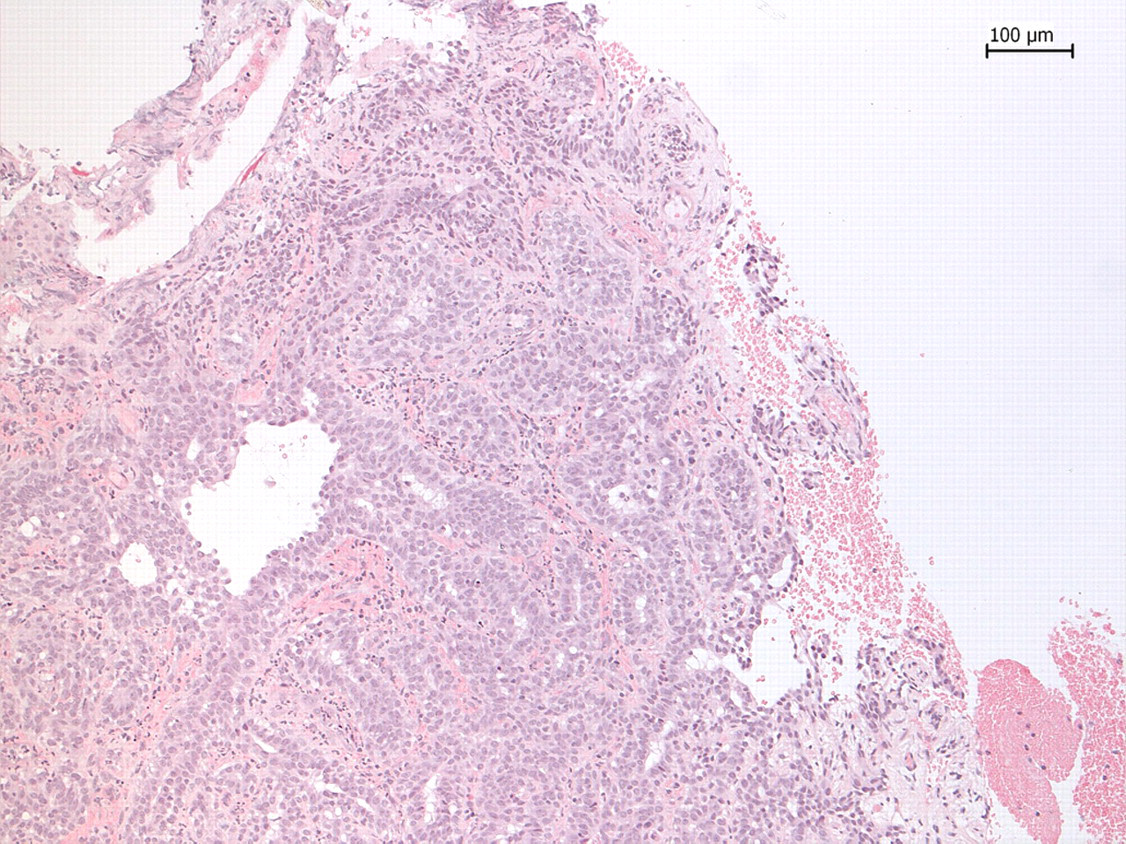
Lesion composed of well-defined apocrine type glands with striking similarity to benign nipple adenoma of the breast
DISCUSSION
‘Mammary-like glands’ are those that resemble mammary glands but are not identical to them. They are recognized as a normal constituent of the anogenital region, the vulva in particular. 1,2 They occur at the surface between mucosa and skin and are typically distributed around anogenital openings. They have a combination of morphological and immunohistochemical features of eccrine, apocrine and mammary glands. They often express receptors for oestrogen and progesterone and these hormones may play a role in their development.
Historically, mammary-like glands were thought to be ectopic breast tissue derived from rudiments of the embryonic milk line. In the females, the milk line has been traditionally hypothesized as a line extending from axilla to medial side of thighs. A review of mammary-like glands and their disorders by Van der Putte in 1994 revealed that such a concept was not supported by embryological evidence. 3 The idea of the milk line extending from axillae to inner thighs was based on observations from pig embryos and is not comparable with human embryos in which the primordium for breasts and vulva remain widely separated in space and time. Consequently, mammary-like glands have been recognized as a distinct entity.
The first ever description of mammary-like glands in the vulva was by Hartung in 1872 who described a lactating breast on the labium majus of a 30-year-old woman. 4 More recently, mammary-like glands have been thought to be the origin of a range of neoplastic (benign and malignant) and reactive conditions with striking similarity to lesions in the breast. They can develop into a lactating tissue, or more commonly, can give rise to hidrocystomas or to adenomas with predominant tubular, papillary, cystic and fibromatous elements. 3 Adenocarcinomas including extramammary Paget's disease originating from mammary-like glands have been reported in the literature. 5–7 These tumours are typically locally aggressive with a low risk for widespread metastasis. 8
Clinical diagnosis of vulval lumps is not always straightforward. Mammary-like glands and lesions derived from them are under-recognized in GU clinics and our case helps to improve awareness of this condition. It also highlights the value of having a low threshold for biopsy of atypical lesions in order to make the right diagnosis. As most GU departments have nurse-delivered clinics, it is particularly important to educate staff to refrain from providing topical wart treatments and cryotherapy to atypical lesions without establishing a diagnosis. This practice will not only mask the clinical picture but also lead to under-diagnosis of such potentially malignant lesions.
Footnotes
ACKNOWLEDGEMENT
We thank Dr Elizabeth Robbins in the Department of Pathology for contributing the slides.