
Abstract
We applied the principles of Hazard Analysis and Critical Control Points (HACCP) to systematically analyse the care pathway of patients diagnosed with gonorrhoea to identify potential intervention opportunities for preventive action. Data were collected on individuals with culture-positive gonococcal infection during 27 February 2003 to 08 January 2004. Qualitative data were gathered within individual semi-structured interviews. Two hundred and twenty-three gonorrhoea patient episodes were evaluated. The median interval between presentation and treatment was significantly longer in females and men having sex with men (MSM), compared with heterosexual men (P = 0.002). Females were significantly more likely to be in regular relationships at the timepoint of perceived infection acquisition than heterosexuals or MSM (P < 0.0001). Four major themes emerged from the interviews: life-stage and infection risk, determinants of risk perception around sexual encounters, attitudes to preventing re-infection and condom use. These informed three potential ‘critical control points’: health-related attitudes/behaviours preceding infection; access to appropriate care and optimizing health promotion to prevent further infection.
INTRODUCTION
Gonorrhoea is a sexually transmitted infection (STI) with dynamic epidemiology. During the late-1990s, gonorrhoea incidence doubled in the UK. 1 Fluctuations in incidence are generally driven by three interacting factors: individual attributes and behaviours, sexual network characteristics and effectiveness of control measures. We investigated the potential role of each factor in Glasgow, where an exponential rise in diagnoses occurred between 1994 and 2000. 2 We combined qualitative and quantitative methodology, using the principles of Hazard Analysis and Critical Control Points (HACCP) to systematically analyse pathways between acquisition of infection to conclusion of clinical care, aiming to identify potential ‘critical points’ for preventive action. 3 Originally used in improving food safety, HACCP identifies key intervention points in complex pathways and uses these to generate evidence-based prevention measures. HACCP principles have been applied to analysis of cancer and orthopaedic care pathways, but not previously in planning sexual health interventions.
METHODS
We applied mixed qualitative and quantitative methods to analyse patient pathways, thus allowing both health-care provider and patient perspectives to be captured and providing a better understanding than either approach alone (Figure 1).

Flowchart showing mixed methodology of study population
Participants
A structured questionnaire was completed by a health-care professional within two weeks of diagnosis for all individuals in whom Neisseria gonorrhoeae was isolated at Glasgow's main bacteriology laboratory during the study period (27 February 2003 to 8 January 2004).
Semi-structured interviews were conducted with a sample of the GUM attendees who presented with a new episode of gonococcal infection. Interviewees were purposively sought, each patient diagnosed with gonococcal infection was asked to participate in a face-to-face interview within four weeks of diagnosis.
Data collection
Demographic characteristics and key health-care outcomes were extracted from laboratory and clinical records. Residential postcodes were classified using the Carstairs deprivation classification. 4
Interviews were tape-recorded and transcribed verbatim (JC), exploring circumstances surrounding sexual encounter/s perceived to have been associated with gonorrhoea acquisition (friendship groups, social activities/venues and substance use); individual reactions and experiences following diagnosis, experiences of using health-care services and attitudes to future gonorrhoea prevention. ‘Time from presentation to treatment’ and ‘time from treatment to confirmation of bacteriological clearance’ were defined as the clinical outcomes of interest (data for these outcomes were obtained from case-notes).
Data analysis
Demographic characteristics and health-care outcomes were compared in three discrete subgroups: women, men having sex with men (MSM) and heterosexual men, using chi-squared tests of association. Care pathways, from presentation of infection to last contact with health services, were analysed using Kaplan-Meier survival methods.
Interview transcripts were analysed (SC) for emergent themes using interpretive phenomenological analysis (IPA). 5 IPA focuses on meanings of events and experiences to participants, using quoted text to illustrate themes representing shared understandings. IPA requires a homogenous sample, therefore analysis was conducted separately for MSM and heterosexual participants. To check consistency and validity of coding, half the interviews were read by another researcher (AS).
RESULTS
Study population characteristics
All 20 interview participants were Caucasian: the majority born in the West of Scotland and lived in Glasgow; 18 were men, of whom seven were heterosexual (Table 1).
Demographic and clinical characteristics of study population
*Numbers do not total 100% as categories not mutually exclusive
GC = gonococcal
Two hundred and thirty-one episodes of gonococcal infection occurred in 226 individuals. Full data were available for 223 first-patient episodes. One hundred and ninety-two (86%) were men, of whom 91 (47.4%) were heterosexual. All 31 women were heterosexual. Thirteen (6%) individuals self-identified as non-white.
About one-third of patients (34.5%) believed they had acquired infection within an established relationship; 19 (61.3%) women, compared with 18 (19.8%) heterosexual men and 40 (39.6%) MSM (P < 0.0001).
The clinical care pathway
The majority (167, 74.9%) presented to GUM for their diagnostic consultation; 49 (22.0%) presented to other sexual health services and 7 (3.1%) to their GP. A significantly higher proportion of GUM clinic attendees received diagnosis and treatment at first presentation, compared with patients who were presented to other settings (144/167 [86%] and 36/56 [64%], respectively, P < 0.0001). One patient defaulted follow-up and remained untreated.
At the time of this study a routine test of cure was recommended in every case of gonococcal infection and was completed in 157 (70.4%) patients. Three individuals required re-treatment, two for ciprofloxacin resistance and one for re-infection.
Figure 2 summarizes care pathways from presentation to two outcomes of interest, stratified by patient and health-care provider characteristics. The median interval between presentation and treatment was significantly longer in women and MSM compared with heterosexual men (P = 0.002).
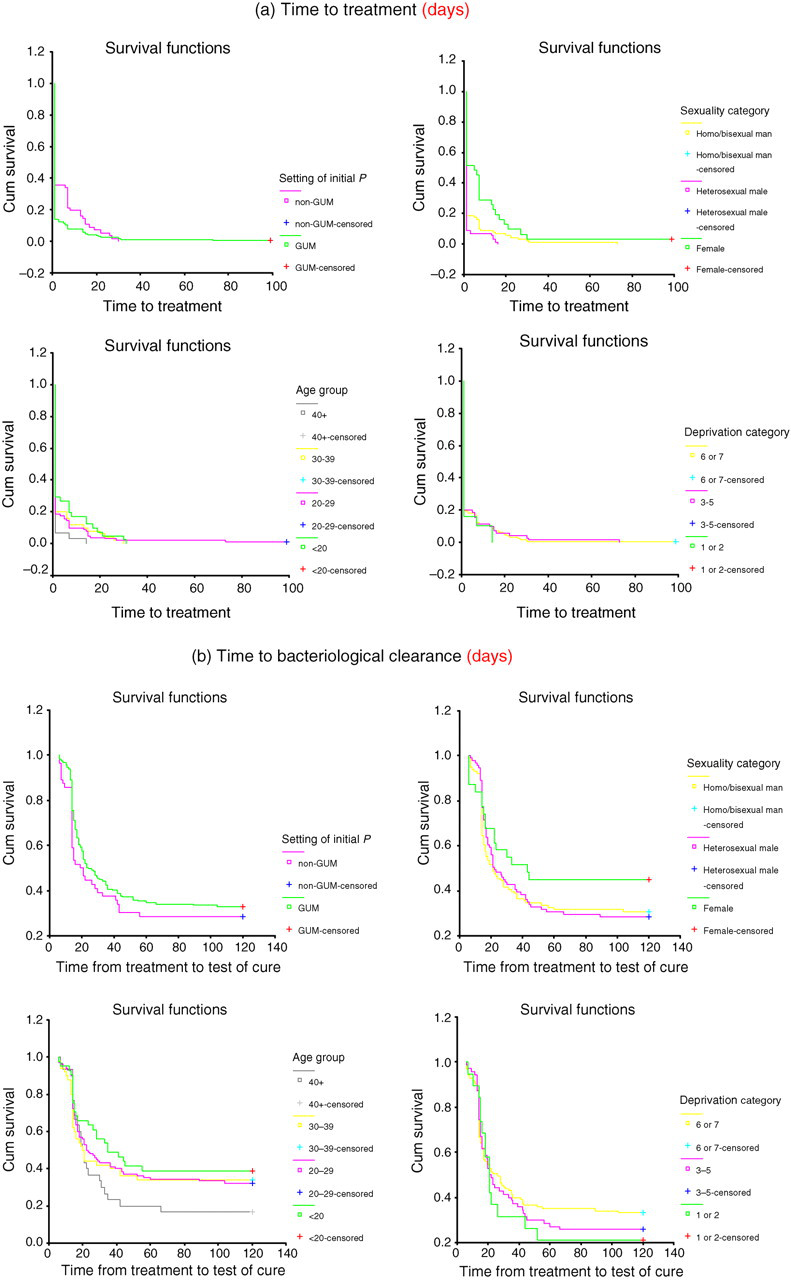
Clinical care pathways of study population
The care pathway: patient perspectives
Four major themes emerged from the interviews, identifying potential critical control points for primary and secondary prevention of gonorrhoea; these comprised the effect of life stage on risk behaviour; perceptions of risk around sexual encounters; intended personal strategies for prevention of re-infection; and attitudes to condom use.
Life stage and risk behaviour
Increased risk activity was associated with key life stages, particularly in heterosexuals, for whom periods of casual sex, increased sexual activity and experimentation were pronounced. For heterosexuals, this was commonly limited to periods outside of relationships and often associated with life stages of ‘youth/student life’ and ‘single again’. Although MSM also described experimentation at life stages, such as ‘coming out’ and ‘youth’ (often coinciding), they were more likely to incorporate concurrency and casual sex into open relationships, suggesting a more uniform pattern of lifetime risk, rather than defined, episodic accentuated periods.
Heterosexual woman (020): ‘I'd never done that before, just met someone and gone home with them like a one night stand…and I was at uni and thought well that's what it's about’.
MSM (055): ‘My boyfriend is 6 years younger than me. He said he wanted to be faithful to me but he's not done it, I can't blame him really cos it's his first time on the scene, he'll want to experiment, much as I wanted to, he'll have to learn the hard way like I did’.
Perceptions of risk associated with sexual encounters
Many participants perceived they had acquired gonorrhoea while in relationships. It was widely perceived that ‘knowing’ someone, even by association through a friend, was associated with cleanliness and safety.
MSM (022): (accounting having unprotected sex with a friend): ‘And when I went to get one [a condom] that night. flavoured, and it was out of date. So and I couldn't find the ones that were in date. So…I thought och, it's Alisdair you know what I mean, we'll be fine. You know.’.
Heterosexual man (044): ‘No, I wouldn't use condoms, no. We are both older people, we've both been married and had children, we didn't think at all that it was relevant for us, condoms are for young kids…’
MSM (037): ‘well I knew it was an infection that I should go straight to the clinic, I did know it would be gonorrhoea but something like that yeah. It's horrible yeah, but you take the pills and it's gone.”
Heterosexual woman (009): ‘Aye, I was really upset about it, I was greetin' aboot it an' that. Thinking I was dead dirty an' aw that, I just thought everybody was going to think I'd slept with hundreds of people when I've no really, I've just slept with two people in my whole entire life…He said he thought he got it from me but he slept with another lassie that's going out wi' noo, behind my back.’
Intended strategies for prevention of re-infection
Several participants spoke of ‘starting afresh’ and that infection had been a ‘wake-up call’:
Heterosexual man (023): ‘Now if I'm going oot on a night oot, definitely [will take condoms]. Know what I mean, but in the past when I was a teenager, I wouldn't even think it. ‘Cause I'm no risking another infection. It could, you don't know what could be next. It could be something bad, untreatable.’
However, several participants reported ineffective future prevention strategies, many still relying on the assumed visibility of infection.
Heterosexual man (068): I mean I think I could tell easily. I'm no being big heided at this point but, I could tell [if someone had an STI] if I've been out and say there's a- like a girl and she basically- she's hanging all over me and the way she's acting and things she might dae or things she might say to me, well, I know that you've slept with a lot of people and I just know…I'll just I'll say to myself in ma heid I know you've slept with a lot of people, and eh, I won't be taking your number or I won't be doing anything else wi’ ye.
MSM (008): I think these days I'd probably tend to go more for somebody that I've known for a while. If I was given a choice of a really nice stranger or a really nice person I've known for a few years, I would go for the person I've known for a few years…cos it's safer, I'm more likely to know their history.
Condom use
Most participants reported inconsistent/absence of condom use, frequently attributed to alcohol consumption:
MSM (038): I won't have unprotected sex sober. I won't do it but when I'm drunk you just don't think about stuff like that.
Many men (MSM and heterosexual) displayed a profound vulnerability and lack of decision-making around condom use. Several reported they would have used condoms if their partner had asked, and reported waiting for cues. This could be related to lack of confidence, not wishing to ‘spoil the moment’ or to avoid suggesting that their sexual partner may be infected. A clear lack of experience with negotiating or creating dialogue around condom use was evident. While this supports literature that men often assume women to take responsibility for sexual health, this was also found for MSM, suggesting that a broader vulnerability exists for men in general. Several men's accounts suggested passivity:
Heterosexual man (026): No, never used condoms. Unless the girl went – no not without this’ know what I mean? …’.
MSM (038): Em, I did suggest using one but I got no reply and I suggested again and got no reply so I just thought, he's not bothered so that was that…I, I tend to…it depends on what mood I'm in…sometimes I'll just not bothering about it and sometimes I'll like go for one, sometimes I'll use one, sometimes I'll suggest it but whatever, but if they say no then I just don't.
DISCUSSION
We applied the principles of HACCP analysis to systematically identify critical points in the gonorrhoea care pathway, representing potential intervention opportunities over a one-year period of incident infection in Glasgow. Use of complementary qualitative and quantitative methodologies created a rich understanding of patient journeys from both patient and provider perspectives.
Three critical control points were identified from our analysis: first, health-related attitudes and behaviours preceding infection, potentially modifiable by social marketing approaches; second, improved access to appropriate clinical care (currently optimized in GUM settings); third, opportunities for secondary gonorrhoea prevention within clinical consultations (Figure 3).

Critical control points identified for primary and secondary prevention of gonorrhoea
Health-related attitudes and behaviours preceding infection
We found evidence of social patterning of attitudes and behaviours with sexual orientation. Our observations suggested the importance of targeting sexual health promotion towards heterosexual individuals at critical life stages, particularly those entering teenage transition, students, those who are ‘single again’ and older people who may not feel themselves to be at risk of STIs. However, as one-third of individuals in our study population acquired infection while in an established relationship, the continuing need for regular sexual health screening should be emphasized for those in new relationships.
Social marketing 6 for gonorrhoea prevention in MSM should aim to promote a culture, which can embrace both sexual freedom and safer sex, recognizing that partner concurrency and ‘low-risk’ sexual practices remain associated with risk of STI acquisition. Social marketing should also promote gay culture that gives space for those wishing to pursue monogamy.
Assumptions of safety with social familiarity were widely held in this study. Social marketing approaches could be designed to challenge the misconception that people who are ‘known’ socially represent low-risk for STI acquisition.
Improving access to high-quality clinical care
A significantly higher proportion of GUM clinic attendees were diagnosed and treated at their first clinical presentation, compared with patients attending other settings. While it is recognized that uncomplicated STI care can be delivered to high standards in other settings, this study demonstrates that specialist services currently reduce time to diagnosis and treatment of symptomatic patients. The median interval between presentation and treatment was significantly longer in women and MSM.
The need for specialist referral for all individuals with possible gonococcal infection should in the future be diminished with wider use of non-invasive nucleic acid amplification tests. This should substantially shorten time to diagnosis in those with asymptomatic and microscopy-negative gonococcal infection and will also allow sampling techniques with superior patient acceptability, including self-collected vulvo-vaginal swabs and male urine samples. 7,8
Optimizing health promotion opportunities in clinical consultations
Our study identified profound vulnerability and lack of decision-making around condom use in both heterosexual and MSM. There is good evidence that sexual health promotion interventions in clinical settings can support patients with changing their sexual behaviour, including increased condom use. 9 Condom use including appropriate use for oral sex should be explored at the first clinical consultation, given that about one-third defaulted follow-up.
Clients also need to have a correct understanding of effective disease prevention, as opposed to relying on intuition about risk.
Our use of HACCP analysis afforded rich insights into the patient journeys associated with gonorrhoea acquisition and its subsequent management, which can directly inform prevention strategy in Glasgow. HACCP approaches offer considerable potential in sexual health improvement, especially for bacterial STIs, where many interacting social, behavioural and organizational factors contribute to the eventual outcomes of care.
Footnotes
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the contribution of Maureen Kennedy, our research nurse, Mark Mason, MLSO and Chris Thow, IT support.