
Abstract
A 20-year-old man presented with a five-week history of an eruption of papules and nodules disseminated over his body and face. We propose that this patient has a late form of secondary syphilis with a nodular, granulomatous inflammation in urgent need of treatment. Otherwise late irreversible sequelae could develop and unwanted possible further sexual transmission could take place.
CASE REPORT
A 20-year-old Moroccan homosexual man presented with a five-week history of an asymptomatic eruption on the face, trunk and extremities (Figures 1–3). The patient did not have a history of a painless genital sore. He was healthy and did not use any medication.

Papules and nodules with an erythematous, livid appearance on the face (with permission from the patient)

Papules and nodules with an erythematous, livid appearance on the trunk (with permission from the patient)

Papules and nodules with an erythematous, livid appearance on the legs (with permission from the patient)
He first presented at the first aid department, where he was suspected of having chickenpox. Because of his promiscuous sexual behaviour he was referred to the Department of Sexually Transmitted Diseases (STD) for additional screening.
Physical examination showed an apparently healthy man, with multiple small, solid, dull-red papules and nodules, distributed across the face, trunk and extremities. The scalp was not involved. No ulceration or alopecia was noted. The palms, soles and mucous membranes were spared. There was mild inguinal lymphadenopathy.
A routine venereological screening was carried out. Because of clinical suspicion of secondary syphilis, a rapid plasma reagin test was done, which was strongly positive (3+). Furthermore, 4 mm punch biopsies were taken.
Preliminary conclusion: atypical secondary syphilis. Treatment: 2.4 million units of benzathine penicillin (Penidural®) i.m.
Laboratory results: Venereal Disease Research Laboratory (VDRL) 1:64, fluorescent treponemal antibody absorption (test) positive, treponema screen assay (TSA)-ratio 7.3, HIV-antibodies negative.
Haematoxylin and eosin stain (Figures 4 and 5) showed some hyperkeratosis and a perivascular mixed dense inflammatory infiltrate extending into the deep dermis. It consisted of lymphocytes, plasma cells, eosinophils, as well as large numbers of histiocytes and some multinucleated giant cells, with foci of a granulomatous inflammation, without central necrosis.
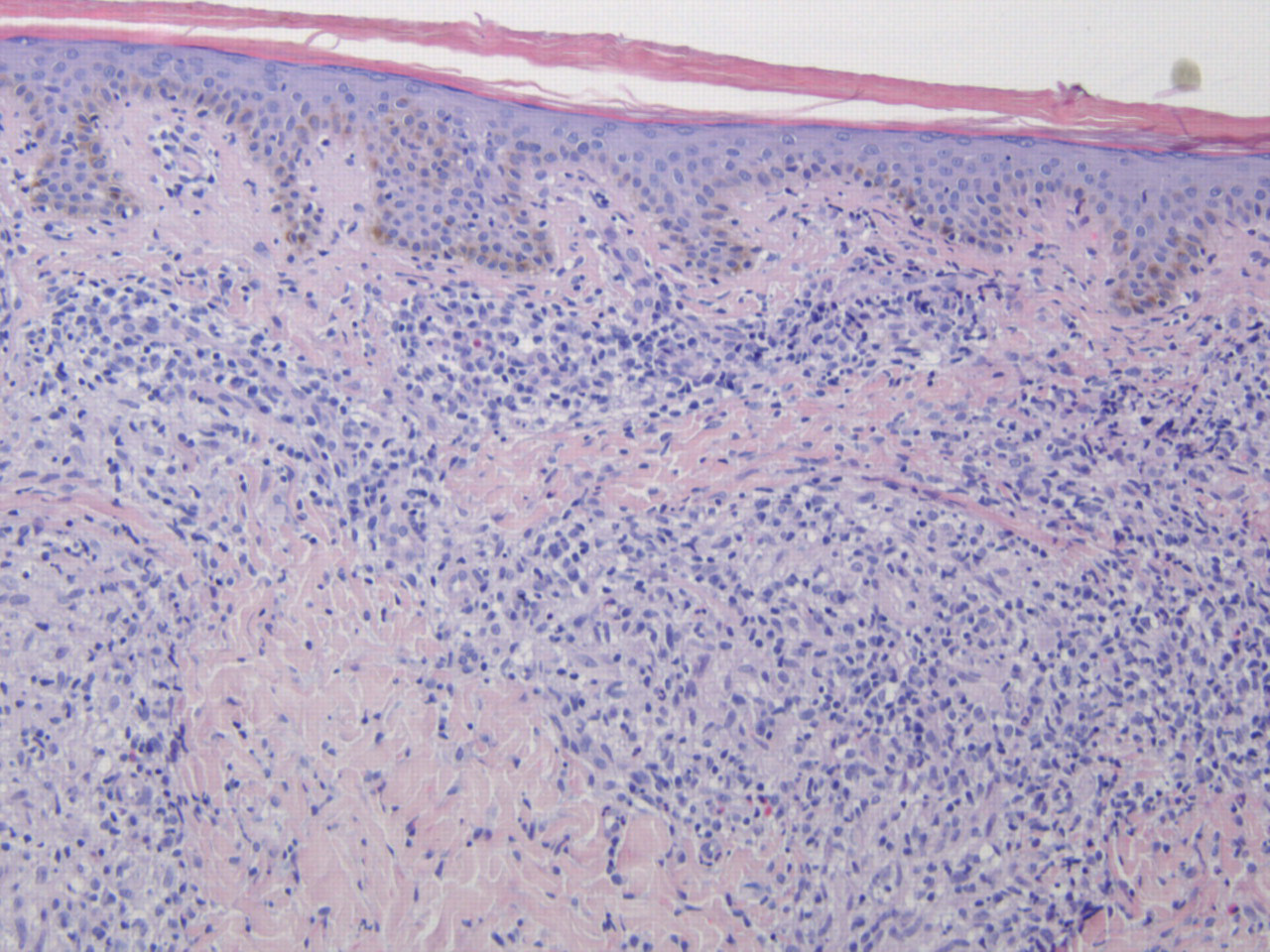
Haematoxylin-eosin stain (original magnification × 10)
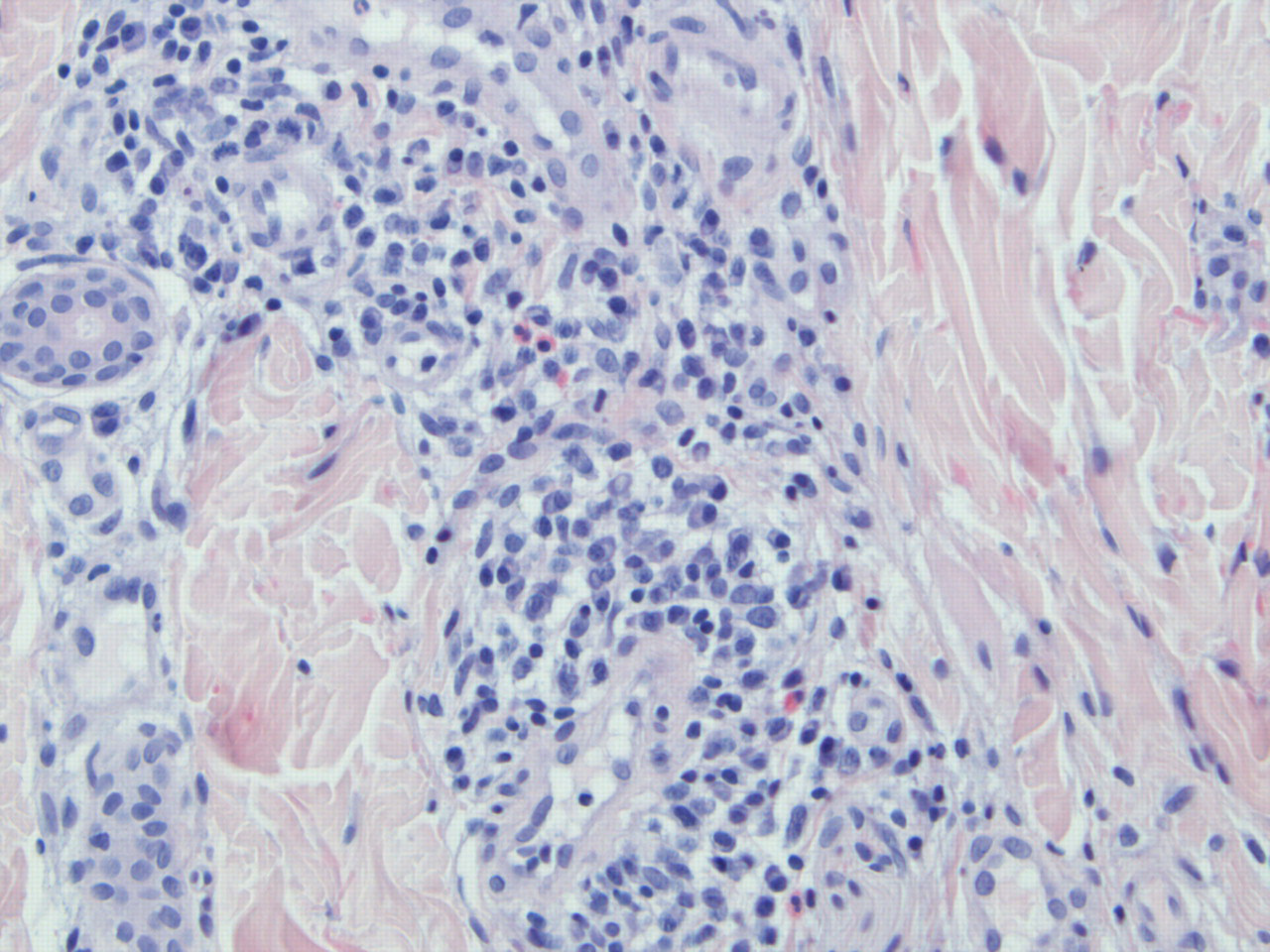
Haematoxylin-eosin stain (original magnification × 20)
Immunofluorescence (Figure 6): positive staining of numerous spirochetes fluorescin isothiocyanate labelled antibodies against Borrelia burgdorferii were used, with a known cross-reactivity with Treponema pallidum).
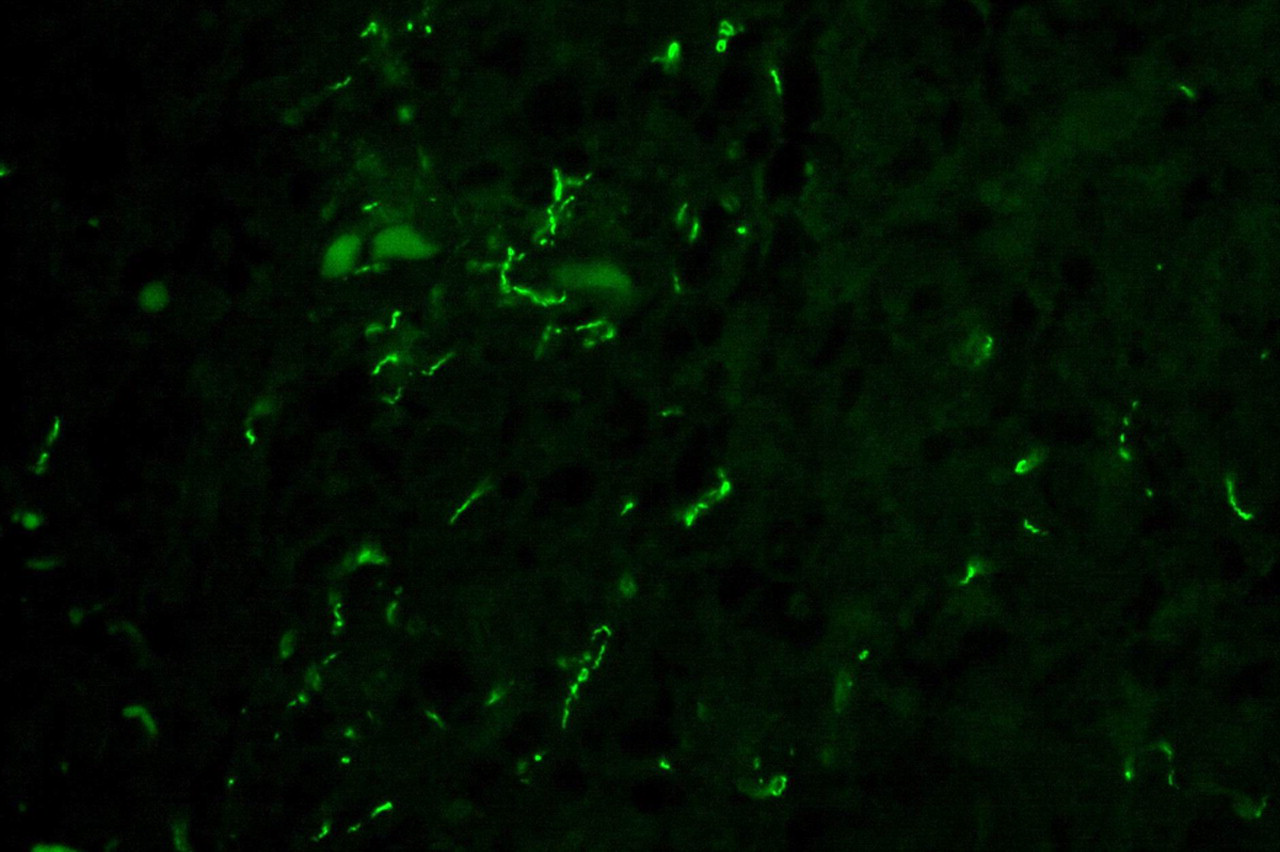
Immunofluorescence test (original magification × 60)
Six weeks after treatment, all papules and nodules had disappeared. VDRL titre after six weeks had fallen to 1:16, to be repeated on a regular basis for testing of the final efficacy of our therapy. The patient was advised to have a repeat HIV-test in three months' time.
DISCUSSION
The lesions of secondary syphilis correspond to an early phase of maculae, a later phase with papules and sometimes nodules and the development of the final stage (tertiary syphilis) of gummata and/or ulcerate forms. In the first stages, spirochetes are widely disseminated through the whole body. In case immune response and/or therapy is inadequate, late syphilis will develop in nearly every organ. 1 For this, syphilis is known as the ‘Great imitator’. 2
Secondary syphilis more typically manifests itself as generalized papulosquamous lesions, often also located at palms and soles (‘roseoles’), sometimes accompanied by fever, lymphadenopathy, weight loss, arthralgias and myalgias. 3 These papulo-erythemato-squamous manifestations can even mimic ordinary psoriasis. 4 The differential diagnosis of late secondary syphilis, overlapping histopathologically with tertiary syphilis includes deep mycoses, leprosy, tuberculosis, sarcoidosis and lymphoma. 5 A papular nodular manifestation was present in our patient. Because of the wide differential diagnosis we performed a biopsy. Nodular presentations have demonstrated granulomata, as in our patient and pseudolymphomatous histology. 6,7
Though nodular lesions are usually a manifestation of tertiary syphilis and occur infrequently, they have also been described in secondary syphilis. 4,8–13 In the course of the late secondary stage, nodular and ulcerated lesions may arise as precursors of the tertiary stage. 1,5 In histopathology, it can be difficult to make the correct diagnosis. In the case of early secondary syphilis treponemas can be easily detected. However, as granulomas develop in the overlap from secondary to tertiary syphilis, the density of T. pallidum diminishes. Immunofluorescence (Figure 6) is a highly sensitive and specific technique to demonstrate bacterial or viral antigens in the skin. 14
Nodular syphilis is an uncommon manifestation of secondary syphilis and may therefore be unrecognized. It is of great importance that non-venereologists especially, will include secondary syphilis in their differential diagnosis. The clinical and histological features of different stages may overlap. In these cases, characteristics of both phases can be seen. In our patient there was an overlap of secondary and tertiary syphilis, reflected by the presence of both lymphocytes and histiocytes in the inflammatory infiltrate and the formation of granulomas. This histopathological granulomatous reaction explains the clinical presentation with papules and nodules. The dynamic course of all phases, often mentioned as the ‘life of lesions’ of syphilis should be considered when making a differential diagnosis. Good clinical practice means an extensive differential diagnosis followed by careful clinical and laboratory investigations to make the correct diagnosis. This case illustrates that a narrow scope gives syphilis the chance to develop into a granulomatous stage and an unwanted lengthy exposure time for further sexual transmission.