
Abstract
China's National Pediatric ART Program began in 2005, in which 32 ART-experienced and 51 antiretroviral therapy (ART)-naïve children received paediatric formulations of (zidovudine or stavudine) plus lamivudine plus (nevirapine or efavirenz). Reverse transcriptase sequencing and analysis was performed on plasma samples with >1000 HIV copies/mL after one year of treatment. Thirty-four samples were sequenced. Nearly all patients had nucleoside reverse transcriptase inhibitor and non-nucleoside reverse transcriptase inhibitor mutations. High/intermediate resistance was found to lamivudine/emtricitabine in 31 patients; to didanosine, abacavir, stavudine and zidovudine in 18 patients; and to tenofovir in 11 patients. All had high-level resistance to nevirapine; all but one had high/intermediate-level resistance to efavirenz. Viral load was the only cohort characteristic significantly associated with developing resistance. Resistance to zidovudine, stavudine and tenofovir was more common in ART-experienced versus ART-naïve patients (P = 0.02–0.05). Drug resistance is high in this cohort. Second-line therapy will require additional ART strategies and options, which are currently unavailable in most developing settings.
BACKGROUND
Approximately 2.3 million children are living with HIV globally. 1 Although access to highly active antiretroviral therapy (HAART) has been limited in the developing world, 2 several initial treatment programmes have begun in recent years. Unfortunately, drug resistance is common among children receiving antiretroviral therapy (ART) in both developed and developing settings and may be more prevalent than resistance in adults. 3,4
China began its National Pediatric HAART Program in July 2005 with a pilot programme of 83 children in a high-prevalence, rural county. The clinical, immunological and virological outcomes of this cohort have been reported elsewhere. 5 Briefly, median CD4 counts initially increased and median viral loads decreased significantly; however, median CD4 counts plateaued and viral replication increased after approximately six months of therapy, suggesting that many children might have developed drug resistance. After one year, 41 children (49.4%) had >1000 copies/mL of RNA (21 of the 32 with ART experience; 20 of 41 previously ART naïve). Eight children (19.5%) had 1000–9999 copies/mL, 11 (26.8%) had 10,000–99,999 copies/mL and 22 (53.7%) had ≥100,000 copies/mL. This paper presents the results of genotype testing on children with viral loads of >1000 copies/mL after taking HAART for one year to determine drug resistance mutations and direct future therapeutic choices.
METHODS
Cohort
All participants were treated at the Chinese Center for Disease Control (CDC) clinic in Shangcai County, Henan Province, which is a poor, rural area heavily affected by contaminated blood and plasma donation in the mid-1990s. Clinicians were trained through the National Pediatric HAART Programme in paediatric-specific HIV/AIDS treatment and care. The median age of the cohort was 11 years (interquartile range [IQR] 7–13) and 69% were male. Thirty-two children had previously taken adult formulations of ART and 51 were ART naïve. Since enrolment, all children have been treated with the paediatric formulations available in China: (zidovudine [AZT] or stavudine [D4T]) plus lamivudine (3TC) plus (nevirapine [NVP] or efavirenz [EFV]). Prior treatment in the ART-experienced cohort consisted of adult formulations of (AZT or D4T) plus (didanosine [DDI] or 3TC) plus NVP. Exact dosing is unknown and likely variable. The median duration of prior treatment was 59.0 weeks (IQR 44.1–80.3). These children were continued on their prior regimens using weight-adjusted paediatric doses, with the exception of substituting 3TC for DDI due to drug availability. There were no disruptions in ART supply, and the children received intensive clinical evaluation as well as adherence support for the first six months of the programme.
Laboratory techniques
As part of the national treatment programme, CD4 count was determined locally from whole blood by FACSCount (BD Biosciences, NJ, USA). Plasma was separated, kept at 2–8°C and transported to the Beijing Ditan Hospital's Laboratory within 24 hours for viral load testing using the COBAS Amplicor HIV-1 Monitor Test (Roche, CA, USA) according to the manufacturer's instructions.
Plasma samples were stored at −70°C. RNA was subsequently extracted using QIAamp Viral RNA Mini Kits (Qiagen, CA, USA) according to the manufacturer's instructions. For this analysis, protease was not analysed as protease inhibitors were available in China until 2005. The polymerase chain reaction products showing the expected band were sequenced by the Sangon Company (Shanghai, China) using an ABI PRISM 377 DNA Sequencer (AME Bioscience, Toroed, Norway).
Sequence analysis
Chromatograms were analysed using Chromas software (Technelysium Pty Ltd., Queensland, Australia). Sequences were compared with the HIV type 1 (HIV-1) clade B consensus sequence, and differences in amino acid sequences, including positions that contained a mixture of wild-type and mutant residues, were classified as mutations. HIV drug resistance mutations were identified using the Stanford University HIV Drug Resistance Database (
Statistical analysis
Drug resistance was analysed with descriptive statistics. Comparisons between ART-experienced and previously ART-naïve children were made using the t-test, Fisher's exact test and Mann–Whitney U test. Cohort characteristics were analysed for association with the development of resistance using univariate and multivariate logistic regressions. Results were considered statistically significant with a P value ≤0.05. Analyses were conducted using SAS (NC, USA).
Study conduct
Caregivers for all patients consented to participation in the National Pediatric HAART Programme, and the Chinese Ministry of Health and CDC Institutional Review Board approved this study.
RESULTS
Resistance testing was successful in 34 of the 41 patients (25 ART experienced and 9 previously ART naїve). Four archived samples with low viral loads failed to amplify on multiple attempts. Three samples that amplified, failed to give sequences. These genotypic failures were due to inadequate sample. All isolates were subtype B.
Nucleoside reverse transcriptase inhibitor (NRTI) and non-nucleoside reverse transcriptase inhibitor (NNRTI) mutations are presented in Figure 1. When comparing the frequency of individual NRTI mutations between ART-experienced and previously ART-naïve patients, no statistically significant differences were found. However, when grouping all thymidine analog mutations (TAMs: M41L, D67 N/G, K70R, L210W, T215F/Y, K219E), more were found in the ART-experienced patients (46 TAMS/25 patients versus 9 TAMS/9 patients, P = 0.05). In analysing NNRTI mutations, the only statistically significant difference was Y181C being more common in previously ART-naïve patients compared with ART-experienced patients (77.8% versus 36.0%, P = 0.05).
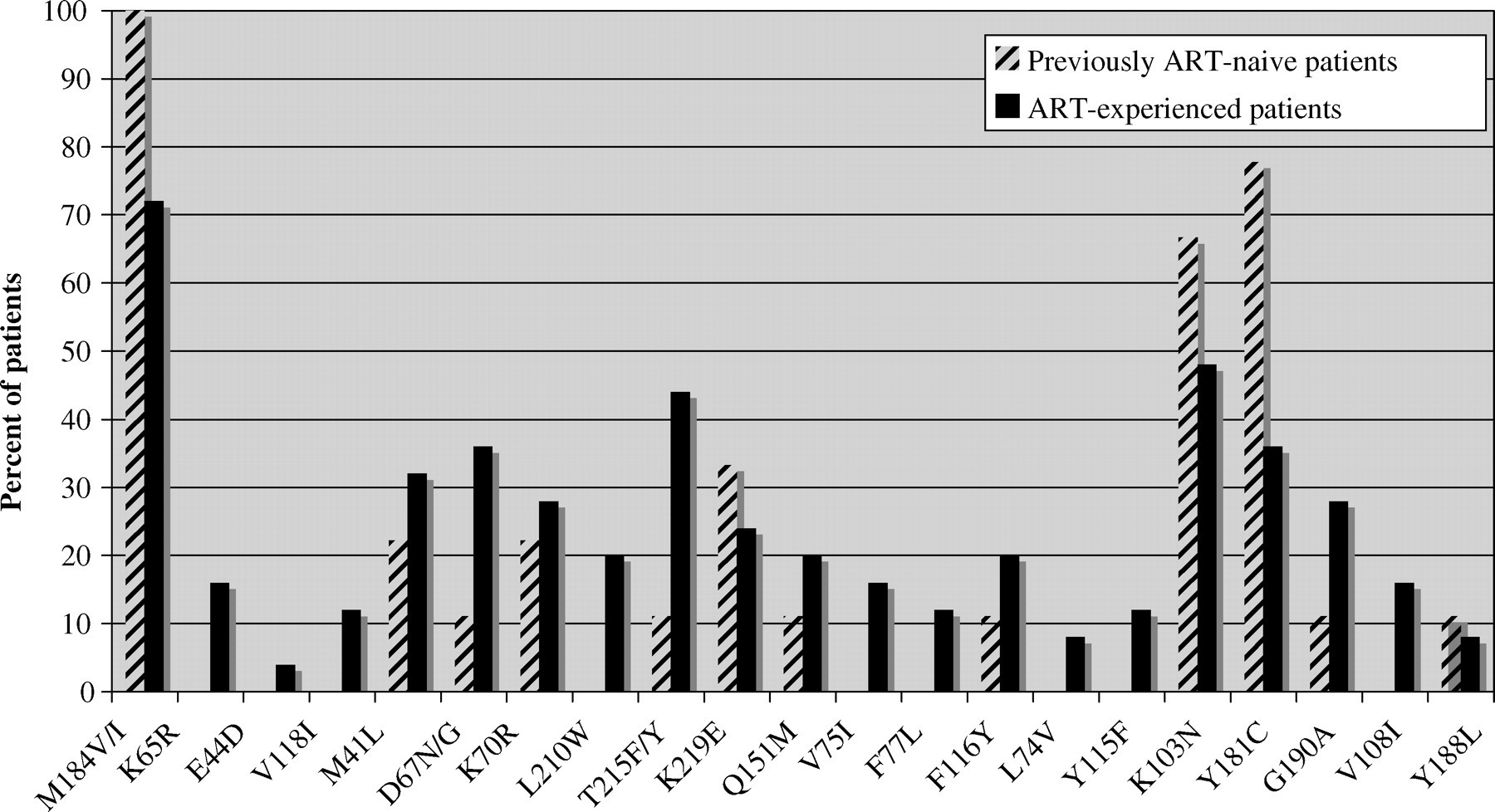
Patients with the most common NRTI and NNRTI mutations. NRTI = nucleoside reverse transcriptase inhibitor; NNRTI = non-nucleoside reverse transcriptase inhibitor
Drug resistance is shown in Figure 2. Resistance to AZT, D4T and TDF were each more common in ART-experienced patients compared with previously ART-naïve patients (68.0% versus 22.2%, P = 0.03; 64.0% versus 22.2%, P = 0.05; 44.0% versus 0.0%, P = 0.02; respectively).
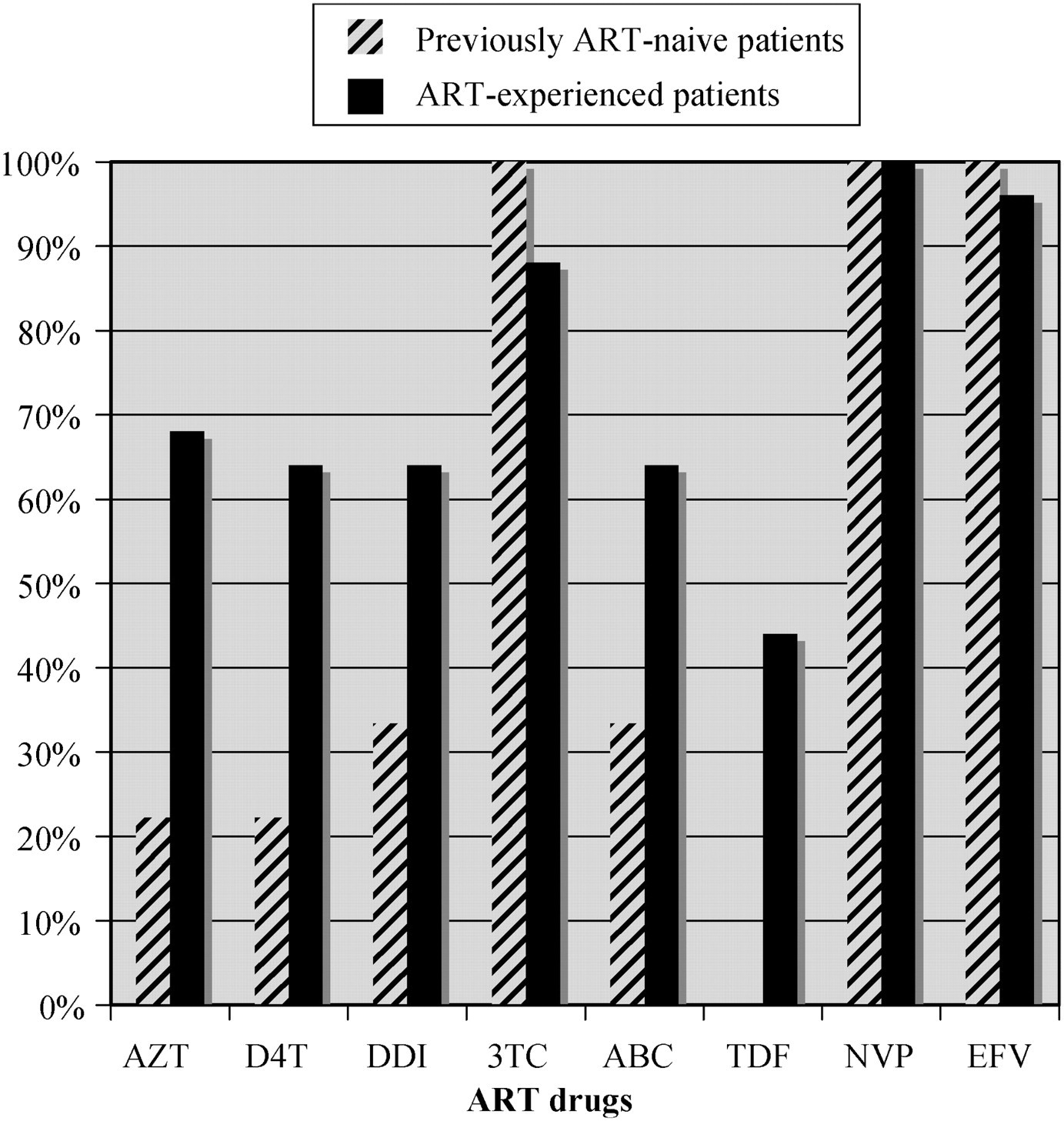
Patients with high or intermediate drug resistance
The following cohort characteristics were analysed to determine predictors of developing resistance: age, gender, transmission mode (mother to child versus blood transfusion/other), ART experience, and low CD4 count (<100 cells/μL versus >100 cells/μL) and viral load (1 log) at one year. In univariate analysis, significance was found for ART experience (odds ratio [OR] 12.3: 4.3–35.4, P < 0.0001), viral load (OR 13.3: 4.5–38.7, P < 0.0001) and low CD4 count (OR 11.7: 1.4–99.2; P = 0.02). In a multivariate analysis of all the above-noted characteristics, only viral load remained significant (OR 26.5: 3.6–96.1, P = 0.001).
DISCUSSION
The prevalence of drug resistance is high in the Chinese National Pediatric HAART cohort, with at least 62.5% of ART-experienced and 27.5% of previously ART-naïve children showing resistance to one or more drugs after one year of HAART. Because seven samples with detectable viral load could not be sequenced, drug resistance is likely even more prevalent. This finding is consistent with the expectation of increasing drug resistance with increasing time on therapy; however, the overall high prevalence after only one year of treatment is of concern.
Some degree of drug resistance was expected for several reasons. First, the ART-experienced children likely had inaccurate dosing through use of adult formulations and inadequate clinician training prior to the initiation of the National Pediatric HAART Programme. Clinicians involved in paediatric HIV/AIDS care must be aware of the specific needs of children, such as frequent dose modifications by weight and adherence challenges. Additional potential causes of drug resistance include variable pharmacokinetics and drug interactions with traditional medicines, which are common in China. Although baseline resistance could contribute to the findings of this study, prior research has shown that the probability is very low. 6 ART was extremely limited in China before 2003, all children in this cohort were infected prior to that time, and none of the children or their mothers received ART for prevention of mother to child transmission.
Adherence is particularly complex for children and can be greatly affected by caregiver characteristics, disclosure of HIV status, age and disease severity. 7 Additionally, the setting was very rural and poor with few resources for medical and social support. Although this study did not objectively measure adherence, caregivers typically reported excellent adherence, likely indicating social desirability bias. Further research is needed to determine optimal adherence support for children in such settings.
The finding of increased TAMs and resistance to AZT and D4T in ART-experienced patients compared with previously ART-naïve patients is consistent with the known accumulation of these mutations and corresponding NRTI resistance over time. 8 Early identification of resistance is therefore critical in preserving the efficacy of these NRTIs. The TDF resistance in ART-experienced patients likely reflects cross-resistance with DDI, as none of the patients had taken TDF.
The high levels of mutations and corresponding drug resistance (particularly M184V reflecting resistance to 3TC/FTC; K103 N and Y181C reflecting resistance to NVP and EFV) in previously ART-naïve children indicate how readily the efficacy of these drugs is lost. These findings are consistent with other paediatric studies and a national analysis of Chinese patients. 3,4,9 The World Health Organization (WHO) and others recommend three-drug regimens including a thymidine analog plus (3TC or FTC) plus (EFV or NVP) in resource-constrained settings, based on efficacy, relative ease of administration and access to low-cost, generic formulations. 10,11 The sustainability of these regimens and the implications of resistance, however, need further study. The WHO is supporting global ART resistance surveillance, 12 including monitoring entry sequences, which will provide guidance for future treatment efforts.
The frequency and breadth of drug resistance from this pilot study strongly suggest the need for potent second-line HAART to sustain clinical benefit. Regimens based on ritonavir-boosted protease inhibitors (rPI) are an excellent option, appear to be safe and effective, and have a high barrier to resistance. 11,13–15 The use of rPI, however, is limited by cost, drug availability, storage temperature requirements and palatability (i.e. liquid lopinavir/ritonavir). While additional resources, such as UNITAID and some pharmaceutical access programmes, are available, many national programmes in the developing world do not have sufficient resources to pay for large second-line therapy programmes. An alternative approach to be considered is the accruing data from the Developing Antiretroviral Therapy in Africa (DART) study in Africa and its paediatric parallel ‘Baby DART’. 16 Use of a triple nucleoside/nucleotide regimen as a first-line therapy may allow for an effective second-line regimen consisting of an NNRTI with new and recycled nucleoside drugs and may defer the need for more expensive rPI.
An additional challenge for the developing world is the ability to perform resistance testing, which is expensive and technically difficult. The variable degree of NRTI resistance and significant cross-resistance to drugs not previously administered in some patients in this study indicates that resistance testing may be needed for individual patients, although many of the mutations are predictable by the drug regimens employed. An algorithmic approach is more practical, and surveillance for resistance, rather than individualized testing, will drive public health treatment decisions in practice. Centralized testing and use of dried blood spot technology may also help maximize resources.
Treatment of paediatric HIV/AIDS in the developing world presents many challenges, but the experience in China and elsewhere indicates that many children respond clinically quite well, albeit for a limited time. Aggressive efforts to optimize access and adherence are the best immediate tools to defer large commitments to more expensive second-line regimens. The drug resistance data from this small cohort suggest that alternative first- and second-line treatment strategies must be explored to identify affordable drug regimens.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the clinical and public health staff in Shangcai County, Henan, the staff at the Shangcai County CDC and Beijing Ditan Hospital laboratories, and Drs. David Katzenstein and Nancy Shulman at Stanford University. This study was funded by the Chinese Ministry of Science and Technology Grant (2004BA719A11), Chinese National Basic Research Program (973:2006CB504201) and United States National Institutes of Health (U2RTW006918). Alex Chu and Nancy Wang were supported partly by Stanford University.