
Abstract
The aim of this study was to compare HIV-1 prevalence between pregnant, non-pregnant, all women and the general population (men and women) and investigate how well risk behaviours of pregnant women reflect those of all women in the general population in rural Kilimanjaro, Tanzania. A cross-sectional survey involving all individuals aged 15–44 years was conducted in Oria village between March and May of 2005. All consenting individuals were interviewed and offered HIV-1 and syphilis testing. The response proportion among women was found to be 73.7% (914/1241). Age-adjusted HIV-1 prevalence among pregnant women (n = 92) was 32.5% lower (5.4% versus 8.0%, P, 0.001) than that of all women but only 8.5% (5.4% versus 5.9%, P = 0.639) lower compared with that of the general population. HIV-1 risk factors among pregnant women were comparable to that of all women in the general population. In conclusion, pregnant women in the general population underestimate the HIV-1 magnitude among women but closely approximate that of the general population. HIV-1 risk factors are similar between pregnant and all women in the general population. Second-generation surveillance could utilize pregnant women risk behaviours to approximate that of all women in the general population.
Introduction
Antenatal clinic (ANC) sentinel seroprevalence surveys are the major empirically based source of HIV-1 prevalence data. Although popular, ANC data are subject to biases. ANC attendance is more likely to vary by age, marital status, locality, socioeconomic status and education level; factors associated with HIV-1 serostatus.1,2 Only sexually active non-contraceptive users attend ANC and HIV-1 tends to reduce fertility for biological and social reasons. The effect of reduced fertility among HIV-positive women has been well studied.3–9 Overall, HIV-1 prevalence from ANC data have been reported to be 10–30% lower than that of women in the general population especially for those over 20 years.1,10 In the efforts to validate the use of ANC data as a sentinel population in HIV-1 population estimation, comparison of ANC and general population HIV-1 prevalence has been tried.11–14 Some studies have even employed a mathematical model in order to adjust ANC data for the purpose of extrapolating general female population estimates.3,15–18
Differential attendance to ANC has been held as one of the cause of biased estimates in HIV-1 prevalence. Direct comparison of HIV-1 magnitude between pregnant, non-pregnant and all women (overall) from the general population may help in avoiding the effect of selection bias among ANC attendees. This may shed light on the magnitude of selection bias and whether the ANC estimates reflect the reality in the general population. Moreover, the World Health Organization (WHO) is recommending the use of ‘second-generation’ surveillance where inclusion of risk behaviours in routine ANC surveillance is advocated.19–21 Only one study has tried to explore the usefulness of behavioural data from ANC in general population behavioural monitoring. 22 However, it is not known how well risky sexual behaviours estimates from pregnant women in the general population approximate those of non-pregnant women and those of all women of reproductive age.
In this study, we had a unique opportunity to examine the above-mentioned issues by comparing HIV-1 prevalence and risky sexual behaviours between pregnant, non-pregnant, all women (pregnant and non-pregnant) and the general population (men and women) from a total village population survey in rural Kilimanjaro, Tanzania.
Methods
Study area
The study was conducted in Oria village in Kahe ward, Kilimanjaro, Tanzania. Details of this study area have been described elsewhere.23,24 In brief, Oria is a rural village at the foot of Mount Kilimanjaro about 30 km from Moshi town in the Kilimanjaro region. The majority of the people engage in small-scale rice and maize farming and some keep goats and/or cattle. The village has one private and one public dispensary.
Study design and population
This was a population-based cross-sectional study conducted between March and May of 2005. All individuals aged between 15 and 44 years (n = 2093; women = 1241, men = 852) and listed as having an address in the village were eligible for participation.
Data collection procedures
The research team completed a house-to-house registration of all eligible individuals. Eligibility was based on being at the given age range and having an address in the village. The village had nine hamlets (small administrative units) and data collection was done from hamlet to hamlet. Appointments for data collection were set by the research team and the hamlets leaders. At the set dates, the research team went from house to house. Participants received information regarding the study aims and procedures, and those who agreed to participate provided a written informed consent. A structured questionnaire was administered in a private place to ensure confidentiality. During the interviews, information on the socio demographic factors (age, sex, education, current occupation and marital status), HIV-1 risk factors (number of sexual partners in the past four weeks and 12 months, exchange of money/goods for sex, past month treatment for genital ulcer disease, genital discharge and past five years history of treatment for sexually transmitted infection) was collected. Data on pregnancy status were also collected. These included current pregnancy status, parity and time since last delivery. The interviews were followed by pretest counselling and subsequent blood collection for HIV-1 and syphilis testing. Appointments were made with each participant for post-test counselling within two weeks from the date of sample collection. Efforts were made to provide results to all who wanted to know their status as this would serve as an entry point for care and prevention. Individuals who indicated that they did not want to know their test results were also re-visited and re-counselled. All missed participants during recruitment were visited three times at home or at their nearby work place before being considered as non-respondents.
Ethical issues
Ethical approval for the study was provided by the Ethical Committee of the Ministry of Health in Tanzania and the Norwegian Committee for Medical Research Ethics in Norway. The village government of Oria granted permission for the study. All participants gave written informed consent for the interview and blood sampling separately. HIV-1 test results were issued to respondents in person after pretest and post-test counselling. Further medical follow-up was offered for all HIV-1-positive respondents. All residents of the village had access to free treatment for common medical conditions from a research mobile clinic throughout the survey duration.
Laboratory methods
Two independent enzyme-linked immunoassay (ELISA) systems (Voronostica Uniform II plus O; Organon, Boxtel, the Netherlands and Enzygnost Anti HIV 1/2 Plus; Dade Behring, South Africa) were used in the detection of HIV-1 antibodies. In case of discordant or weakly concordant ELISA results, Western blot (Bio-Rad Laboratories Ltd, Dartford, UK) was used for confirmation. Past infection with syphilis was tested using rapid plasma reagin test (Immutrep RPR, Omega Diagnostics, Scotland, UK). All specimens were tested at the clinical laboratory of the Kilimanjaro Christian Medical Centre, Moshi, Tanzania.
Statistical analysis
Frequencies and cross tabulation of various demographic characteristics was done for descriptive purposes. The χ2 test for differences in proportions was applied for categorical variables; continuous normally distributed variables were presented as means with their respective standard deviations (SDs). To test for differences between means, Student's t-test and analysis of variance (ANOVA) were employed. Age-specific HIV-1 prevalences were calculated using the district (Moshi rural) population as standard population. Strength of association between HIV-1 infection and various pregnancy statuses was estimated by calculating the odds ratios with 95% confidence intervals (CIs). Multivariable logistic regression with HIV-1 seropositivity as a dependent variable was used to control for potential confounders (age, marital status and parity). Adjusted odds ratios (AOR) with 95% CI were then presented. The Statistical Package for Social Sciences (SPSS) for windows version 15.0 (SPSS Inc., Chicago, IL, USA) was used for the data analysis.
Results
A total of 1528 individuals (men and women) participated in the study. The overall response proportion was 73.0% (1528/2093). Of all participants, 914 (59.8%) were women (response proportion 73.7%) and 614 were men (response proportion 72.1%). The mean age did not differ significantly between women and men (mean age 27.9 [SD ±8.6] years for women versus 28.7 [SD±8.8] for men, P = 0.056). The overall age-adjusted HIV-1 prevalence in the village was 5.9% (8.0% for women and 3.2% for men). During the time of the survey, 92 (11.2%) of the women were pregnant and 822 were not pregnant. A total of 708 (77.5%) reported to have ever been pregnant and the majority of them, 433 (61.2%), reported to have delivered in the past five years preceding the survey. Half of those who have ever been pregnant 354 (50.0%), had had 2–4 pregnancies.
Comparison of background characteristics between pregnant, non-pregnant and all women in the general population in a rural village, Kilimanjaro, Tanzania
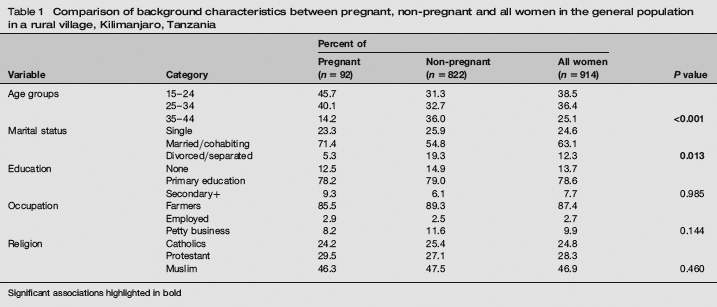
Significant associations highlighted in bold
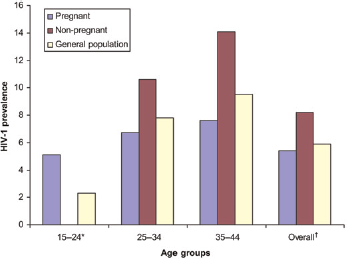
Figure 1 compares HIV-1 prevalence between pregnant, non-pregnant women and all women in the general population by age groups, while Figure 2 compares the HIV-1 prevalence between pregnant women, non-pregnant women and the general population by age groups. Under the age of 24 years, pregnant women had significantly higher HIV-1 prevalence as compared with non-pregnant women, all women and the general population (Figures 1 and 2). Above the age of 24 years, pregnant women had a significantly lower HIV-1 prevalence as compared with non-pregnant women, all women and the whole general population. This difference was much larger when pregnant women were compared with all women than when compared with the general population (Figures 1 and 2). The overall age-adjusted HIV-1 prevalence among pregnant women was 32.5% lower than that of all women in the general population (5.4% versus 8.0%, P < 0.001). However, this prevalence was only 8.5% (5.4% versus 5.9%, P = 0.639) lower when compared with that of the whole general population.
Comparison of HIV-1 prevalence between pregnant, non-pregnant women and all women in the general population in rural Kilimanjaro, Tanzania. *No HIV-1 seroconversion among the non-pregnant women in this age group, †Age-adjusted HIV-1 prevalence Comparison of HIV-1 prevalence between pregnant, non-pregnant women and the general population by age groups in rural Kilimanjaro, Tanzania. *No HIV-1 seroconversion among the non-pregnant women in this age group, †Age-adjusted HIV-1 prevalence. General population include both men and women
Multivariable analysis of pregnancy status and HIV-1 infection among women in a rural village Kilimanjaro, Tanzania
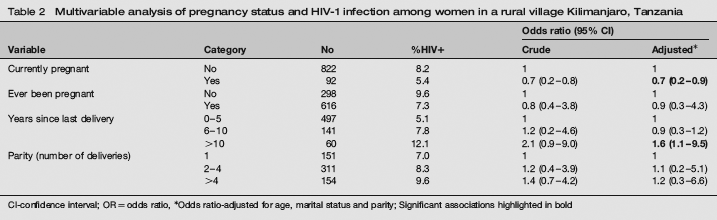
CI-confidence interval; OR = odds ratio,
Odds ratio-adjusted for age, marital status and parity; Significant associations highlighted in bold
Comparison of HIV-1 risk factors between pregnant, non-pregnant and all women in the general population in a rural village Kilimanjaro, Tanzania
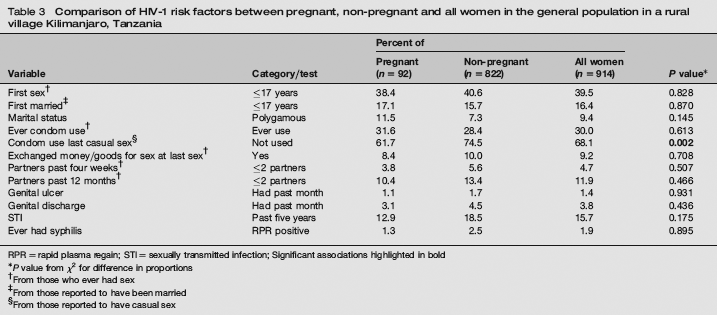
RPR = rapid plasma regain; STI = sexually transmitted infection; Significant associations highlighted in bold
P value from χ2 for difference in proportions
From those who ever had sex
From those reported to have been married
From those reported to have casual sex
Discussion
The results from this study showed that pregnant women in the general population were significantly younger and more frequently married/cohabited compared with non-pregnant women. HIV-1 prevalence was significantly lower (32.5% lower) among pregnant women as compared with non-pregnant women in this rural population but closely similar to that of the general population (men and women combined). Young (<24 years) pregnant women overestimated HIV-1 prevalence among both all women and the whole general population while older women (>24 years) underestimated the same estimates. Pregnant, non-pregnant women and all women had similar age at sexual debut and age at marriage. Reported risk behaviours among pregnant women were comparable to that of all women in the general population. Increased duration since last delivery was significant associated with HIV-1 infection.
This study shows that although HIV-1 testing among pregnant women tends to significantly underestimate the actual HIV-1 magnitude in the female population, they approximate closely the overall general population estimates (women and men combined). This observation could be explained by the fact that women in Africa have disproportionally high HIV-1 prevalence compared with men (8.0% versus 3.2% in this population) 24 and involving men estimates adjust downward the overall general population estimates close to that of pregnant women. Similar findings have been recently published from Zambia using women attending ANC. 25 This study therefore underpins these findings using pregnant women from the general population by comparing them with non-pregnant, all female population (pregnant and non-pregnant) and the whole village population (men and women). Therefore, in areas where ANC utilization is high, ANC HIV-1 estimates reflect the reality in the general population and selection bias might have very little effect. The importance of these findings is the usefulness of pregnant women in directly extrapolating general population HIV-1 estimates.
Differences in HIV-1 risk factors between pregnant, non-pregnant women and overall women in the general population have yet to be described. A study in Mwanza Tanzania tried to examine the usefulness of ANC collected behavioural data in reflecting the general population behavioural data. 22 However, this study involved a selected sample of pregnant women attending ANC and did not involve non-pregnant women. This study had a unique opportunity to compare unbiased sample (from the general population versus ANC sample) of pregnant, non-pregnant women and all women (overall) in terms of various HIV-1 risk factors. It was shown in this study that although pregnant women were younger than non-pregnant women, these two groups had similar age at sexual debut and marriage. Moreover, pregnant women's reported risk behaviours were comparable to that of all women of reproductive age in the general population. This indicate that in places where ANC utilization is high in such a way that women attending ANC represent women of reproductive age in the general population, estimation of HIV-1 risk factors among them could be held to approximate that of all women in the general population. These findings support the WHO ‘second-generation’ surveillance recommendation by showing that collection of various HIV risk factors from ANC attendee may not only explain their HIV estimates but also risk factors of all women in the general population.19–21 The increased HIV-1 infection with time since last delivery has been observed in many studies.4,6–8 The impact of HIV on fertility and social explanation like widowhood among HIV-positive women has been held to explain this observation. This is supported by the finding in this population where HIV-1 prevalence was high among women who reported to be widowed/separated. 24
Findings in this study have the following implications: firstly, estimated HIV-1 risk behaviours among pregnant women could be used as a proxy measure of risk among all women of reproductive age in the general population. This may be crucial in the implementation of the WHO ‘second-generation’ surveillance. Secondly, HIV-1 estimates from pregnant women could continue to be used as a proxy measure of the general populations estimates and lastly, ANC estimates reflect the actual estimates of respective group (pregnant women) in the general population where ANC utilization is high and selection bias may not have a significant effect.
In this study, a response proportion of 73.7% was achieved among women. As a response proportion above 70.0% have been recommended for population surveys, 26 it may be stated that a representative sample of women were included giving the results good external validity. The approach of involving the whole village population in this study may also help to eliminate potential sampling biases. Differential non-response among men may affect general population estimates. In this study, no significant difference in participation was observed between men and women. Comparison of sociodemographic characteristics between participants and non-participants did not show any significant difference indicating that participants were a representative sample of the village population. 24 Estimation of reported risky sexual behaviours is always associated with biases that could be due to desirability reporting or the fact that the behaviours of partners are not known.19,27,28 Moreover, women tend to under-report their HIV risk behaviours in Africa as part of cultural femininity ideologies. 27 But these biases may have affected both pregnant and non-pregnant women non-differentially hence introducing less effect on the findings presented.
Conclusions
Pregnant women from the general population significantly underestimate HIV-1 estimates of all women of reproductive age but closely approximate that of the general population (women and men). Reported HIV-1 risk factors among pregnant women are comparable to those of all women of reproductive age in the general population. Long period since last delivery is associated with HIV-1 infection probably due to infertility and widowhood among HIV-1-infected women. A representative sample of pregnant women attending ANC could be used to estimate general population HIV prevalence. Risky sexual behaviours among these women could also be used to explain HIV estimates of all women of reproductive age in the general population as recommended in the ‘second-generation surveillance’.
Footnotes
Acknowledgements
The authors are grateful to the participants for their time. This work was facilitated by the collaborating institutions: Muhimbili University of Health Sciences, Kilimanjaro Christian Medical College, Centre for Education in Health Development Arusha in Tanzania, and the Universities of Oslo and Bergen, Norway.