
Abstract
We describe the case of a 37-year-old African woman with an asymptomatic lesion on her right conjunctiva; histology of the lesion revealed the presence of conjunctival intraepithelial neoplasia. HIV-positive patients from Africa are at increased risk of developing conjunctival malignancies, and early diagnosis and treatment can prevent serious consequences.
Keywords
INTRODUCTION
Over the last 10 years, a number of reports have indicated an association between ocular surface squamous neoplasia (OSSN) and HIV infection in sub-Saharan African populations. 1 OSSN includes conjunctival intraepithelial neoplasia (CIN) and invasive squamous cell carcinoma (SCC). CIN is sub-divided into grades 1–3. In mild dysplasia (CIN1) neoplastic changes involve partial thickness of the conjunctival epithelium, and in CIN3 full thickness of the epithelium is affected. 2 We report a case of CIN in an HIV-positive African woman.
CASE REPORT
A 37-year-old HIV positive woman from Congo attended our clinic after her recent arrival in the UK. She was diagnosed with HIV infection two months previously at a refugee camp in Zambia. She had probably acquired HIV infection through a heterosexual route. She had no symptoms and was not on any treatment. Her CD4 count was 139 cells/mm3 and the HIV load was 59,540 copies of RNA/mL of blood.
On examination she was noted to have a 5-mm-diameter white plaque on the right conjunctiva (Figure 1). To a direct question, the patient informed us that this eye lesion had been present for more than six months and was entirely asymptomatic, and she had not noticed any loss of vision. Systemic examination was normal apart from genital warts; cervical cytology showed mild dyskaryosis and high-risk human papilloma virus (HPV) was detected.
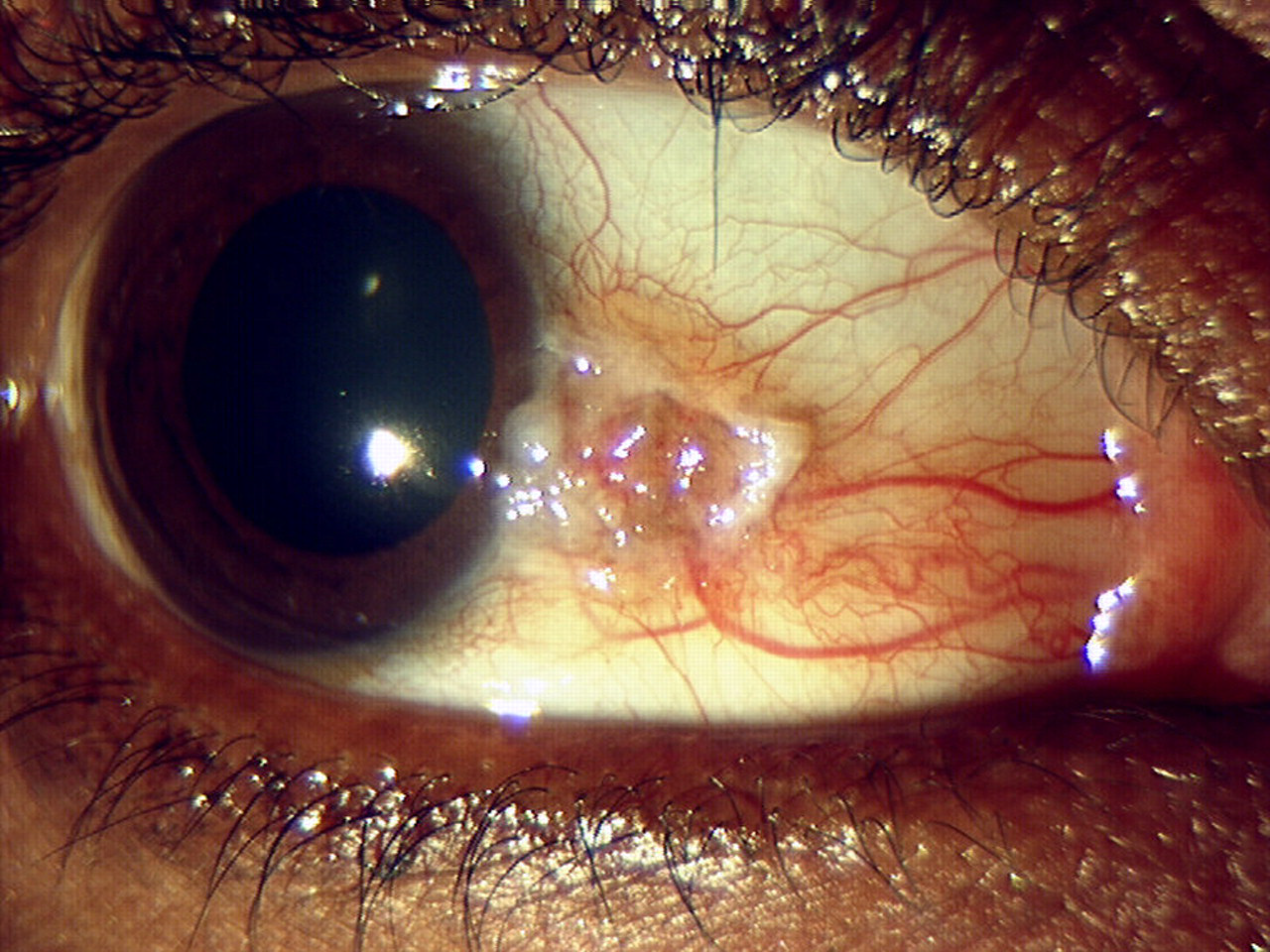
Lesion on the right conjunctiva
The patient was started on highly active antiretroviral therapy (abacavir, lamivudine and nevirapine) and was reviewed by the ophthalmology team. She had no visual symptoms and her vision was good at 6/9 in both eyes. She was found to have an irregular conjunctival raised lesion at her right nasal limbus extending onto her nasal cornea. This was associated with some engorged vessels leading to it and also with some whitish plaque-like areas suggestive of leucoplakia. The rest of her eye examination was unremarkable. In view of the patient's positive HIV status, the clinical appearances of the lesion and the fact that she had had no previous ocular surgery, a presumptive diagnosis of CIN was made, but the differential diagnosis included Bowen's disease. The lesion was excised and sent for histological examination.
Histopathology of the lesion showed conjunctival tissue with central epithelial thickening, moderate keratinocyte dysplasia and scattered suprabasal mitoses. Underlying stroma showed a moderate infiltrate of chronic inflammatory cells. The overall findings were suggestive of CIN stage 2–3. The lesion extended to the deep surgical margin but was clear of the peripheral margins. There was no evidence of invasive malignancy or metastases.
The patient was reviewed after surgery and was started on mitomycin drops 0.02% three times a day for one week, because of incomplete excision. A month later she had two very small elevated areas of conjunctiva at the site of surgery and was started on another cycle of mitomycin 0.04% four times a day for a week, which resulted in resolution of the clinical signs. She remains under periodic review to check for possible recurrence, and may need a third cycle of mitomycin drops topically.
DISCUSSION
The epidemiology of OSSN is changing. 2 It used to be an uncommon slow-growing tumour found in elderly men, but recent reports suggest that in Africa it is becoming more common, more aggressive and more likely to affect younger people, especially women. 2 This pattern is related to the coexistence of HIV infection, high HPV carriage and high levels of solar radiation in the region. 2,3 HIV infection leads to an approximately 10-fold increase in the risk of conjunctival neoplasia. 4 In one series of African patients, 79% of patients with OSSN were HIV positive and OSSN was the only detectable manifestation of an HIV-related condition in 70% of these patients. 1
Patients may be asymptomatic or suffer from a red eye, ocular irritation, severe pain and visual loss. 2,3 OSSN commonly affects the visible area between the upper and lower eyelids (palpebral conjunctiva), usually on the nasal side at the margin of the conjunctiva and the cornea (limbus). 2 The growth may be nodular, gelatinous, flat superficial leukoplakic or diffusely invasive. It may mimic benign conjunctival degenerations and sometimes co-exist with pinguecula and pterygium. 5 It is important to recognize CIN because it causes disfigurement and can progress to SCC, which has the potential to cause severe disability. 3 SCC may extend into the eyeball, orbit, regional lymph nodes, surrounding paranasal sinuses and the brain. Death may result from regional or distant metastases, as well as intracranial spread. 2
Current treatments for CIN include complete tumour excision, with or without reconstruction of the surface defect by amniotic membrane transplantation or limbal autografts. Adjunctive therapies include cryotherapy, topical antimetabolites such as mitomycin and 5-fluorouracil, radiotherapy, immune therapy (e.g. Interferon alpha) and cidofovir antiviral therapy. 2 Advanced disease where the tumour has spread requires removal of the eyeball (modified enucleation) or the entire orbital contents (exenteration) in an attempt to save life. 2 The recurrence rate may be higher in Africa due to late presentation, lack of many of the adjunctive therapies and immunosupression. Cryotherapy and chemotherapy are only likely to be found in specialist centres. 2
With increasing numbers of HIV-positive African patients being treated in the UK, awareness of OSSN is important in both asymptomatic and symptomatic patients. A combination of immunosupression due to HIV, solar exposure and HPV infection may have contributed to the development of CIN in our patient. Early diagnosis and treatment may prevent the development of invasive SCC, which could be sight- and life-threatening. We suggest that every patient with OSSN should be assessed for risk factors and encouraged to undergo HIV testing.