
Abstract
We report a 31-year-old man with an obstructive bronchial lesion due to herpes simplex type 2 infection, who responded promptly to endoscopic resection and oral treatment with acyclovir. Exophytic lesions of the respiratory tract are rare, potentially life-threatening, but readily treated complication of herpes simplex virus infection in HIV-infected individuals.
INTRODUCTION
Severe mucocutaneous disease due to herpes simplex virus (HSV) infection of the orolabial, genital or perianal regions is a well recognized opportunistic infection in patients with HIV infection. The pathogenesis of these infections may be influenced by complex interactions between the HIV, HSV and the human immune system. 1,2 We report a potentially life-threatening complication of HSV–HIV co-infection to draw attention to the unusual manifestations of HSV infection of the respiratory mucosa in HIV-infected patients.
CASE REPORT
A 31-year-old European man presented with a three-week history of a productive cough and increasing dyspnoea on exertion. HIV infection had been diagnosed six years previously when he presented with Pneumocystis jirovecii pneumonia (PJP). His antiretroviral treatment regimen was lamivudine/zidovudine 150 mg/300 mg and lopinavir/ritonavir 200 mg /50 mg twice daily, plus cotrimoxazole 480 mg once daily as PJP prophylaxis. One month prior to presentation, his absolute CD4+ T lymphocyte count was 158 cells/μL and his HIV viral load was <40 copies/mL.
He was afebrile on admission but had temperatures up to 37.9°C during his admission. His pulse rate was 70 beats per minute and respiratory rate was 18 breaths per minute. His chest was resonant to percussion, but he had decreased breath sounds in the right lower zone. His transcutaneous oxygen saturation was 96% at rest while breathing room air, but fell to 88% after walking up two flights of stairs. During his 12-day hospital admission, his oxygen saturation while breathing room air ranged between 85% and 99% but was frequently between 90% and 95%.
Routine investigations failed to find a cause for his symptoms. His chest X-ray showed peri-bronchial thickening in the right lower lobe with a small patch of air space consolidation in the right upper lobe. A high-resolution computed tomography scan showed a soft tissue mass obstructing the right main stem bronchus and extending into the region of the carina plus 1.5 cm diameter subcarinal lymph nodes. Subtle ground glass attenuation was present in both lungs. These radiology findings were thought to be suspicious for malignancy or lymphoma (Figure 1a).
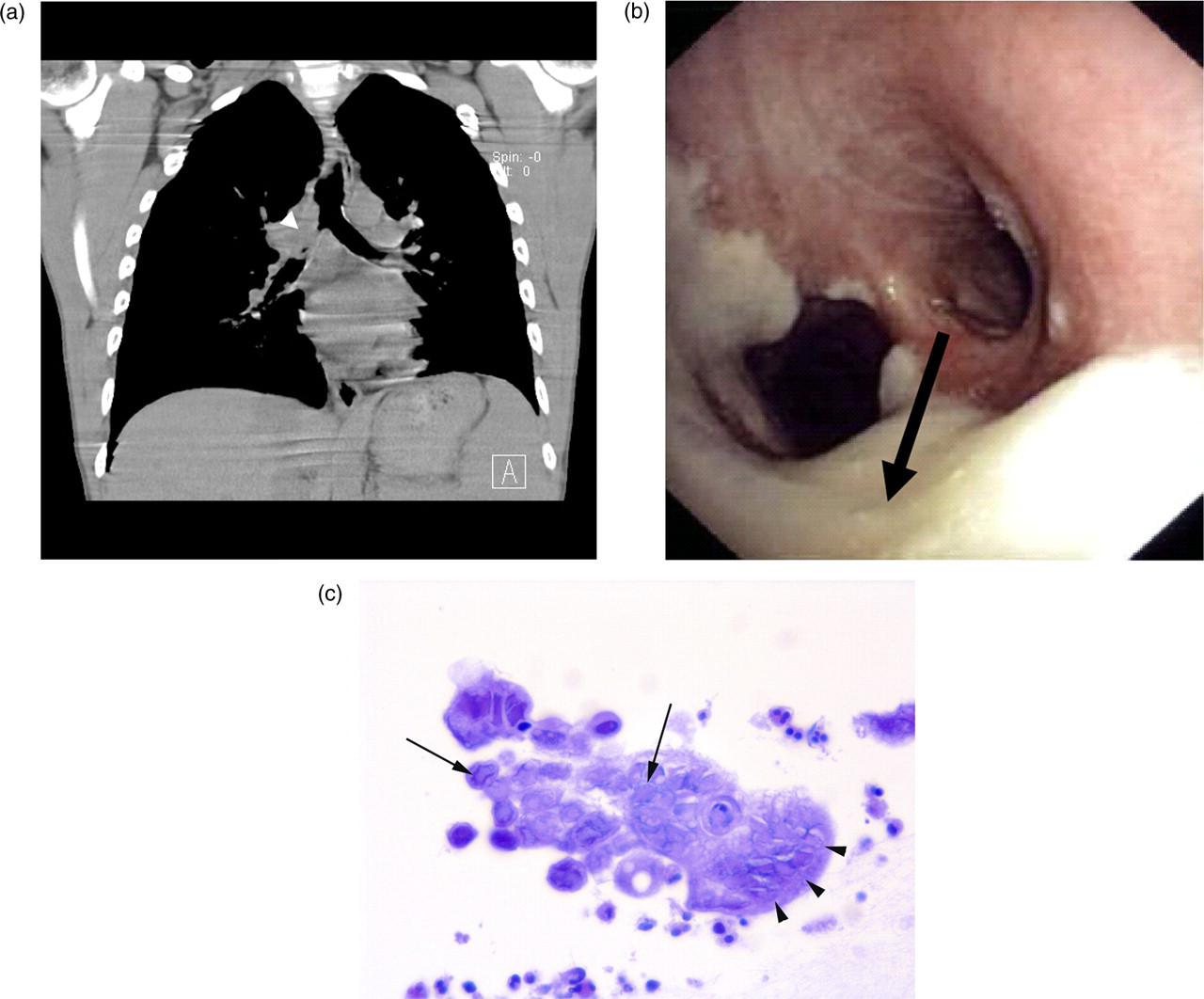
Radiological, endoscopic and histological findings in endobronchial Herpes simplex disease. (a) Computed tomography coronal reconstruction image showing an obstructing lesion in the right main bronchus (arrowhead). (b) Endoscopic appearance of lesion in the right main bronchus (arrow). (c) Histological appearance of endobronchial pseudotumour showing epithelial cells with Cowdry type A nuclear inclusions (arrows), and syncytium (giant cell) formation (arrowheads) visualized with haematoxylin and eosin staining at original magnification ×100 with oil immersion
He underwent a fibreoptic bronchoscopy, which showed diffuse white plaque-like material in the lower trachea and the upper right main bronchus (Figure 1b). During the procedure, he spontaneously coughed up a white plaque and then further white plaque-like material was removed from the right main bronchus. He was discharged from the hospital while awaiting the laboratory results of the bronchoscopy samples. When seen in clinic a week later he reported that while living in Sydney, one year previously, he had had white plaques in his mouth, of similar appearance to the material removed during the bronchoscopy and that these had been treated successfully with oral acyclovir.
The tissue obtained at bronchoscopy consisted of laminated mucin with fibrin, eosinophils and exfoliated epithelial cells with ground glass intranuclear inclusions and multi-nucleation typical of HSV infection (Figure 1c). Immunohistochemistry for HSV was positive and HSV type 2 was cultured from the bronchial washings. He was given a two-week course of oral acyclovir 800 mg five times a day and when seen at the clinic three months later he reported that his symptoms of dyspnoea and productive cough had resolved. He has remained well during the subsequent 18 months.
DISCUSSION
We are aware of five other case reports of exophytic pseudotumours of the respiratory tract due to HSV infection. 3–7 The macroscopic appearance of these pseudotumours was similar to the appearance of the pseudotumour in our patient. The lesions were commonly described as shiny, white, exophytic or plaque-like tumours. HSV infection was demonstrated by immunohistochemical staining of excised tissue in four cases 3,4,6,7 and by culture 7 and polymerase chain reaction (PCR) testing 5 in two cases. Two of the five patients had severe HIV-infection-related immunosuppression (absolute CD4+ lymphocyte count <50 cells/μL) and one patient had HIV infection without significant immunosuppression (absolute CD4+ lymphocyte count = 382 cells/μL). No statement was made about whether the other two patients had been tested for HIV infection. One, a 59-year-old man, had recently suffered a cerebrovascular accident, 6 while the other, a 68-year-old woman, had a history of multiple congenital abnormalities. 7 Neither of these two patients were reported to have any immunosuppressive conditions or treatment.
In all reported cases, the duration of symptoms was less than one month, suggesting that the lesions had enlarged relatively rapidly. In our case and three of the five reported cases, the pseudotumour caused significant obstruction of the respiratory tract: partial obstruction of the right main bronchus in our patient, complete obstruction of the right upper lobe bronchus in one patient, 4 partial obstruction of the right middle lobe bronchus in another patient, 7 and almost complete occlusion of the larynx during inspiration in the third. 6 In our case and four of the reported cases, resection of the pseudotumour plus antiviral therapy resulted in prompt complete cure. 3–6 In one patient active treatment was withdrawn and death ensued. 7
Clinicians caring for patients with HIV infection should be aware that HSV co-infection may be responsible for exophytic lesions of the respiratory tract, which may rapidly progress to cause significant airway obstruction. Diagnosis is readily made by immunohistochemical staining or by culture or PCR. Combined medical and surgical treatment is promptly effective.