
Abstract
Summary
The re-emergence of syphilis among HIV-infected patients has been reported in recent years. We evaluated co-infection among heterosexual immigrants in an Israeli AIDS center. The records of 1060 HIV-infected patients were evaluated for positive syphilis serology between the years 2000 and 2005, and all seropositive patients were further evaluated. We found 150 HIV/syphilis co-infected patients (57% men, 93% of African origin), of who 135 were found to have late latent syphilis. Lumbar puncture (LP) was performed in 51 patients, 16 (31 %) had abnormal cerebrospinal fluid (CSF) compatible with neurosyphilis. Abnormal CSF correlated with the absence of previous anti-syphilis treatment, but not with CD4 count, viral load or Venereal Disease Research Laboratory titres. Penicillin was recommended to all patients according to their disease stages and 81 patients completed 12 months post-treatment follow-up. Twenty-one of 81 (26%) treatments were successful, 33 (41 %) showed ‘serofast reaction’ and 27 (33%) failed therapy. In conclusion, a high incidence of syphilis with CSF reactivity suggestive of neurosyphilis was observed in heterosexual Ethiopian HIV-infected patients. Thus, repeated serological screening and CSF evaluation seems to be indicated in these patients. Penicillin therapy resulted in ‘serofast reaction’ or treatment failure for most patients. More, intensive treatment might be needed for HIV/syphilis in co-infected patients, especially those with severe immune-deficiency and prolonged syphilis infection.
Introduction
The sexually transmitted infections, syphilis, caused by the spirochete Treponema pallidum, and HIV/AIDS, caused by the human immunodeficiency virus (HIV), affect similar groups of patients. 1 Co-infection of syphilis and HIV alters the course of both diseases. 1 HIV infection might also change the clinical presentation of syphilis (e.g. high rate of undiagnosed primary syphilis). Central nervous system (CNS) invasion by the spirochete is an early event in the course of syphilis that usually clears spontaneously. Persistent CNS infection increases the risk for development of neurosyphilis, 2 4 and co-infection has been reported to increase CNS involvement. 5 8 On the other hand, syphilis (especially ulcerative primary syphilis) increases the risk of HIV transmission.1,9,10 Best practice is not clear for syphilis evaluation, treatment and monitoring of treatment response in HIV co-infected patients due to lack of controlled comparison studies.6,11,12
In the last decade re-emergence of syphilis has been documented worldwide disproportionately among patients infected with HIV. 13 In Europe, US and Australia syphilis rates have increased by 3 to 14-fold, mostly among men who have sex with men (MSM). 13 18 However, most of the 12 million new syphilis infections reported annually are from Asia and sub-Saharan Africa. 6 Ethiopia, like many African countries, is experiencing a severe HIV/AIDS epidemic. The prevalence of syphilis seroreactivity in Ethiopia is 20–30% in men and 2–27% in women measured in different regions of the country. 19 21
In our Israeli AIDS center, the majority of HIV-infected patients are immigrants from Ethiopia (70%), many of the remainder have immigrated from Eastern Europe, mainly the former USSR, with a small proportion from other countries, or born in Israel. Highly active antiretroviral therapy and medical surveillance are available at no cost to all HIV-infected patients in Israel. The population rate of syphilis in Israel has increased 10-fold in the last decade from 0.0003% to 0.004%, mostly due to immigration from Ethiopia and the former USSR. 22
The aim of this study was to evaluate the prevalence of seroreactivity to syphilis among HIV-infected patients in our AIDS center, and to analyse the clinical presentation, degree of CNS involvement and treatment outcome of HIV/syphilis co-infected patients.
Patients and Methods
Study design
A retrospective study from a single Israeli HIV-AIDS center (Kaplan Medical Center, Rehovot, Israel) from January 2000 to December 2005.
Data collection
A total of 1060 files of HIV-infected patients were evaluated for serological and clinical evidence of syphilis. Patients were tested for non-specific and specific treponemal antibodies simultaneously with Venereal Disease Research Laboratory (VDRL) and enzyme immunoassay (EIA), respectively, as this is the routine evaluation in Israeli hospitals. Each patient underwent serological evaluation at their first medical check-up as part of the routine screening performed for every new patient. A previous diagnosis of syphilis and any prior treatments were documented. Yearly treponemal serology was performed on patients with prior positive serology as well as patients at risk of subsequent exposure to syphilis. Positive serology was repeated within two to three months in order to confirm positivity; syphilis EIA reactivity on two separate sera was considered confirmatory. Patients with syphilis seroreactivity were further evaluated for demographic data, time of HIV diagnosis, HIV disease status, VDRL levels, cerebrospinal fluid (CSF) analysis (if performed), syphilis treatment and treatment response. Data collection was approved by the local Helsinki committee.
Laboratory methods
Sera and CSF were tested for VDRL utilizing the Syphscreen kit (Axis-Shield Diagnostics, Dundee, UK); VDRL levels were determined for dilutions of 1:1 to 1:32. CSF analysis for protein and leucocytes were performed using standard methods. Sera were analysed for specific T. pallidum IgG, IgM and IgA antibodies using the CAPITA™ Syphilis TA EIA (Trinity Biothech, Bray, Co. Wicklow, Ireland).
HIV viral load was determined with the use of the COBAS Ampliprep/COBAS AMPLICOR HIV-1 MONITOR Test, version 1.5 (CAP/CA; Roche Molecular Systems, Branchburg, NJ), with plasma levels below 400 copies/mL deemed to be ‘undetectable’ as was appropriate at that time. CD4 cells were determined by fluorescence-activated cell sorting (FACS) using fluorescein isothiocyanate (FITC)-conjugated monoclonal antibodies (IQ Products, Groningen, Netherlands).
Clinical diagnosis
Early syphilis (i.e. primary, secondary and early latent) was determined either when symptoms were apparent or when seroconversion was documented within 12 months. Late latent disease was defined as having positive treponemal serology of more than one year or of unknown duration.
As recommended by the Centers for Disease Control and Prevention (CDC) for HIV-infected patients who have either late latent syphilis or syphilis of unknown duration, a CSF examination by lumbar puncture (LP) was offered to all patients in this stage. Neurosyphilis was defined as the presence of CSF pleocytosis (WBC > 10 cells/mL) or reactive CSF–VDRL serology; CSF-protein was not used for this definition due to the various other reasons for elevated CSF-protein in HIV-infected patients.
Treatment and treatment response
All patients diagnosed with syphilis (according to serology) received recommendation for one of two treatment protocols according to the CDC guidelines. Patients with no evidence of neurosyphilis or those who refused LP received a recommendation for treatment with three intramuscular injections weekly of 2.4 million units (MU) of benzathine penicillin (the intramuscular protocol). Patients diagnosed with neurosyphilis were encouraged to receive treatment with 10 days of high dose (24 MU) intravenous penicillin (the intravenous protocol).
Blood samples for VDRL levels were obtained 12 and 18 months following treatment. Treatment success was defined as a four-fold decline of VDRL level from pretreatment levels or sustained level for very low primary levels of VDRL, within the first 12–18 months of follow-up. Treatment failure was defined as four-fold or more increase of VDRL level within the following 12–18 months. ‘Serofast’ response was allocated when treatment success or failure criteria were not met. 3
Data analysis
The statistical analysis was performed by the Student's t-test, χ 2 test or Fisher's exact test as appropriate. P ≤ 0.05 was considered significant.
Results
Rate of co-infection
In the study period (2000–2005) 1060 HIV-infected patients were evaluated for VDRL and EIA serology; 162 (15.2%) had seroreactivity for which 150 files were available and thus included in the study. VDRL and EIA serology were routinely performed for every ‘new’ HIV patient as well as following anti-syphilis therapy. In our AIDS center there are 80–100 ‘new’ patients per year (i.e. newly diagnosed or new to the clinic). The rate of treponemal seroreactivity among all sera screened increased 20-fold, from 1.8% in 2000 to 36% in 2005. This increased prevalence was higher than expected for the stable annual increase of patients in our clinic.
Clinical and demographic data
Of 150 patients with treponemal seroreactivity, 134 (93%) were of Ethiopian origin, 4% were immigrants from the former USSR and 3% were ‘native’ Israelis. In our cohort, 70% of HIV-infected patients were immigrants from Ethiopia, thus syphilis was diagnosed in 19% of them. The mean age of co-infected patients was 42 ± 11 years and 57% were men. Ninety-five (62%) patients were diagnosed with HIV/syphilis co-infection on their first visit to our clinic, whereas 55 (38%) patients seroconverted during follow-up. Primary syphilis was diagnosed in two patients, secondary syphilis in five patients and early latent disease in 8 patients. Most patients (135) were diagnosed with late latent or unknown duration of disease, of which five died during the study period. Eleven patients with late latent syphilis presented with symptoms compatible with tertiary disease, eight had cognitive/psychological impairments, two had aortitis and aortic valve disease confirmed by echocardiography and one had severe hearing impairment. These patients were treated according to their clinical status and were not included in the analysis of those who had CSF evaluation in this study. At the time of syphilis diagnosis, the mean HIV viral load was log 5.5 ± 6.2 copies/mL, 57 (37%) patients had viral loads below detection level (<400 copies/mL) and the mean CD4 cell count was 380 ± 260 cells/mm3.
CNS involvement
Characteristics of syphilis/HIV co-infected patients regarding cerebrospinal fluid (CSF) reactivity
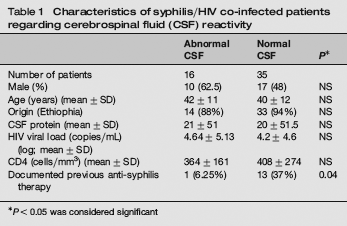
*P < 0.05 was considered significant
Treatment response
Response to therapy with penicillin in 81 syphilis/HIV co-infected patients
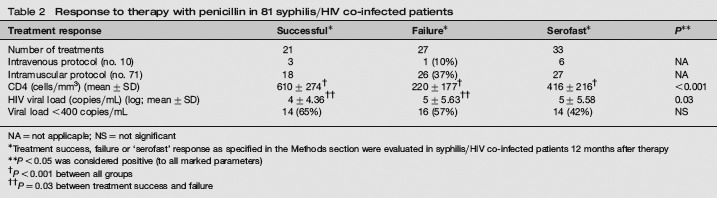
NA = not applicaple; NS = not significant
Treatment success, failure or ‘serofast’ response as specified in the Methods section were evaluated in syphilis/HIV co-infected patients 12 months after therapy
P < 0.05 was considered positive (to all marked parameters)
P < 0.001 between all groups
P = 0.03 between treatment success and failure
Although not statistically significant, treatment failure was observed only in one (10%) of 10 patients treated for neurosyphilis (intravenous protocol) and one (16%) of six patients treated for early disease (intramuscular protocol) compared with 25 (38%) of 65 patients with late latent disease who received the intramuscular protocol.
Pretreatment levels of VDRL or CSF pleocytosis did not correlate with treatment outcome in the 10 patients with neurosyphilis.
Discussion
A significant increase in syphilis/HIV co-infection was observed in our cohort during 2000–2005. In total, 15.2% of all HIV-infected patients had syphilis seroreactivity, 93% of whom were heterosexual immigrants from Ethiopia. In our region (southern Israel) 70% of the HIV-infected patients are immigrants from Ethiopia, and thus, co-infection was diagnosed in 19% of them. A high prevalence of co-infection was also documented among immigrants living in the northern part of Israel 23 as well as in other Western and African countries.6,7,14,15 In Ethiopia, syphilis seroreactivity was documented in 13–29% of high-risk populations. 19 21
In the current study, 39% of HIV-infected patients had syphilis seroconversion during follow-up, implying that syphilis was acquired following the diagnosis of HIV. This, emphasizes the need for epidemiological and educational programmes that will address sexually transmitted infection prevention in high-risk populations.
A low rate of primary and secondary syphilis was observed in our cohort compared with studies from Europe, UK and the USA.12,15 In general, 33–56% of patients with early syphilis are asymptomatic,15,18,24 and HIV can modify syphilis manifestations and obscure the diagnosis of early disease. Moreover, differences between studies may reflect genetic differences between populations or the lower likelihood of African patients to approach medical facilities. 20 As early diagnosis of syphilis facilitates its management, improves treatment response and decreases complications,3,18 it seems logical to recommend yearly screening for syphilis in all HIV-infected patients.
CNS involvement was suspected in 31 % of patients with late latent syphilis who underwent CSF examination, which is consistent with previous reports of CNS involvement among co-infected patients.12,25 However, in contrast to some reports 25 we did not find correlations between CNS involvement and CD4 counts or VDRL levels (Table 1). CD4 counts differ between populations and therefore may not be useful for determination of CNS involvement in our cohort, whereas VDRL levels differ among laboratories and are not easily comparable. Moreover, unlike some studies we offered LP only to patients with late latent syphilis, therefore the role of CD4 cell counts and VDRL levels in patients with early syphilis was not addressed in this study. Thus, it seems that LP should be offered to all co-infected patients with late latent syphilis, regardless of their immune status or VDRL levels, both factors which are currently not included in the CDC recommendations for LP. 3 CNS involvement negatively correlated with a history of past penicillin treatment in our study, suggesting that formerly treated patients, probably in the earlier stages of syphilis, were less likely to be diagnosed with neurosyphilis. Clearance of spirochetes from the CNS following early treatment of syphilis has been reported.3,11
The recommended treatments for syphilis resulted in only 26% of successful responses in the present study and a relatively high rate of ‘serofast’ (41%) and treatment failures (33%). The increased prevalence of ‘serofast’ reaction has been reported in co-infected patients previously. This might be attributed to HlV-associated hyperglobulinaemia or a longer period of time (2–5 years) required for VDRL levels to decline in HIV-infected patients, especially those with prolonged infection or low VDRL levels (<1:8). 26
A high rate of syphilis treatment failures has been previously reported, especially in patients with prolonged disease. 26 30 In our cohort, 33% of treatments failed and this correlated with patients’ immune status and duration of treponemal infection (Table 2). Thus, it might be speculated that a weaker immune system might encounter difficulties in eradicating infection. Further studies are needed as a prolonged or more potent therapy (i.e. combination therapy) might be required for this subgroup of co-infected patients. Furthermore, treatment failure might be influenced by different treatment protocols. Although not statistically significant, failure was observed in 37% of patients with late latent disease treated with the intramuscular protocol versus 10% of those treated with the intravenous protocol. These protocols differed by the type of penicillin, method of injection, duration of therapy and treatment location, as intramuscular penicillin was given by community physicians whereas intravenous penicillin was given in hospital. We could not conclude whether treatment responses differ due to protocol potency or lack of compliance to the ambulatory intramuscular protocol.
There are several limitations to this study: being a retrospective, single centre study our results might not be extrapolable to other centres or populations. Furthermore, CSF examinations were performed in only 39% of patients with late latent syphilis and were not repeated following treatment. This limits our ability to measure successful treatment outcomes in the CSF.
In conclusion, increased syphilis seroreactivity was observed in our cohort of HIV-infected patients, mainly of Ethiopian origin. Possible benefits of treatment intensification in this subgroup of co-infected patients, as well as issues of compliance, need to be addressed by a larger prospective study.