
Abstract
Progressive multifocal leukoencephalopathy (PML) is still a underinvestigated central nervous system infection, often linked to HIV-related immunodeficiency. We present an unusual case report characterized by motor involvement, which occurred as the first AIDS-defining event in the absence of appreciable immunodeficiency in a patient with previously undiagnosed HIV infection, who was also assessed by a functional–metabolic magnetic resonance imaging technique (MRI–spectrometry). A 45-year-old patient had HIV infection detected after the appearance of motor abnormalities, in the absence of other signs or symptoms. No significant immunodeficiency was found (initial CD4+ lymphocyte count of 566 cells/µL), and HIV viral load was 24,000 RNA copies/mL. Combination antiretroviral therapy was started with lamivudine, abacavir and lopinavir/ritonavir, with subsequent addition of efavirenz and enfuvirtide. Elevated cerebrospinal fluid levels of JC virus (JCV) (11,668 copies/µL) and consistent neuroradiological findings at contrast-enhanced computed tomography and MRI scans confirmed a diagnosis of PML. Despite the aggressive therapeutic approach, which achieved undetectable HIV viraemia, a CD4+ count above 700 cells/µL and disappearance of JCV after 20 days, the neurological motor involvement rapidly deteriorated, yet associated cognitive impairment never occurred. Clinical and neuroradiological deterioration occurred, and our patient died five months after the diagnosis due to respiratory failure. Combined MRI–spectrometry studies performed 10 days before death included proton (1H) spectrometry, and an MRI study-calculation of water diffusion and anisotropy: through this innovative technique combining morphological and metabolic findings, multiple abnormalities involving the subtentorial white matter were detected (with multiple encephalic trunk and ponto-bulbar lesions), which usually are not part of the PML course.
INTRODUCTION
Progressive multifocal leukoencephalopathy (PML) is a rare central nervous system (CNS) disease, characterized by diffuse cerebral and cerebellar demyelinating lesions, first described in the year 1958. Since the 1960s and 1970s, the association of PML with primary or secondary (i.e. iatrogenic) cell-mediated immune deficiency, haematological disorders or other malignancies was already evident. 1–4 However, starting from mid-1980s, HIV-related cell-mediated immunodeficiency became the most frequent underlying condition for the development of PML. 5–9 As measured by an absolute CD4+ T-lymphocyte count, the underlying immunodeficiency proved extremely low in the great majority of described cases of PML, 3,7–9 especially in the setting of HIV infection, and in the era preceding the introduction of potent combination antiretroviral therapies (cART). In our single-centre series of 34 consecutive patients, all 18 subjects observed until 1996 had a CD4+ count below 50 cells/µL, 10 while the remaining 16 cases confirmed since 1997 (save the present episode) had a mean CD4+ count of 78.3 ± 45.2 (range 3–235) cells/µL, with only two subjects above the threshold of 200 CD4+ cells/µL10 (Manfredi R, unpublished observation, 2009).
The Polyomavirus JC has been demonstrated to be the causative agent of PML. It seems to remain latent in the kidney tissue from infancy, and becomes pathogenic and CNS-tropic after being transported by peripheral mononuclear cells, in the presence of a deep cell-mediated immunodeficiency. 6 Anecdotal literature reports claimed PML or PML-like syndromes apparently attributed to human herpes virus type 6 (HHV-6), 11 while in one haematological patient a dual JC-HHV-6 infection was found. 2
From a pathogenetic point of view, the demyelinating activity of JC virus (JCV) seems to be mediated by specific damage caused by the so-called ‘antigen T’ on oligodendrocytes. 6 From a pathological point of view, a very recent study 12 underlined the cortical demyelination typical of PML, which is associated with relative axonal sparing as a distinct feature when compared with other demyelinating disorders. 12
The multiform neurological picture depends on the progressive, severe and often asymmetric multifocal demyelinating lesions of the brain cortex, with inexorable progression towards a vegetative status and ultimately death due to cachexia, wasting syndrome and overwhelming infectious complications. 8,9 The initial, insidious and often atypical first appearance is usually followed by focal deficits, dizziness, coordination deficits, hemiplegia, and memory and cognitive impairment, while headache, seizures and neck stiffness are infrequent. In the pre-cART era, the average prognosis among HIV-infected patients was limited to six months from the occurrence of early neurological signs and symptoms, although one case of apparent spontaneous remission has been reported in a non-HIV-infected patient with Hodgkin's lymphoma, 13 and some long-term survivors were related to a blunted local inflammatory reaction. 5
Among instrumental studies, the electroencephalographic findings may help the diagnosis, but the neuroimaging studies (contrast-enhanced computed tomography [CT], and especially magnetic resonance imaging [MRI]) are usually sufficient to demonstrate the typical brain and cerebellum white matter alterations without mass effect (with the well known greater efficiency of MRI techniques in assessing the white matter abnormalities). 14–20 While in the pre-cART era, many PML diagnoses were revealed only post mortem examination of patients affected by multiple, AIDS-related opportunistic diseases, 8 invasive CNS biopsy followed by histopathological studies has been replaced in the last decade by the ability to defect JC DNA virus by hybridization assays and especially quantitative molecular biology assays (polymerase chain reaction) performed on the cerebrospinal fluid (CSF), with techniques validated since the mid-late 1990s. 2,18
Unfortunately, no specific treatment of PML is presently available. Since the mid-1970s multiple trials have been carried out with cytarabine, 10,21,22 adenine arabinoside, and also transfer factor, and various types of interferons; 16 more recently, an anecdotal report suggested a possible role for the antiviral compound cidofovir. 23 With regard to the role of cART in HIV-infected patients, a potentially favourable effect is expected by the parallel action against the main HIV comorbidities (at CNS level, too), and especially in prompting a rapid and effective immune system recovery 7,24 (although some cases of initially suspected PML were probably misinterpreted by the rapid and massive immune reconstitution following effective cART), but unfortunately no antiretroviral compound of any available class has been shown to be effective against JCV. 7,24
CASE REPORT
A 45-year-old patient with a negligible clinical history had HIV infection detected after hospitalization due to the sudden appearance and rapid worsening of predominantly motor abnormalities (dysarthria and coordination anomalies, most right sided, followed by apraxia and horizontal ophthalmoparesis), in the absence of other relevant signs and symptoms. HIV infection was revealed in the absence of an appreciable immunodeficiency (as measured by an absolute CD4+ lymphocyte count of 566 cells/µL), while the measured HIV viral load was limited to 24,000 HIV-RNA copies/mL (branched-DNA technique). A potent cART regimen was started immediately with lamivudine, abacavir and lopinavir/ritonavir (drugs characterized by an elevated brain penetration), with subsequent addition of both efavirenz and enfuvirtide (antiretroviral drugs with different mechanisms of action compared with the previous ones). The virological studies of CSF showed elevated levels of the PML-associated JCV (11,668 DNA copies/µL), enabling the diagnosis of PML to be made. MRI findings included multiple T-2 weighted hyperintense lesions involving thalamus, posterior arm of the internal capsule and cerebral pedicles, and later in the course of disease also pontine-bulbar lesions were seen. No other HIV-associated disorders were found, other haematological, clotting and biochemistry profiles tested within normal limits, and all microbiological investigations were negative.
Despite the aggressive antiretroviral treatment, which achieved undetectable HIV viraemia, a CD4+ lymphocyte count above 700 cells/µL and the disappearance of JCV from CNS after only 20 days, the neurological picture deteriorated rapidly, predominantly in motor function (anarthria, severe dysphagia, trunk-limbs paresis, sphincter abnormalities, later associated with diffuse and peripheral tremors, with an associate myoclonic component at the left side), while relevant cognitive impairment never occurred. Enteral nutrition (including the administration of oral anti-HIV drugs) was carried out without complications. Clinical neuroradiological (CT-MRI) deterioration occurred, and our patient died five months after the initial diagnosis of PML due to respiratory failure.
A combined MRI–spectrometry study performed 10 days before death included a proton (1H) MRI–spectrometry and an MRI study-calculation of water diffusion and anisotropy (Figure 1). Through this innovative technique allowing the concurrent assessment of multiple morphological and metabolic findings, a number of metabolic and microstructural abnormalities diffusely involving the subtentorial white matter were detected. The extensive alterations involved cerebellar hemispheres, the encephalic trunk and ponto-bulbar structures; the latter usually are not considered part of the HIV-associated PML course, with associated cerebral hemisphere alterations (optic radiation, parietal-occipital white matter and corpus callosum). In particular, the single-voxel proton spectroscopy showed a 23% and 22% reduction of choline and N-acetyl aspartate, respectively, in the thalamus while no lactate and lipid accumulation was found, and myo-inositol concentration was within normal limits. When examining with the same technique the left parietal-occipital white matter, a 19% and 21% reduction of content of N-acetyl-aspartate and choline was found, while myo-inositol was increased by 36%; again, no increased amount of lactate and lipids was detected.
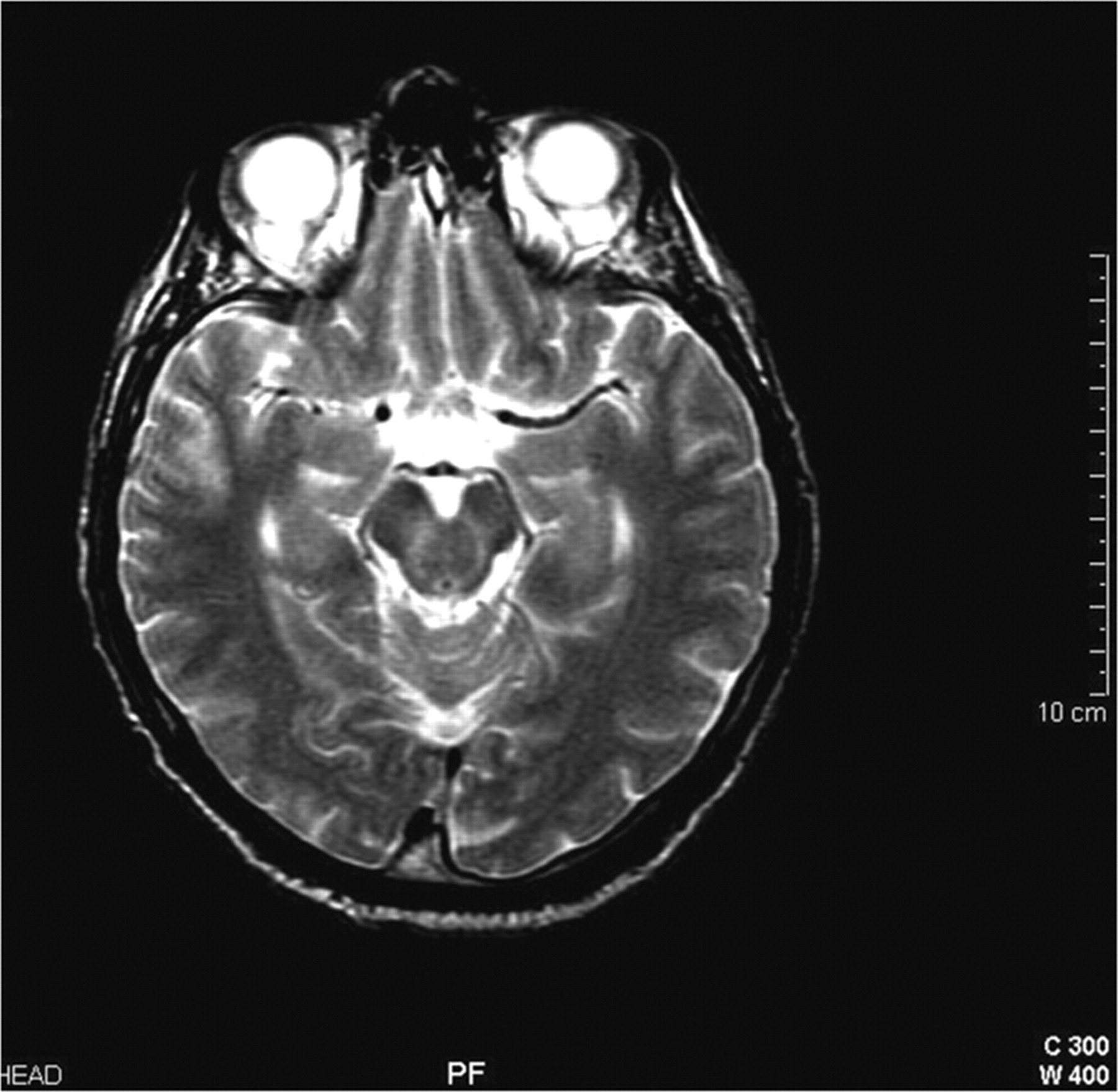
A combined magnetic resonance imaging (MRI) plus spectrometry study included a proton (1H) MRI–spectrometry and an MRI study-calculation of water diffusion and anisotropy
DISCUSSION
Even 12 years after the introduction of cART in 1996, opportunistic disorders and multiple HIV-related illnesses are still common among HIV-infected patients, 7,9,25 predominantly due to missed or neglected HIV disease (and the consequent lack of access to cART), and probably also due to residual immune system imbalances, and the intrinsic pathogenicity of HIV itself (with special reference to HIV-associated malignancies and degenerative disease). Moreover, ‘novel’ illnesses and disease expressions triggered by immune recovery (the so-called ‘immune reconstitution syndrome’), further complicated the clinical picture with multiple HIV-related disorders (including those of the CNS), 26 seen especially when baseline values of patients starting cART reflect advanced disease.
CNS disorders as a whole are still frequent in the setting of HIV disease in the third millennium, 7,9,18,26 and PML is one that remains somewhat underinvestigated, from both a diagnostic and therapeutic point of view. The present case shows that an HIV- and JCV-associated PML may occur as the first AIDS-defining event in patients who are unaware of their HIV infection, and PML disease may coexist with other HIV-associated disorders, thus complicating and/or delaying its recognition. 25 Moreover, the history of our patient shows that HIV-associated PML may rapidly evolve with atypical clinical features (with motor deficits largely prevailing over cognitive ones), even when the initial CD4+ count is well above 500 cells/µL, and a quick decay of both plasma HIV-RNA and CSF JCV-DNA viral loads are achieved after immediate, aggressive cART.
A broad range of neurological abnormalities may be seen in HIV-infected patients, but diagnostic and management may be delayed by concomitant depression, motor impairment and lethargy associated with wasting, and may be masked or worsened by concurrent pharmacological treatments. As a consequence, motor, cognitive and behaviour anomalies may underlie a number of potential neurological disorders. Therefore, even a combination of clinical, laboratory and neuroimaging studies may fail to provide a definite diagnosis. New developments in quantitative MRI spectroscopic imaging (as well as those obtained by SPECT techniques and other neuroimaging assays) are expected to add significantly to the diagnostic process by allowing dynamic and metabolic assessment and monitoring of morphological changes. 20,27
When focusing our attention on PML and other demyelinating CNS complications HIV disease, few reports exist of MRI spectroscopy studies and related techniques. 19,20,28–31 A 1998 paper assessed the role of proton MRI spectroscopy in detecting metabolic changes in a broad spectrum of focal or diffuse HIV-related lesions versus seronegative controls. 28 Eight patients with PML were also included and showed a quite homogeneous metabolic pattern: a lactate signal (an inflammatory marker) was found in six out of eight subjects with a diagnosis of PML, while this marker had a lower incidence in the other HIV diagnostic groups (P < 0.0003), so that spectroscopy–MRI was claimed as a potential adjunct to MRI in differentiating CNS white matter lesions (such as HIV-related encephalopathies) from PML. 28 A subsequent study on six patients with AIDS-related PML compared with a control group noticed a significantly reduced N-acetylaspartate and lactate content, and increased choline and lipid levels, with a homogeneous pattern in the sample. 29 The absence of thallium-201 brain uptake at SPECT examination in association with choline and lactate increase and preserved N-acetylaspartate at proton MRI study has been claimed to add to the differential diagnosis of PML in HIV-infected 31 and non-HIV-infected 32 patients.
On the other hand, when assessing non-HIV-associated pathological conditions evaluated with MRI-spectroscopy techniques, extra-signals from lactate and glucose were confirmed in a broad range of disorders characterized by vanishing white matter in HIV-negative individuals. 33 In a newly-described form of leukoencephalopathy with onset in childhood and involvement of the spinal cord, increased lactate within the abnormal white matter was found at MRI-proton spectroscopy in three of the five cases studied. 34 A diagnosis of PML associated with a rare idiopathic CD4+ deficiency was posed in a single, anecdotal patient who also received an MRI–proton spectrometry. 4 Proton MRI–spectroscopy was recently employed together with diffusion tensor imaging to confirm a possible PML in a non-HIV-infected women without any evident immunodeficiency: reduced N-acetyl aspartate and increase choline contents were found in the involved brain white matter. 35 Recently, an autosomal recessive brainstem and spinal cord PML was described from Brazil: in the three examined cases, spectrometry–MRI contributed to the diagnosis depicting cerebral and cerebellar white matter abnormalities with associated increased lactate levels. 36
The neuroradiological features of our patient (contrast-enhanced CT and MRI scans) were implemented by ultraspecialistic spectrometry–MRI techniques, which are demonstrating value in the assessment of primary and secondary neurological abnormalities, 20,27 although complete validation and reference standards are still lacking for some neurological disorders, including the most infrequent HIV- and immunodeficiency-associated disorders. 4,19,20,27,29,30,33,34 Through these metabolic-imaging studies, a predominantly subtentorial disease localization was demonstrated and assessed, while the usual PML-related abnormalities tend to involve the brain and cerebellar white hemispheres.