
Abstract
A 33-year-old man who developed progressive multifocal leukoencephalopathy (PML) with HIV infection is reported. The patient exhibited rapid decline in neurological status after initiation of antiretroviral therapy (ART), which was attributed to the PML-immune re-constitution inflammatory syndrome. Following the administration of mefloquine in combination with ART, the patient's neurological status improved substantially. This case suggests that further investigation of the use of mefloquine might be warranted for treatment of PML in HIV-infected patients.
CASE REPORT
A 33-year-old HIV-infected man started to develop slurred speech, according to his family, in mid-August 2009. He had never received antiretroviral therapy (ART) and never had opportunistic infections. Upon initial visit to our institution, neurological examination revealed dysarthria and sensory defect of left angle of the mouth. Brain magnetic resonance imaging (MRI) showed multiple hyperintense white matter lesions of the occipital lobes bilaterally on fluid-attenuated inversion-recovery imaging (Figures 1a and b). He was admitted the following week for further work-up. His CD4 T-cell count and plasma HIV-RNA were 269 cells/μL and 8700 copies/mL, respectively. The results of cerebrospinal fluid (CSF) examination were as follows: nucleated cells 12/μL, glucose 3 mmol/L, protein 27 g/L; polymerase chain reaction (PCR) for John Cunningham virus (JCV) was positive. We diagnosed his status as progressive multifocal leukoencephalopathy (PML) from neurological and radiological findings. ART consisting of abacavir/lamivudine and lopinavir/ritonavir was initiated. Upon initiation of ART, he exhibited deterioration of dysarthria and hemiparesis with left upper dominance. In addition, he presented dysphagia, right central pattern facial paresis and sensory aphasia. Repeat brain MRI performed two weeks later showed the progression of the white matter lesion (Figures 1c and d) and mild contrast enhancement, suggesting PML-immune re-constitution inflammatory syndrome (PML-IRIS) (Figures1e and f). He received prednisolone 30 mg/day and a 5-hydroxytryptamine receptor 2a (5HT2a) antagonist, risperidone, was initiated to inhibit JCV propagation.
1
Since his status remained unchanged following these therapies, we tapered the dose of prednisolone and discontinued over the next two weeks. The lack of expected clinical improvement led us to search for unconventional therapy for salvage. We found a report that mefloquine, an antimalarial drug, inhibited JCV replication in vitro
2
and decided to add mefloquine after the permission from Institutional Review Board (accession number: 21–32). After initiating mefloquine, no further clinical deterioration was noted. Furthermore, within 30 days, his neurological symptoms started to improve gradually, with the reduction of abnormal lesion volume on MRI (Figures 1g and h). PCR for JCV in the CSF two months later was negative. The patient did not need any rehabilitation and was discharged from our hospital soon after. Risperidone was discontinued after six months of administration. The administration schedule of mefloquine was 250 mg/day for the first three days, and then 250 mg weekly for total of six months. No adverse events were identified during this time and there has been no evidence of clinical PML recurrence.
Magnetic resonance imaging (MRI) findings. (a, b) On 28 August 2009, fluid-attenuated inversion-recovery (FLAIR) imaging demonstrates areas of increased signals in the right and left bilateral occipital white matter. (c–f) Follow-up MRI on 14 September 2009. FLAIR imaging shows progression of white matter abnormalities (c, d). T1-weighted image after gadolinium injection shows mild contrast enhancement suggesting progressive multifocal leukoencephalopathy-immune re-constitution inflammatory syndrome (e, f). (g, h) FLAIR imaging shows regression of the white matter lesions in both hemispheres six months after mefloquine administration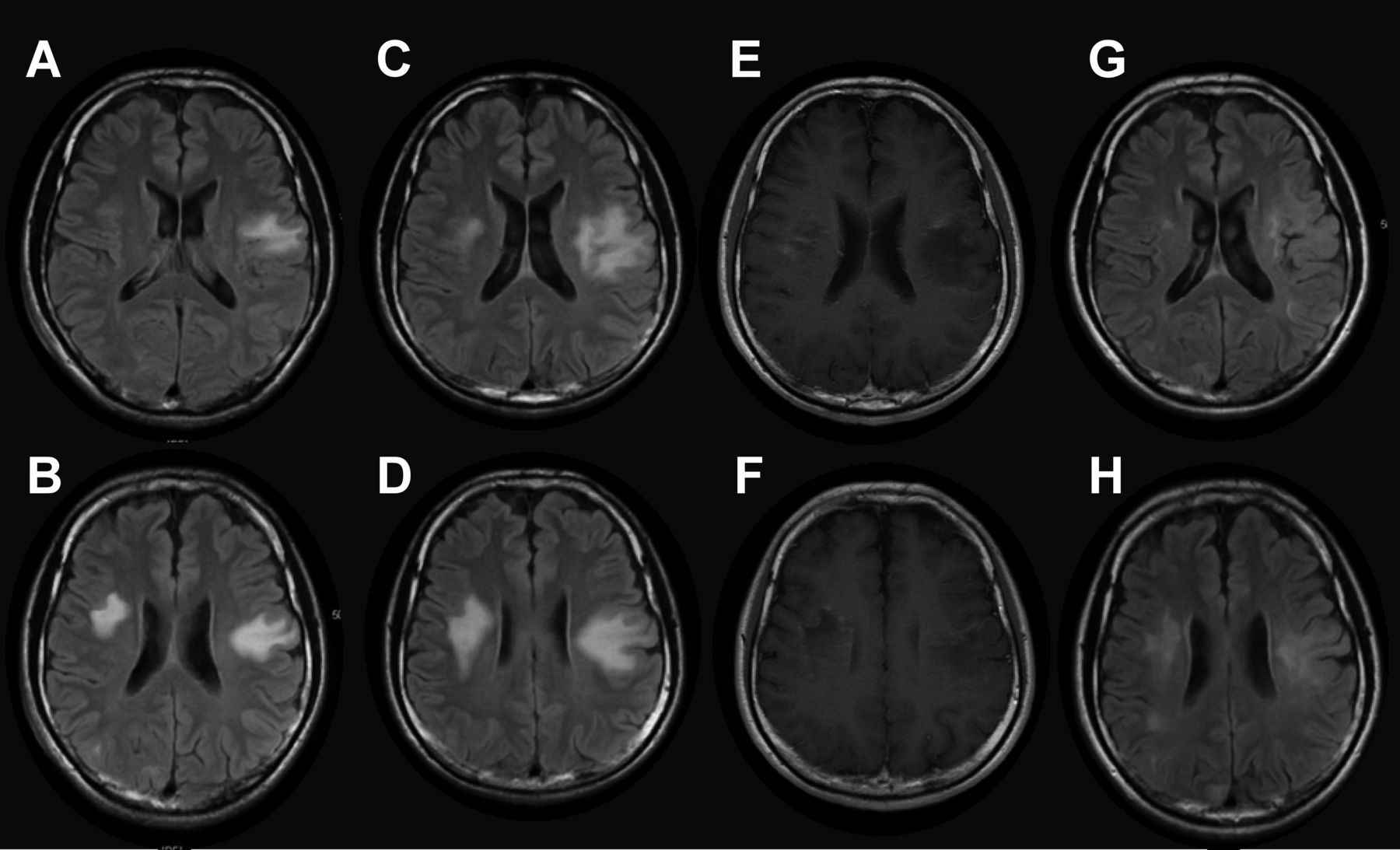
DISCUSSION
At present, the main approach to treatment of PML is to restore the host adaptive immune response to JCV. For HIV-infected PML patients, initiation or optimization of ART is the only therapy that has proven to be effective. However, PML still carries a significant mortality rate. Berenguer et al. 3 reported that one-half of the survivors exhibited some partial neurological improvement, but generally neurological deficits persist or progress due to irreversible brain damage. Hence, the search for specific treatment targeting JCV is imperative. Brickelmaier et al. 2 recently reported that mefloquine could inhibit replication of JCV in a cell culture system. Although the exact mechanisms by which mefloquine acts against JCV remain unclear, Phase I and II clinical trials have been in progress since September 2008 (ClinicalTrials.gov number, NCT00746941). One case report of non-AIDS-associated PML describes successful treatment with combination of mirtazapine (another 5-hydroxytryptamine receptor a [5HT2a] antagonist, like risperidone) and mefloquine. 4 Another case report of PML after umbilical cord blood transplant described partial clinical improvement after treatment with mefloquine. 5 This case exhibited significant recovery of neurological deficit and improvement of radiological findings after initiation of mefloquine. As both ART and risperidone had also been administered to our patient, it is difficult to determine whether any improvement can be attributed to mefloquine use. In addition, the administration of corticosteroids also complicates the evaluation of mefloquine's efficacy. However, we would like to highlight the substantial improvement of neurological symptoms after initiating mefloquine in spite of rapid deterioration after introduction of ART. In some studies, a higher CD4 T-cell count was associated with long-term survival for PML. 6 The good outcome observed in this case may have been affected by the patient's higher CD4 T-cell count at the time of PML onset.
In this case we were confronted by rapid progression of PML disease after initiation of ART. The neurological symptoms of PML may worsen in the setting of recovery of immune system, termed PML-IRIS. The pathophysiology of PML IRIS is poorly understood, it is speculated that activated CD4 and CD8 T-cells trafficking into the central nervous system are the main mediators of this phenomenon. Although the diagnosis of PML-IRIS can be challenging, contrast-enhancing lesions present in the brain can support this diagnosis. We regarded this case's initial neurological exacerbation as PML-IRIS based on clinical and radiological findings. Although a couple of studies showed a partial benefit of corticosteroids in PML-IRIS, 7 treatment with corticosteroids remains highly controversial. 8 However, in a patient with severe inflammation, we believe the anti-inflammatory effects of corticosteroids are warranted.
To our knowledge, this is the first case report describing potential benefit of mefloquine in an HIV-infected PML patient with IRIS. Although the efficacy and safety of mefloquine therapy awaits validation by ongoing clinical trials, our case demonstrates the potential benefit of mefloquine to improve neurological deficits in PML-IRIS patients.
Footnotes
ACKNOWLEDGEMENTS
This work was supported in part by a contract research fund from the Ministry of Education, Culture, Sports, Science and Technology (MEXT) for Program of Japan Initiative for Global Research Network on Infectious Diseases; Global COE Program (Center of Education and Research for Advanced Genome-Based Medicine – for personalized medicine and the control of worldwide infectious diseases) of MEXT; Research on international cooperation in medical science, Research on global health issues, Health and Labor Science Research Grants, the Ministry of Health, Labor, and Welfare of Japan; Health and Labor Sciences Research Grants (No. H24-AIDS-002) from the Ministry of Health, Labor and Welfare, Japan. We thank Kei Ouchi, MD, for his comments on drafts of the manuscript.