
Abstract
Integrase inhibitor-resistant HIV-1 was detected in the cerebrospinal fluid, but not in the plasma of a 42-year-old man with HIV encephalopathy treated with a raltegravir (RAL)-containing regimen. Raltegravir resistance may develop in the central nervous system when the virus is already multi-drug resistant because of different penetration into cerebrospinal fluid of individual antiretroviral agents.
INTRODUCTION
Raltegravir (RAL) is the first approved HIV-1 integrase inhibitor that has demonstrated potent antiretroviral activity in combination with an optimized background regimen in treatment-experienced patients. 1 However, RAL resistance develops relatively easily after virologic failure. 2,3 We describe here a case of HIV encephalopathy, in whom a major resistance mutation of integrase inhibitors was detected in the cerebrospinal fluid (CSF) but not in the plasma during RAL-containing antiretroviral treatment.
CASE REPORT
A 42-year-old man infected with HIV-1 presented with asthenia, skin hyperesthesia, loss of memory and psychomotor slowing. Magnetic resonance imaging (MRI) of the brain revealed diffuse bilateral and symmetrical increase in T2-weighted signal in the periventricular matter of the frontal and parieto-occipital regions. He was diagnosed with HIV encephalopathy based on the MRI findings and negative test results for other viral and bacterial infections, supported by a higher HIV-1 load in the CSF than in the plasma. During eight years of combination antiretroviral treatment (cART) (including zidovudine, didanosine, abacavir, efavirenz (EFV), indinavir and nelfinavir), multiple drug-resistance mutations were detected in plasma HIV-1, including A62V, V75I, F77L, Y115F, F116Y, Q151M, M184V and Y188L in reverse-transcriptase, and L10I, K20R, E35D, M36I, M46I, H69K, V82F and I93L in protease (at day −505). 4 The CD4 count was 246 cells/µL and the HIV-1 load was incompletely suppressed in the plasma (70–1200 copies/mL) over the preceding 15 months with cART of tenofovir (TDF), stavudine (d4T), lamivudine (3TC) and ritonavir-boosted lopinavir (LPVr), whereas active HIV-1 replication seemed to continue in the central nervous system (CNS) (120,000 copies/mL in CSF; Figure 1). In order to control HIV-1 replication, the cART regimen was modified to the combination of TDF, emtricitabine (FTC), EFV, darunavir (DRV), ritonavir (RTV), RAL and enfuvirtide (ENF) (day 0), resulting in successful HIV-1 suppression to below the level of detection (50 copies/mL) in both plasma and CSF on day 33, and the patient's CNS symptoms improved. ENF injection was stopped on day 58 though the other antiretroviral agents were continued. The CNS symptoms gradually deteriorated, although the plasma HIV-1 load was persistently suppressed below the level of detection (50 or 40 copies/mL), but the CSF HIV-1 load was found to have rebounded to a level of 440 copies/mL on day 224. ENF treatment was re-introduced, which resulted in the suppression of the CSF viral load to below the level of detection on day 253, and improvement of CNS symptoms; however, the patient showed gradual mood changes and developed psychiatric symptoms. ENF injection became difficult and it was stopped on day 358. By day 371, the HIV-1 load in the CSF was 4300 copies/mL but still undetectable in the plasma. Direct sequencing of the HIV-1 integrase gene identified a major mutation of RAL resistance (Q148R) in CSF, which was not detected by sequencing of earlier plasma (day −8) and CSF (day 224) samples. The above resistance mutations in reverse transcriptase and protease genes were detected in all successfully polymerase chain reaction-amplified samples. 4 The antiretroviral treatment was stopped on day 371 because of potential choking by the patient during swallowing. The HIV-1 load rebounded to 18,000 copies/mL in the plasma and 28,000 copies/mL in the CSF by day 405, in both of which no major RAL-associated mutation was detected.
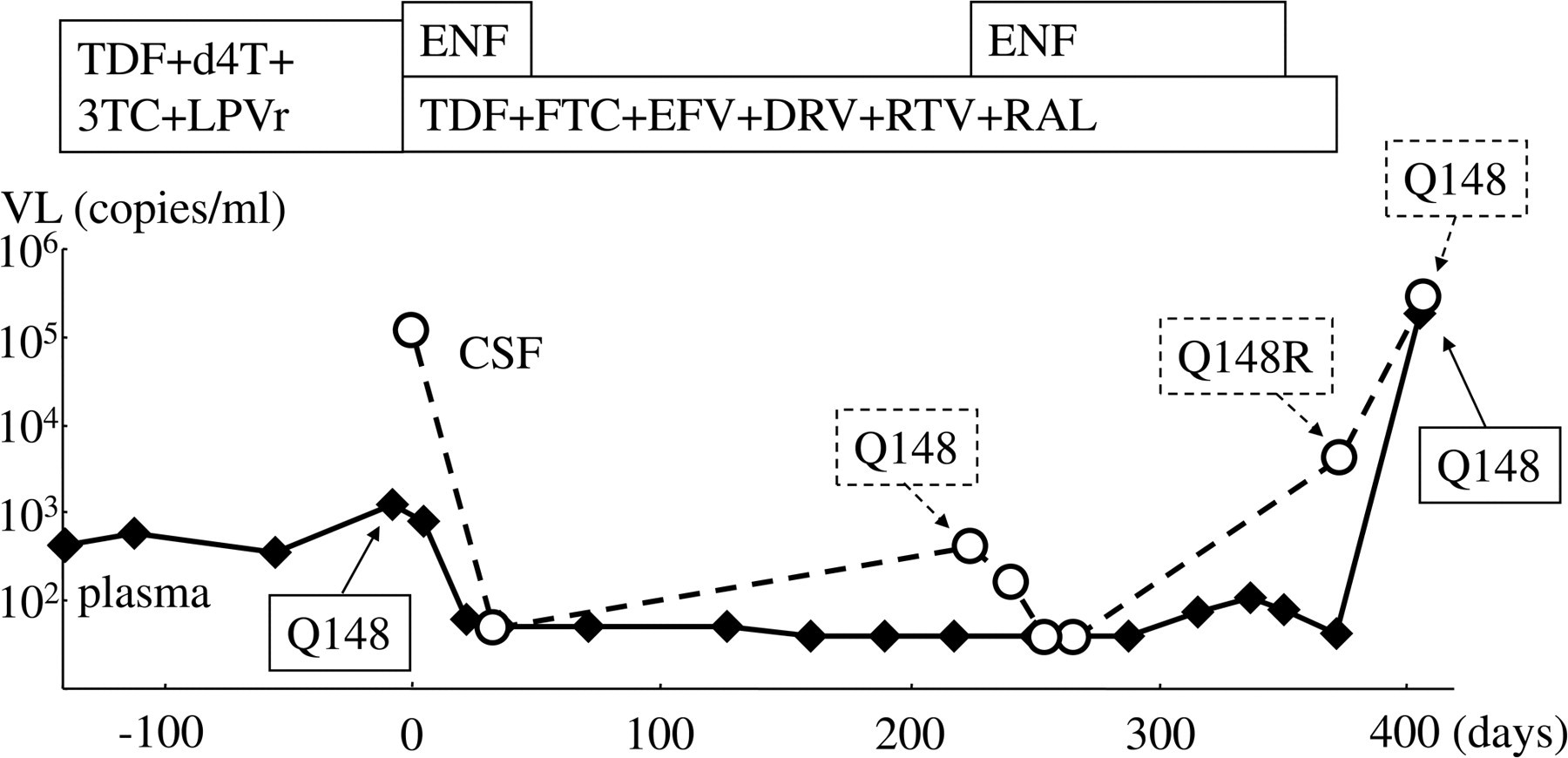
HIV-1 resistance mutations in the integrase gene and changes in viral loads (VL) in plasma and cerebrospinal fluid (CSF). HIV-1 integrase sequence was successfully analysed in two plasma samples (days −8, and 405) and three CSF samples (days 224, 371 and 405). A major mutation of raltegravir resistance (Q148R) was detected in only one CSF sample (day 371) which reverted to wild-type (Q148) after cessation of RAL-containing regimen (day 405). HIV-1 integrase gene could not be amplified from the plasma sample taken at day 371. No other integrase mutations listed in mutations figures or described in user notes of the International AIDS Society-USA Drug Resistant Mutation Groups were detected. 4 Multiple drug resistance mutations in reverse transcriptase (A62V, V75I, F77L, Y115F, F116Y, Q151M, M184V and Y188L) and protease genes (L10I, K20R, E35D, M36I, M46I, H69K, V82F and I93L) were persistently detected in all successfully amplified samples
DISCUSSION
In the present case of HIV encephalopathy HIV-1 load was persistently higher in CSF than in plasma, suggesting active viral replication in the CNS, which continued under RAL-containing regimen. RAL has a lower genetic barrier to resistance compared with protease inhibitors (PIs) to which multiple mutations are necessary for HIV-1 to attain significant resistance. 2,3 Recently, RAL was reported to penetrate well into CSF, whereas the penetration of DRV and EFV are extremely limited. 5–7 In the present case, the altered cART seemed to suppress multidrug resistant HIV-1 replication successfully in the systemic circulation and lymph nodes in the presence of effective concentrations of RAL, DRV, and EFV. However, in the CNS, active replication was suppressed only imperfectly, most likely due to lower concentrations of DRV and EFV in the CSF, which induced the emergence of HIV-1 variants resistant to RAL, the only drug fully active against the previous HIV-1 variants. This case study illustrates the potential for RAL resistance developing in the CNS when the virus is already multi-drug resistant.