
Abstract
The risk of HIV transmission via breastfeeding is well reported. We conducted a national survey in the UK to look at the current knowledge and postpartum practice of HIV physicians caring for HIV-positive pregnant women. In total, 167 questionnaires were distributed, 85 (51%) questionnaires were returned. All the respondents advised their patients against breastfeeding, 17 (23%) respondents routinely prescribed drugs for postpartum lactation suppression and 32 (43%) detailed awareness of interactions between antiretroviral therapy and dopaminergic lactation suppression agents. Thirteen respondents reported awareness of guidance on lactation suppression. The knowledge and use of lactation suppression agents appears to be low. However, its use will not only reduce postnatal mastitis and breast engorgement but will also help women deal with social pressures to breastfeed. Increased use in specific circumstances will improve the postnatal care of HIV-positive pregnant women in the UK.
INTRODUCTION
The risk of HIV transmission via breastfeeding is 5–20%. Studies are underway in resource-limited settings using extended antiviral prophylaxis to reduce the risk of HIV transmission by breast milk. In the UK, where safe alternatives to breast milk are available, exclusive formula feeding is the recommended method of infant feeding. We conducted a UK national survey to look at the current knowledge and postpartum practice of HIV physicians caring for HIV-positive pregnant women.
AIMS
To identify whether lactation suppression is routinely used in HIV-positive pregnant women, methods used and the level of awareness about currently available guidance.
METHODS
A paper-based questionnaire was sent to all the UK genitourinary medicine clinic leads involved in the care of HIV patients. Their responses were analysed using a Microsoft Access database.
RESULTS
In total, 167 questionnaires were distributed, 85 (51%) questionnaires were completed and returned. Of the respondents, 75 clinics were directly involved in the care of HIV-positive pregnant women, 55 (74%) clinics ran a joint obstetric/HIV service and 46 (61%) clinics had a named lead for the care of HIV-positive pregnant women. The total HIV cohort, including all men and women, in the clinics who participated in the survey varied from below 100 to over 2000 patients (Chart 1). The average number of pregnant women per year managed in the clinics each year ranged from 0 to over 50 women (Chart 2).
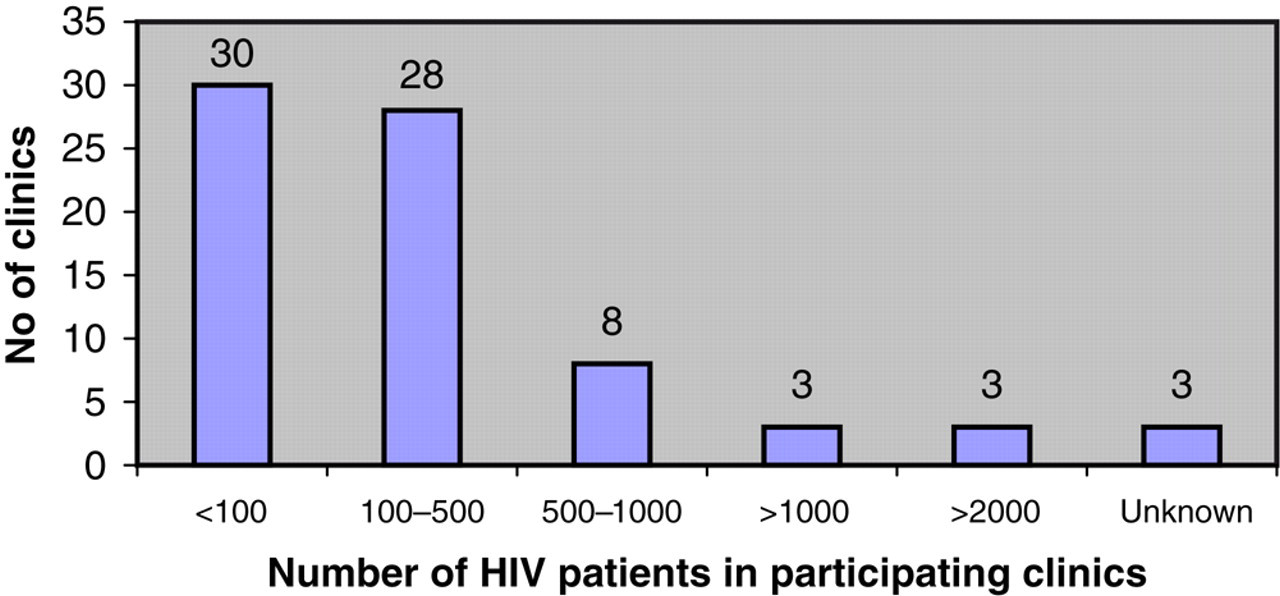
Total HIV cohort in participating clinics

Average number of pregnant women per year in participating clinics
Breastfeeding: All (100%) the respondents advised the women to avoid breastfeeding and 70 (93%) were sure that the women avoided breastfeeding.
Lactation suppression: Seventeen (23%) respondents routinely prescribed drugs postpartum for lactation suppression and of these 75% used cabergoline. One-third of the respondents were aware of one or more natural methods of lactation suppression. Thirty-two (43%) respondents were aware of the interactions between antiretroviral therapy and dopaminergic lactation suppression agents, with 22% indicating that the interactions were significant enough to avoid dopaminergics.
Awareness of available guidance: Thirteen (17%) respondents reported awareness of guidance on lactation suppression and six respondents were aware of specific British HIV Association (BHIVA) guidance on this subject. 1
DISCUSSION
We believe that this survey is the first of its kind to evaluate the postnatal care of HIV-positive pregnant women in the UK. It has shown that the awareness of lactation suppression methods, the interactions with antiretroviral therapy and awareness of guidance on the issue are low.
Non-pharmacological and pharmacological lactation suppression methods are available. Cabbage leaves, jasmine flowers, breast support, fluid restriction and ultraviolet lamps are among the non-pharmacological methods traditionally used. Sex hormones, frusemide, synthetic oxytocin, pyridoxine, bromocriptine and cabergoline are some of the pharmacological options available.
Of the pharmacological agents, bromocriptine and cabergoline have been extensively used. A Cochrane review concluded that there was no evidence to indicate whether non-pharmacological approaches are more effective than no treatment in suppressing lactation. 2 The same review reported that there were several trials supporting the efficacy of bromocriptine in suppressing lactation but concluded that there was weak evidence that it is better than having no treatment. 2 In addition, there are significant ergot side-effects with bromocriptine, including cardiovascular events. These side-effects are much less common with cabergoline, which is an effective lactation suppressant. A European multicentre trial concluded that cabergoline should be the drug of choice as it has a simpler single-dose administration schedule and a lower rate of adverse events. 3 Cabergoline is a selective dopamine D2 agonist and acts by reducing both the synthesis and release of oxytocin from the pituitary lactotrophs. 4 It is metabolized mainly by hydrolysis, its effect on cytochrome P450 enzyme system is minimal and hence there are no significant interactions with antiretrovirals.
Although the routine use of lactation suppression is not recommended, its use in selected situations will help to reduce postnatal morbidity such as mastitis, breast engorgement and pyrexia. In addition, it will help women overcome difficulties if they have social pressures to breastfeed.
CONCLUSIONS
The knowledge and use of postpartum medication to avoid breast engorgement and awareness of guidance on lactation suppression is low. Single-dose cabergoline is a safe and effective way of preventing breast engorgement and using it in specific circumstances will improve the postnatal care of HIV-positive pregnant women.