
Abstract
Although the Central American HIV epidemic is concentrated in high-risk groups, HIV incidence is increasing in young women. From 2005 to 2007, we conducted a cross-sectional study of pregnant women in a large public hospital and an HIV clinic in Guatemala City to describe risk factors for HIV infection and inform prevention strategies. For 4629 consenting patients, HIV status was laboratory-confirmed and participant characteristics were assessed by interviewer-administered questionnaires. Lifetime number of sexual partners ranged from 1 to 99, with a median (interquartile range) of 1 (1, 2). 2.6% (120) reported exchanging sex for benefits; 0.1% (3) were sex workers, 2.3% (106) had used illegal drugs, 31.1% (1421) planned their pregnancy and 31.8% (1455) experienced abuse. In logistic regression analyses, HIV status was predicted by one variable describing women's behaviour (lifetime sexual partners) and three variables describing partner risks (partner HIV+ , migrant worker or suspected unfaithful). Women in our sample exhibited few behavioural risks for HIV but significant vulnerability via partner behaviours. To stem feminization of the epidemic, health authorities should complement existing prevention interventions in high-risk populations with directed efforts towards bridging populations such as migrant workers. We identify four locally adapted HIV prevention strategies.
INTRODUCTION
The HIV epidemic in Latin America is remarkably diverse, with important differences in HIV prevalence and mode of transmission in the various subregions. 1,2 While injection drug use is a key epidemic driver in parts of South America, 2–4 HIV transmission in Central America (Belize, Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua and Panama), the region hit hardest by the epidemic is predominantly sexual and concentrated in men who have sex with men (MSM) and female sex workers (FSW). 3,5 Recent evidence suggests that many Central American MSM may also have sex with women. 6 These factors contribute to a distinct and an important role for heterosexual dissemination of HIV in Central America and suggest a potential for rapid epidemic spread. 2,6
Guatemala is a lower-middle income Central American nation of 13.4 million inhabitants with an HIV prevalence approaching 1%. 7 As of December 2007, an estimated 59,000 (95% confidence interval [CI] 41,000–84,000) adults aged 15–49 years were living with HIV in Guatemala, representing approximately 37% of estimated cases in the Central American region (authors' calculations based on 8–12 ; data for Belize not available). Ninety-four percent of infections in Guatemala are sexually transmitted; an additional 5% are transmitted from mother to child. 13 Epidemic growth continues with HIV prevalence for the general population expected to surpass 1% in 2010 and 1.5% in 2015. 13
While the male-to-female ratio of reported AIDS cases in Guatemala has remained relatively stable since 1994 at 2.31 to 1, 13 UNAIDS has recently voiced concerns that HIV incidence may be increasing in young women. 14 Epidemiological estimates for 2008 compiled by UNAIDS show an HIV prevalence among Guatemalan females aged 15–25 years of 1.5% as compared with an HIV prevalence of less than 0.1% for males in this age group – a 15-fold difference that suggests a possible shift in the population affected by the epidemic. 7 A high fertility rate of 4.3 per woman, 7 a young population with a median age of 19 years, 7 the presence of substantial poverty and income inequality, 15 and the importance of heterosexual transmission 6 reinforce concerns about progressive feminization of the Guatemalan HIV epidemic. 3,7,14
Valuable information on the epidemiology of HIV in populations of MSM and FSW in Central America is now available 6 ; however, understanding of HIV transmission dynamics in the region's general populations is sharply limited by the lack of national-level HIV surveillance systems. 3,5 In this context, HIV surveillance in pregnant women can provide important insights, helping us to understand who is affected by the epidemic and to identify common routes of transmission.
Our objective was to describe risk factors for HIV infection in a hospital-based sample of pregnant women in Guatemala City, Guatemala, to inform the development of locally adapted prevention strategies. To our knowledge, this is the first study to address this issue in Guatemala and the Central American region.
METHODS
Study design
A cross-sectional study of pregnant women attending the Hospital General San Juan de Dios (HGSJD), Guatemala City or the Clínica Familiar Luis Angel Garcia (CFLAG), a specialized HIV clinic located at the same site, from 2005 to 2007.
Setting
In 2004, Guatemala pledged to establish a national programme to reduce mother-to-child transmission (MTCT) of HIV from an estimated 30% to 5% for HIV+ pregnant women delivering in public health facilities. 16 In 2005 and 2006, we conducted HIV MTCT pilot projects at the HGSJD, one of Guatemala's two national hospitals. Located in Guatemala City, the HGSJD is a major teaching hospital serving a poor and ethnically diverse patient population. It has an active non-government organization (NGO)-run HIV clinic (Clínica Familiar Luis Ángel García, ‘CFLAG’). Since the end of the pilot studies, the HIV MTCT programme has continued to run at the HGSJD with support from the Global Fund to Fight HIV/AIDS, tuberculosis (TB) and malaria.
Study procedures
For the HIV MTCT pilot studies, all pregnant women presenting to antenatal care (‘MTCT pilot study 1’, intake dates 2005-04-01 to 2005-12-01) or to the delivery room during daytime (‘MTCT pilot study 2’, intake dates 2006-06-01 to 2006-09-30) at the HGSJD were offered counselling and an HIV test. Hepatitis and syphilis tests were also offered to all women reporting to the delivery room. All HIV+ women and their children were referred to CFLAG for treatment and follow-up. HIV MTCT interventions included triple combination antiretroviral therapy and a Caesarean section whenever feasible. Infants received zidovudine for six weeks postpartum, replacement feeding with infant formula, and were followed for a minimum of 24 months. HIV+ women also received clinically indicated care for their own HIV infection. The original goals of the MTCT study were: (1) to determine HIV prevalence in pregnant women at this site; and (2) to evaluate the impact of the HIV MTCT programme on clinical outcomes including treatment initiation and reduction of perinatal transmission. Identifying determinants of HIV status in women was a secondary study goal. We also recruited patients directly from CFLAG; HIV MTCT interventions were identical. Study protocols were approved by an independent local ethics committee certified by the US National Institutes of Health. All participants gave written informed consent.
Participants
Participants were recruited from the HIV MTCT pilot studies and from the CFLAG HIV clinic. The eligibility criteria were as follows:
All pregnant women reporting to antenatal care at the HGSJD during HIV MTCT pilot study 1; All pregnant women reporting to the delivery room at HGSJD during HIV MTCT pilot study 2; All additional women in care at CFLAG and pregnant between 2005 and 2007.
Figure 1 describes the recruitment of study participants. Data collection and measurement procedures were identical for all groups.
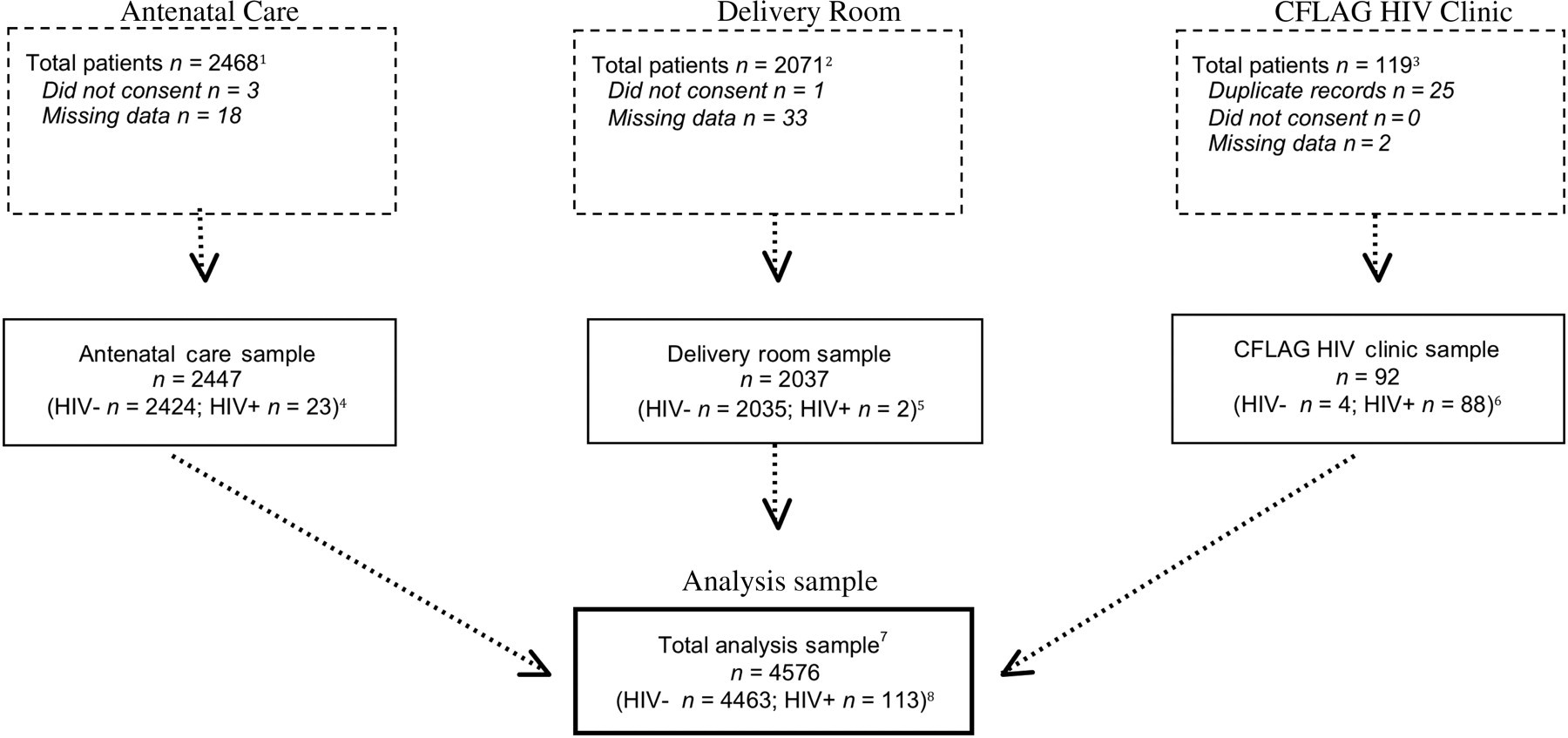
Analysis sample (n = 4576). CFLAG = Clínica Familiar Luis Ángel García; HGSJD = Hospital General San Juan de Dios; MTCT = mother-to-child transmission 1These are all pregnant women reporting to antenatal care at the HGSJD during MTCT pilot study 1 (2005-04-01 to 2005-12-01). All were eligible to participate. 2These are all pregnant women reporting to the delivery room at the HGSJD during MTCT pilot study 2 (2006-06-01 to 2006-09-30, during daytime hours only). Women reported for a variety of indications, including labour, pregnancy complications and miscarriage. All were eligible to participate. 3These are all women in care at CFLAG and pregnant between 2005 and 2007. The initial figure includes 25 HIV+ patients diagnosed in the MTCT studies. All were eligible to participate. 4Of the 23 women identified as HIV+ in antenatal care, 10 (44%) were previously aware of their HIV status; 13 (57%) were newly diagnosed cases. Crude HIV prevalence is 23/2447 = 0.93%; HIV prevalence adjusted to remove HIV cases that had been previously identified is 13/2437 = 0.53%. 5The two HIV+ women screened in the delivery room were newly diagnosed cases. HIV prevalence is 2/2037 = 0.09%. 6Of the additional 88 HIV+ women recruited from the HIV clinic, 50 (56.82%) had been previously diagnosed, 32 (36.37%) were new cases and 6 (6.82%) could not be classified. 7The total analysis sample comprises participants from antenatal care, the delivery room and the CFLAG HIV clinic. 8Of the 113 HIV+ women in the total analysis sample, 60 (54%) had been diagnosed as seropositive prior to our study. The rest were new cases (n = 47 of 113, 41.6%), or time of first diagnosis was undetermined (n = 6 of 113, 5.3%). There were no statistically significant differences between previously diagnosed and newly diagnosed patients except for a greater tendency for HIV+ patients previously aware of their serostatus to report having had a partner who is HIV+ (P ≤ 0.001)
Variables
The primary endpoint for the analysis was laboratory-confirmed HIV status. Patients were considered HIV+ based on two or more positive HIV tests, at least one of which was an enzyme-linked immunosorbent assay (ELISA) or Western blot. For the majority of patients, HIV status was initially assessed via rapid testing using the Determine HIV-1/2 (Abbott Diagnostics, North Chicago, IL, USA). Patients received guidance on HIV prevention and testing on an individual basis from trained counsellors (nurses and psychologists) prior to obtaining consent for the HIV rapid test. Counsellors returned results from the rapid test during the same hospital visit. Patients with a positive result on the initial HIV rapid test received explicit guidance about the possibility of false positives and an appointment to return for definitive results. Those with a positive test had their serostatus confirmed using ELISA, followed by Western blot in case of discrepancies or indeterminate results. Controls were run on negative tests at regular intervals to ensure diagnostic quality. Other variables reflect participant responses to interviewer-administered questionnaires collecting sociodemographic data, a detailed medical history and social and behavioural factors related to HIV risk. Data were collected by trained clinicians and analysed using Stata 10. 17
Data sources/measurement
Questions concerning domestic abuse and violence were adapted from the World Health Organization's Multicountry Study on Women's Health and Domestic Violence 18 and Guatemala's National Survey of Maternal-Child Health. 19 Participants' economic status was classified using a list of household goods taken from the National Survey of Maternal-Child Health. 19 Based on multiple correspondence analysis, we excluded one item (solar energy) from the list and summed the remaining eight to create a wealth index ranging from 0 (poorest) to 8 (best off).
Potential sources of bias
This study combines data from patients recruited from antenatal care at the HGSJD in 2005, the delivery room at the HGSJD in 2006 and the CFLAG HIV clinic (located on the premises of the HGSJD) from 2005 to 2007. Recruitment of HIV+ women from a specialized HIV clinic may be thought to introduce biases into a study of HIV risks, as HIV clinic patients might have different risk factors from those diagnosed during pregnancy.
To improve understanding of the groups in our study, we reviewed charts and traced referral patterns of all HIV+ patients. For conceptual reasons, we focused on the issue of how previously diagnosed HIV+ patients might differ from those newly diagnosed during pregnancy. We had anticipated that HIV+ cases diagnosed in antenatal care would represent new cases. We discovered, firstly, that HIV+ patients from the MTCT studies and the CFLAG clinic represented a mix of newly diagnosed and previously diagnosed patients (Figure 1). Almost half of the patients in antenatal care (44%) had originally been diagnosed elsewhere. These patients deliberately sought antenatal care at the HGSJD because HIV treatment and prevention of MTCT were largely unavailable elsewhere in Guatemala at that juncture. They did not inform study personnel of their serostatus. Secondly, about 57% of patients from CFLAG had been diagnosed elsewhere. The remainder were new patients diagnosed in the HGSJD antenatal care and delivery rooms. After the MTCT studies had officially closed, procedures and protocols were taken over by the HGSJD with funding from the Global Fund. Moreover and thirdly, that for women identified as previously diagnosed cases, no information is available on duration since diagnosis. Some were longstanding HIV patients; others were diagnosed a matter of days prior to entering into care at our study centres. Fourthly, for women identified as known cases, the sites of original diagnosis are similar regardless of centre. Initial diagnoses were most frequently made at local health centres and NGOs in Guatemala City, such as Medicos Sin Fronteras (Doctors without Borders), Aprofam, Yaloc and the Hogar Marco Antonio. Some came from outside Guatemala City, notably from the port city of Escuintla. Fifthly, we assessed differences between previously diagnosed and newly diagnosed HIV+ patients using methods to assess crude associations described below. The only statistically significant difference concerned the proportion aware of previously having had an HIV+ partner, which was higher for known HIV+ patients (P ≤ 0.001). In summary, given the information available to us, there seemed to be no sharp distinction to be made in terms of populations with distinct HIV risks, either between study sites, or between known and newly diagnosed cases. We hence analysed HIV+ patients as a single group.
Statistical methods
Crude associations were assessed using univariable logistic regression for continuous variables and the χ 2 test for categorical variables. Categorical variables with cell counts of 5 or less were examined with Fisher's exact test.
For multivariable analyses, we followed guidelines developed by Steyerberg and colleagues 20–22 for prognostic modelling using logistic regression analysis in small data-sets, defined as data-sets where the number of events per variable (EPV) is less than 10.
We selected model predictors based on risk factors for HIV described in the scientific literature. We examined bivariate relationships to HIV only to select among sociodemographic covariates, such as ethnicity or age, for which no reliable information exists in Guatemala. EPV was 10. For continuous variables, we examined the assumption of linearity in the logit using lowest smoothers, local mean regression and inspection of quartiles. We used a linear association to model the number of sexual partners, and a dichotomous variable to model age (age 18 or less, versus the rest). Regression analyses were restricted to individuals with complete data on all variables. Missing cases were infrequent (<2%) and did not depend on the value of any observable variable. 23
Regression coefficients were estimated for the full model including all predictors, independent of statistical significance. We also explored more parsimonious nested models. Comparisons between models examined the possibility of specification error resulting from omission of relevant variables, and considered the likelihood ratio test to study the enhancement to predictive ability conferred by additional variables. The Hosmer–Lemeshow goodness-of-fit statistic was used to assess model fit. 24 The tolerance test and its reciprocal variance inflation factors were used to explore the possibility of multicollinearity among model variables. 25,26 The full model was retained. Details of the modelling process and sensitivity analyses examining alternative modelling strategies based on automated selection are available from the authors.
Internal validity was assessed using bootstrapping, a resampling method that allows one to make inferences about the population from which the sample originated by drawing with replacement from the original sample. 23 The full model was fit 1000 times on a bootstrap sample equal in size to the original sample. 27
Finally, for variables of interest identified in the regression analysis, we stratified the sample and performed exploratory analyses to evaluate crude associations within strata.
RESULTS
Participants
Of the 4633 women eligible for this study, four (0.09%) did not consent to participate. An additional 53 (1.15%) were excluded due to missing data. A total of 4576 subjects (98.78% of those eligible) were included in the analysis: 113 HIV+ and 4463 HIV− women (Figure 1).
Table 1 describes characteristics of study participants. Although HIV+ women were slightly less well-off than HIV− women (mean wealth index 5.83 for HIV− women versus 5.5 for HIV+ women, P ≤ 0.05) and less likely to be 18 years or less (17.42% for HIV− versus 7.96% for HIV+ women, P ≤ 0.05), sociodemographic characteristics were similar between groups. Sexual risk behaviours and drug use were infrequent. Rates of pregnancy planning were generally low and were lower among HIV+ women (31.32% for HIV− versus 20.35% for HIV+ women, P ≤ 0.05). Partner risk behaviours and experiences of abuse were common; prevalence was higher among HIV+ women.
Characteristics of HIV+ and HIV− patients in a sample of 4576 pregnant women, Guatemala City, Guatemala 2005–2007*†
STD = sexually transmitted disease; TB = tuberculosis; IQR = interquartile range
*All figures reported as number, % unless otherwise indicated
†Statistically significant differences denoted as*P ≤ 0.05, **P ≤ 0.01, ***P ≤ 0.001
‡Ethnicity was self-identified; the rest of the sample identified as ladina (an ethnic
identity that in Guatemala is associated with a mixture of indigenous and European heritage, or simply means, ‘not indigenous’)
§Highest level of education completed
**An index of household goods ranging from 0 to 8
††Only six patients reported use of illegal drugs by injection. All were HIV negative
‡‡An affirmative answer to any of the following forms of abuse: sexual abuse up to 12 years of age; sexual abuse after 12 years of age; or verbal, physical or sexual abuse at the hands of a domestic partner during the last 12 months
§§We asked: have you ever had a partner with any of the following characteristics?
Main results
Logistic regression analysis was performed on HIV status as outcome with maternal, partner, relationship and socioeconomic predictors of risk. A test of the full model against a constant-only model was statistically significant, χ 2 (11, n = 4576) = 424.60, P ≤ 0.000, indicating that the predictor set reliably distinguished between HIV+ and HIV− women.
Table 2 presents regression results. HIV status was reliably predicted by one variable related to women's behaviour (lifetime number of sexual partners) and three predictors related to partner risks. Having a partner that was HIV+ conferred the highest additional risk (odds ratio [OR] 405.1, 95% CI: 191.9–854.9, P ≤ 0.001), followed by a partner who was a migrant worker (OR 2.015, 95% CI: 1.13–3.59, P ≤ 0.05), a woman's lifetime number of sexual partners (OR 1.186, 95% CI: 1.10–1.28, P ≤ 0.001) and a partner suspected of being unfaithful (OR 1.89, 95% CI: 1.088–3.15, P ≤ 0.05). The same factors were identified as significant risks after bootstrapping, although lifetime sexual partners decreased in significance to P ≤ 0.5.
Logistic regression model of HIV risks
CI = confidence interval; OR = odds ratio; STD = sexually transmitted disease
n = 4576
*P < 0.05, **P < 0.01, ***P < 0.001
†Coefficient and odds ratio for each five additional sexual partners beyond the mean value (1.8)
Other analyses
We performed exploratory analyses comparing the characteristics of female partners of migrant workers to those whose partners were not migrant workers (Table 3). Sexual risks were higher among partners of migrant workers, as evidenced by more lifetime sexual partners (mean 1.64 [SD 3.42] for non-migrants versus mean 2.71 [SD 9.68] for migrants, P ≤ 0.01), and more frequent exchange of sex for benefits (2.30% for non-migrants versus 4.37% for migrants, P ≤ 0.01) and sexually transmitted infections (10.66% for non-migrants versus 14.65% for migrants, P ≤ 0.01). Rates of suspected partner infidelity were considerably higher (21.88% for non-migrants versus 39.44% for migrants, P ≤ 0.001).
Selected characteristics of female partners of migrant workers (n = 4576)*†
STD = sexually transmitted diseases
*All figures reported as number, % unless otherwise indicated
†The table presents only statistically significant differences, denoted as: *P < =0.05, **P < =0.01, ***P < =0.001
‡An affirmative answer to any of the following forms of abuse: sexual abuse up to 12 years old; sexual abuse after 12 years old; or verbal, physical or sexual abuse at the hands of a domestic partner during the last 12 months
§We asked: have you ever had a partner with any of the following characteristics?
DISCUSSION
This study described risk factors for HIV infection among pregnant women in Guatemala City, Guatemala, to inform the development of locally adapted prevention strategies. Women in this sample exhibited few behavioural risks for HIV. HIV status was predicted by one variable related to women's behaviour (lifetime number of sexual partners) and three variables related to partner risks (partner HIV+ , partner migrant worker and partner suspected unfaithful). The OR for ‘partner HIV+ ’ conferred the highest additional risk; ORs for the other factors were of similar magnitude. Results were robust under diverse analytic approaches.
Strengths and limitations
Particular strengths of this study include its high acceptance rate and the completeness of information collected, enabling virtually all eligible individuals to be included in the analyses. A statistical approach well adapted to predictive modelling in data-sets with rare outcomes is also an important asset. Together, these factors contribute to internal validity of results derived from a large sample of rarely studied people.
Three important limitations merit consideration. First, with the exception of HIV status, all variables in this study reflect participant responses. Imprecise measurement of exposures is likely and would tend to result in bias towards unity (i.e. no association). True risks may therefore exceed those described in our model. Second, this analysis included previously diagnosed and newly diagnosed HIV+ patients, and combined these groups for purposes of analysis. Statistical comparisons demonstrated that known HIV+ patients were more often aware of previously having had an HIV+ partner, enhancing the importance of this variable in our data-set. Groups were found to be otherwise similar; however, it remains possible that they differ from one another in terms of variables not measured by our study. Third, while the sample size from our study was larger (and the EPV ratio higher) than previous similar studies from Latin America, 28,29 a larger sample might have permitted greater precision in the identification of risks and model specification. Risk factors identified should be taken as a minimum set.
Comparison with other studies
Although limited information on the epidemiology of HIV infection in pregnant Latin Americans has been published over the last 25 years in Lima, Peru, 28 Campinas, Brazil 30 and Tijuana, Mexico, 29 epidemiologic patterns evolve rapidly and are distinct from those found in Central America. In addition, our study had a larger sample size and more robust statistical methods than earlier published reports. The grey literature is also an important information source. A recent report identifies 10 studies describing HIV prevalence rates in specific populations of pregnant Guatemalans over the period 1998–2007, with estimates ranging from 0% to 1%. 31 No other studies documented risk factors.
Interpretation
The four predictors identified in our analysis represent important risk factors for HIV infection in this hospital-based sample of urban, pregnant Guatemalan women. The factors ‘migrant worker’ and ‘partner unfaithful’ are of particular importance epidemiologically, as they document bridging routes for sexual transmission from high-risk populations to the general population. Although mobile populations have long been suspected to contribute to HIV dissemination in the region, 32,33 this study provides the first clear evidence documenting the impact of migrant work on HIV infection in Central America. It also confirms the role of male partner infidelity as a bridge for HIV transmission to the general population, most likely from higher risk populations of male or female commercial sex workers (CSWs) to their regular female partners. 6
The definition of migrant work used in this study encompasses both internal migrants (those who migrate as seasonal labourers, most commonly on agricultural plantations in the country's southwest region) and migrants to other countries, such as Mexico and the USA. Guatemala's economy depends increasingly on remittances from the 5–10% of its population living abroad. Approximately 97% of migrants live in the USA, many in situations of economic and social vulnerability. 34 The value of remittances has grown 10-fold over the period 1997–2007 and now represents 12.7% of Guatemala's GDP, 35 exceeding the total volume of its annual exports or income from tourism. 34 Around 3.7 million Guatemalans (one third of the population) now receive remittances; 57% live in rural areas. 34 The rapid increase in migrant work associated with economic globalization thus yields new potential pathways for HIV transmission, particularly in formerly isolated rural areas.
Our results derive from a clinical sample of pregnant women in Guatemala City. Extrapolation to other groups of women in Guatemala, or in Central America, must of necessity be performed with caution. Nevertheless, risk factors identified fit plausibly with conjectures about HIV transmission in the region. 2,3 Comparisons with Guatemala's nationally representative 2002 National Survey of Mother and Child Health 19 suggest that the HIV-negative patients in our sample are likely a good reflection of sexually active women of reproductive age who use public health services in urban areas such as Guatemala City, in terms of variables such as age, education, ethnicity, civil status, parity, religion and experiences of violence and abuse. Due to the lack of previous studies of HIV+ women in Guatemala and the more complex ways in which HIV+ women entered this study, it is difficult to assess to what extent the HIV+ women in our sample represent the population of HIV+ women in Guatemala, or in Guatemala City. Additional studies and national-level HIV surveillance for the general population are needed to complete this epidemiological portrait. Information on HIV in rural areas is especially important.
Lessons for prevention
HIV prevention policy in Guatemala currently focuses on high-risk groups of MSM and FSW. In accordance with the United Nations targets of reducing the proportion of infants infected with HIV by 20% by 2005 and 50% by 2010,
36
Guatemala has also recently invested in programmes to prevent MTCT. To effectively control HIV in this low-prevalence setting, it is important to capitalize on opportunities for PMTCT programme strengthening and other strategic prevention interventions. Our results suggest four important new directions for consideration by health authorities:
Rates of pregnancy planning were generally very low in our sample, with only 31% of HIV− women (1398 of 4463) having planned their pregnancy. Rates were lower still among HIV+ women, whether newly diagnosed or known cases, of which only 20% (23 of 113) reported pregnancy planning. Pregnancy counselling for HIV+ couples can help reduce unwanted pregnancies with the possibility of transmission to the child.
37
Services must be offered in a spirit of respect for reproductive rights;
38
Regression analyses identified awareness of having had an HIV+ partner as the most important risk factor for the women in our study, affecting 54 of the 113 HIV+ women (48%). In fact, 17 of 113 HIV+ women (15%) had no other identified risks. While Guatemalan law requires HIV+ individuals to notify their partners, fear of stigma and negative repercussions upon disclosure of positive serostatus may prevent or delay HIV+ individuals from complying.
39
Establishment of a formal partner notification programme has the potential to prevent forward transmission;
40–42
Regression results identified having a partner who is a migrant worker or who is suspected unfaithful as significant predictors of positive HIV serostatus, providing evidence of two important bridging behaviours. These findings suggest that targeted educational interventions for migrant workers and their spouses, as well as for the clients of CSWs, have the potential to help to stem HIV transmission to the general population;
43
Finally, a comprehensive, multisectoral response to reduce women's vulnerability is urgently needed. Regression results show a correlation between a woman's lifetime number of sexual partners and positive HIV serostatus. In our study, while only three women identified themselves as sex workers, approximately 2% of the sample can be identified as at higher risk based on reported number of sexual partners (i.e. lying two or more standard deviations above the mean). Abuse and drug use were the variables most highly correlated with high numbers of sexual partners for women (data not shown); Links between HIV and intimate partner violence are now well established;
44,45
poverty and gender inequality play an important contributory role.
46
Gender inequality is itself now recognized as an underlying epidemic driver. Prevention interventions must recognize and tackle the complex sources of women's vulnerability if the increasing feminization of the Guatemalan HIV epidemic is to be stopped.
Footnotes
ACKNOWLEDGEMENTS
We extend our sincere thanks to Brenda Monroy, Miguel D'Avila, Tamara Velasquez, Claudia Motta, Karla Alonzo, the staff of the Clínica Familiar Luis Ángel García, the Asociación de Salud Integral and the ASI Laboratory, and the Obstetrics and Gynaecology Departments at the Hospital General San Juan de Dios, Guatemala City. We are also grateful for very helpful comments by an anonymous reviewer. Our greatest debt is to the study participants, to whom this article is dedicated. Funding for this study was provided by the Canadian Institutes for Health Research (CIHR) via Grants GLH – 63104, HPP-79623, and MPD-2008, and the Pan-American Health Organisation (PAHO)/Health Canada BPB Funds 2006–2007. Equipment and in-kind support was provided by UNICEF, the Guatemalan Ministry of Health via the National Program for HIV/ AIDS and STDs, the Global Fund for HIV/AIDS, TB and malaria (GFATM) Grant #GUA-304-G01-H, the Asociación de Salud Integral (Guatemala), Clínica Familiar Luis Ángel García (CFLAG), and the Department of Obstetrics and Gynaecology, Hospital General San Juan de Dios (HGSJD), Guatemala City. Dr Johri is a recipient of a CIHR New Investigator Award.