
Abstract
An African HIV-infected patient presented with widespread necrotic lymphadenopathy five months after starting combination antiretroviral therapy (cART) and was thought to have disseminated tuberculosis in the context of an immune reconstitution inflammatory syndrome (IRIS) on the basis of typical imaging appearances and suggestive appearances from a fine needle aspirate of a nodal mass. The patient deteriorated despite empirical antituberculosis therapy and the correct diagnosis of nodal cryptococcal infection was subsequently established by histological examination of a core biopsy from a lymph node. IRIS should be borne in mind when considering the differential diagnosis in a patient who has recently started cART.
INTRODUCTION
HIV-associated immune reconstitution inflammatory syndrome (IRIS) occurs after institution of combination antiretroviral therapy (cART) and is usually associated with latent, occult or previously treated infections, 1 including tuberculosis, Mycobacterium avium-intracellulare, 2,3 cytomegalovirus (CMV) 4 and Cryptococcus neoformans. 1,5 Several reports describe ‘typical’ imaging features of tuberculosis in patients co-infected with HIV 6,7 and in the context of IRIS. 8,9
We describe a black African HIV-infected patient who presented with widespread necrotic lymphadenopathy five months after starting cART and was thought to have disseminated tuberculosis in the context of an IRIS on the basis of typical imaging appearances and suggestive appearances from a fine needle aspirate of a nodal mass. The patient deteriorated despite empirical antituberculosis therapy and the correct diagnosis of nodal cryptococcal infection was subsequently established by histological examination of a core biopsy from a lymph node.
CASE REPORT
A 35-year-old black African woman presented with microbiologically confirmed C. neoformans meningitis (CM) at which time she was found to be HIV infected. Baseline CD4 count = 10 cells/μL and HIV viral load = 220,000 copies/mL. Following treatment of cryptococcal meningitis with intravenous liposomal amphotericin and flucytosine the patient had started maintenance fluconazole therapy and commenced cART (zidovudine/lamivudine and efavirenz). Two months later the patient presented with bilateral progressive loss of visual acuity. CMV retinitis and an associated immune reconstitution syndrome (IRIS) uveitis were diagnosed. Treatment with intravenous ganciclovir was started; at this time CD4 count = 40 cells/μL and HIV viral load = 370 copies/mL.
Five months later (7 months after the original presentation) the patient reported a four-day history of fever, night sweats, headache and general lethargy. General examination was unremarkable. The patient was initially thought to have a relapse of CM. Investigations showed C-reactive protein = 117 mg/L (n < 5.0) and a normal WBC; HIV viral load = undetectable and CD4 count = 110 cells/μL. Cranial computed tomography (CT) imaging and lumbar puncture findings were normal. Cerebro spinal fluid CrAg = negative; serum CrAg = 1:1000. CT imaging of the chest, abdomen and pelvis revealed multiple enlarged, necrotic right supra-clavicular fossa (Figure 1a), internal mammary and mediastinal lymph nodes and multiple pulmonary nodules, which were thought to represent disseminated tuberculosis. A bone marrow aspirate and trephine showed no evidence of opportunistic infection or malignancy; prolonged cultures were negative for fungi and mycobacteria.

(a) Computed tomography (CT) scan of the thorax showing a right-sided supraclavicular necrotic lymph node mass with ring-enhancement and low attenuation centres (long arrow). Additionally, there is superior mediastinal necrotic lymphadenopathy (short arrow). (b) CT scan of the thorax at the level of the aortic arch, showing posterior mediastinal necrotic lymphadenopathy (arrows) compressing the oesophagus
Analysis of a fine needle aspiration (FNA) of the right supra-clavicular node showed no acid- and alcohol-fast bacilli (AAFB) and mycobacterial culture of the FNA sample, blood, sputum and early-morning urine were negative. Cytological examination of the FNA sample showed necrotizing granulomatous inflammation; a presumptive diagnosis of disseminated tuberculosis was made. Tuberculosis treatment was started (rifampicin, isoniazid and pyrazinamide, in conventional doses).
Despite empirical antituberculosis therapy the patient remained unwell and over the next four weeks the supraclavicular lymphadenopathy progressed. In addition, the patient reported dysphagia. At this time CD4 count = 140 cells/μL and HIV viral load = undetectable. Further CT imaging confirmed widespread necrotic lymphadenopathy in the right supraclavicular fossa and throughout the mediastinum; there were necrotic nodes adjacent to the oesophagus at the level of T2/3 (Figure 1b). Additionally, there were persistent pulmonary nodules. Histological examination of an ultrasound-guided core biopsy of the supraclavicular node mass showed C. neoformans (Figure 2); culture for AAFB was negative. Retrospective staining of the supraclavicular lymph node FNA sample with Grocott methenamine silver stain revealed C. neoformans. At this time the working diagnosis of tuberculosis was changed to that of cryptococcal IRIS. Antituberculosis treatment was stopped and intravenous liposomal amphotericin was given for three weeks, followed by maintenance with oral fluconazole. Seven months later, the patient remains well, with CD4 = 120 cells/μL and HIV load = undetectable, on cART.
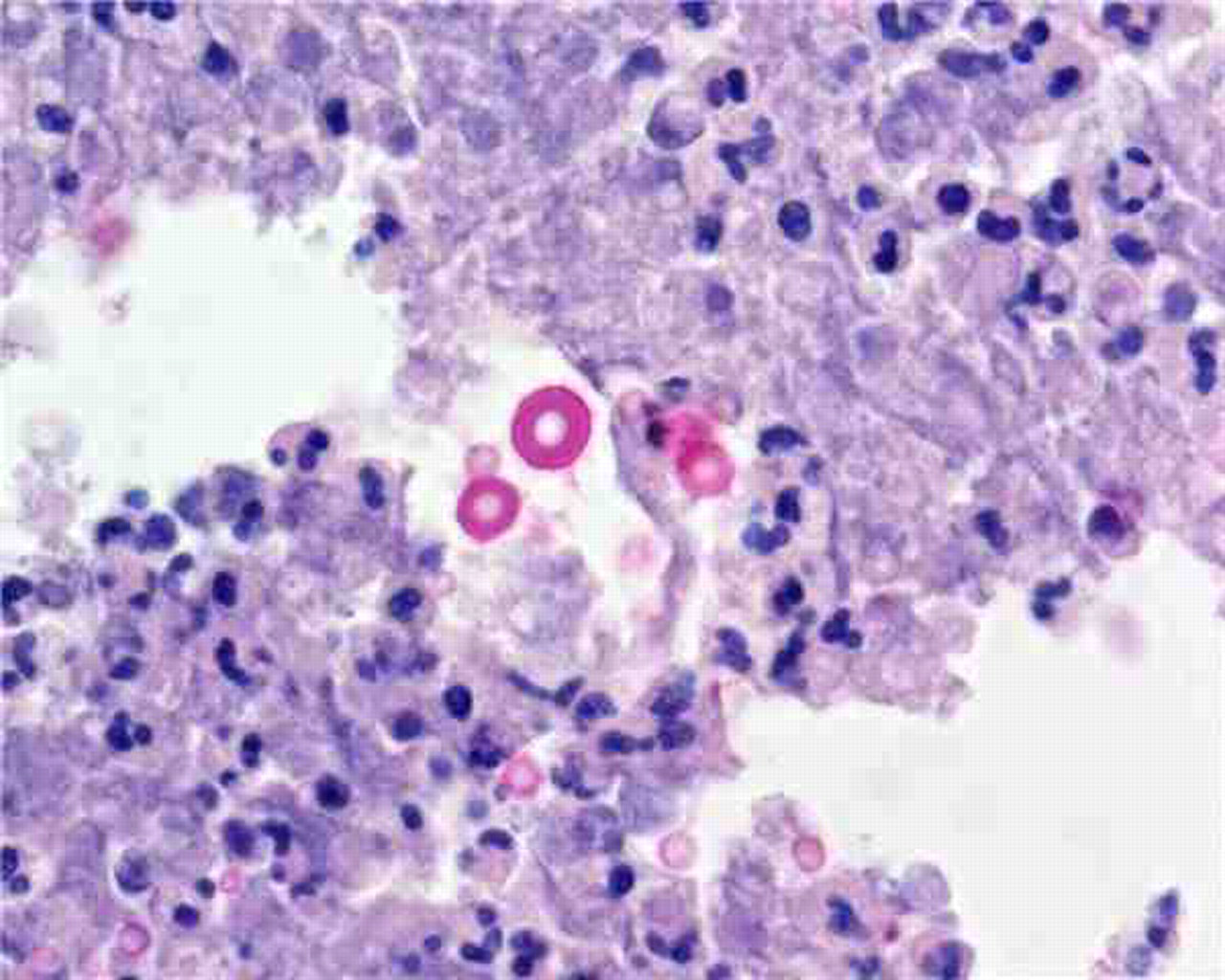
Lymph node core biopsy showing numerous Cryptococci. Mucicarmine stain; ×20 magnification
DISCUSSION
This patient was initially thought to have disseminated tuberculosis in the context of IRIS, the diagnosis being made on the basis of typical imaging appearances, 6–8 the time course in the context of starting cART and strongly suggestive cytopathological findings from FNA cytological analysis. The patient's subsequent clinical progression, despite empirical antituberculosis therapy, led to further investigation and the correct diagnosis being made.
The case described here, although not unique, 9,10 has importance for clinicians and pathologists involved in care of immunosuppressed HIV-infected patients. First, it illustrates the importance of clinicians discussing a patient's clinical presentation with histopathologists so that appropriate investigations, including use of special stains, are performed; in this case retrospective review of FNA cytology showed C. neoformans. Second, it reminds both clinicians and pathologists that although tuberculosis is the most likely explanation for necrotizing granulomata in this patient population other diagnoses should be considered. Third, it underscores the importance of clinico-pathological review, when a patient's clinical course is at variance with their pathological diagnosis.