
Abstract
We reviewed our practice in order to determine the optimum neuroimaging strategy for HIV-infected patients with acute neurological presentations between April 2007 and August 2008. Overall magnetic resonance imaging (MRI) detected cranial abnormalities in more than twice as many patients as did computed tomography (CT) (74% and 32%, n = 54 and 38, respectively). Replacement of CT by first-line MRI for all patients would have required an additional 16 MRI scans, although at a saving of 38 CT scans. Our study highlights the importance of first-line MRI brain imaging in HIV patients with neurological symptoms and reinforces the need for early transfer of patients from centres that do not have rapid access to (or expert interpretation of) MRI scanning, to an appropriate HIV specialist centre.
INTRODUCTION
Human immunodeficiency virus (HIV) is responsible for a variety of neurological complications, either as a primary effect of the virus itself or as a consequence of secondary immunosuppression. 1,2 The prevalence of neurological symptoms in HIV patients has been estimated at around 40%. 3 However, the neuroepidemiology of HIV disease may be changing, with an existing cohort of mainly older men who have sex with other men receiving long-term highly active antiretroviral therapy (HAART) 4 and, increasingly, a new cohort of patients from sub-Saharan Africa who typically present late with low CD4 count and advanced disease. 5
Two neuroimaging modalities are routinely used to investigate HIV patients presenting with neurological symptoms: computed tomography (CT) and magnetic resonance imaging (MRI). CT is widely available, quick and cheap to perform, but the downside for the patient is radiation exposure. By contrast, MRI is not as widely available and is more expensive to run. However, MRI is widely recognized to be considerably more sensitive than CT for detecting the wide spectrum of neurological disease seen during HIV infection. 3,6,7 Given these changing patterns of clinical presentation of neurological disease, we performed a retrospective case series review of our practice in order to determine the optimum neuroimaging strategy for HIV-infected patients with acute neurological presentations.
METHODS
Data were collected on all patients who had neuroimaging during their admission to University College London Hospital's HIV inpatient facility between April 2007 and August 2008. Demographic (age, gender, duration of admission), laboratory (CD4 count, HIV-1 RNA viral load) and radiology data (formal imaging reports) were collated from the hospital online clinical data repository, the radiology picture archiving and communication system and patient notes/discharge summaries, where appropriate. Presenting symptoms were classified into focal or non-focal neurology and radiology reports were classified as normal (no changes other than HIV-related atrophy) or abnormal (all other findings). In patients who had both CT and MRI imaging during their admission, the radiological findings were compared.
RESULTS
Over the period of the study, 66 patients (Table 1) presented on 68 occasions and underwent 92 episodes of neuroimaging, of which 38 (41%) were brain CT and 54 (59%) brain MRI. The most common focal neurological presentations included hemiparesis, cerebellar dysfunction or cranial nerve palsy. Headache, progressive cognitive impairment or altered mental status were among the most common non-focal presentations. A cohort of patients (n = 22) received an initial CT scan followed by MRI (median interval between scans = 4 days). An example of the different imaging findings on CT and MRI in the same patient is shown (Figures 1a and b).
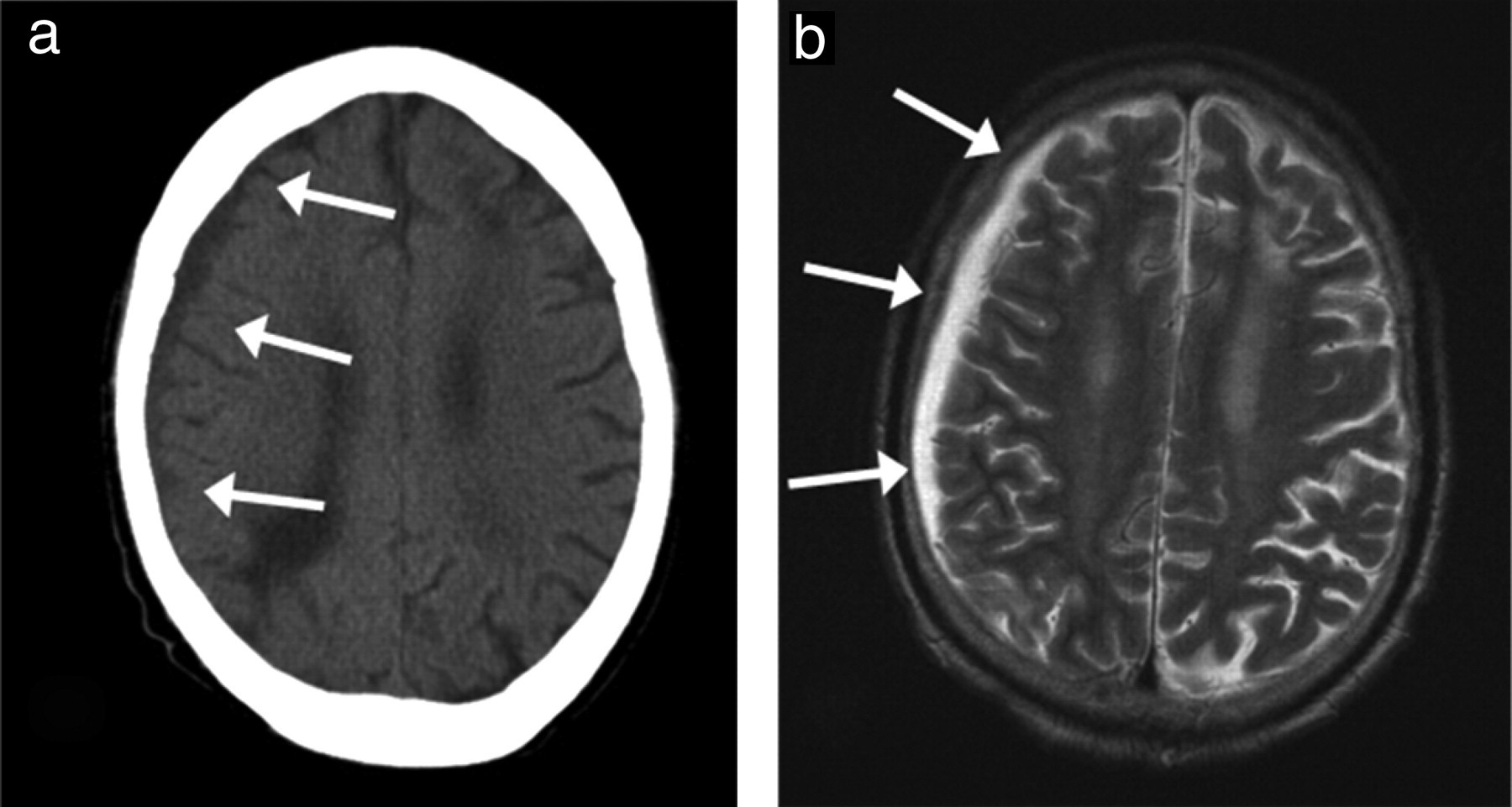
(a and b) Representative images taken from a patient who presented with a CD4 count >200 and a one-week history of headache and cerebellar signs with a left third cranial nerve palsy are shown. Panel (a) shows a transverse computed tomography section taken on the day of admission which was reported as showing a chronic subdural haemorrhage (white arrows). With continuing symptoms, a magnetic resonance imaging (MRI) was performed two days later. Panel (b) shows a T2-weighted MRI scan, showing pathological enhancement and nodularity (white arrows), the report suggested tuberculosis meningitis as a likely cause, a diagnosis subsequently confirmed by lumbar puncture
Demographic data for patients included in this study
There were no significant differences between the cohort presenting with focal neurology and those with non-focal presentations. IQR = interquartile range; HAART = highly active antiretroviral therapy
*Two patients were admitted on two separate occasions
In patients who had first-line MRI (Figure 2a), the abnormality detection rate was similar for focal and non-focal neurological presentations being 73% and 75% (n = 15 and 16, respectively). The most common reported findings were white matter hyperintensities, features suggestive of viral encephalitis and evidence of stroke. Overall MRI detected intracranial abnormalities in more than twice as many patients as did CT (74% and 32%, n = 54 and 38, respectively). Among patients who had first-line CT (Figure 2a), 11/12 (92%) of patients who had an abnormal scan subsequently had an MRI (including five patients where MRI was specifically recommended on the CT scan report). MRI altered the CT findings in 7/11 (63%) of cases, including the case shown in Figures 1a and b and other cases where MRI corrected the CT diagnosis from toxoplasmosis to a glioma and from medullary infarct to encephalitis. By contrast, 11/26 (42%) of patients who had a normal CT scan report also underwent MRI brain imaging; abnormalities were found in 5/11 (45%) of cases including cases with a final diagnosis of viral meningitis, HIV-related encephalopathy and HIV-associated small vessel disease.
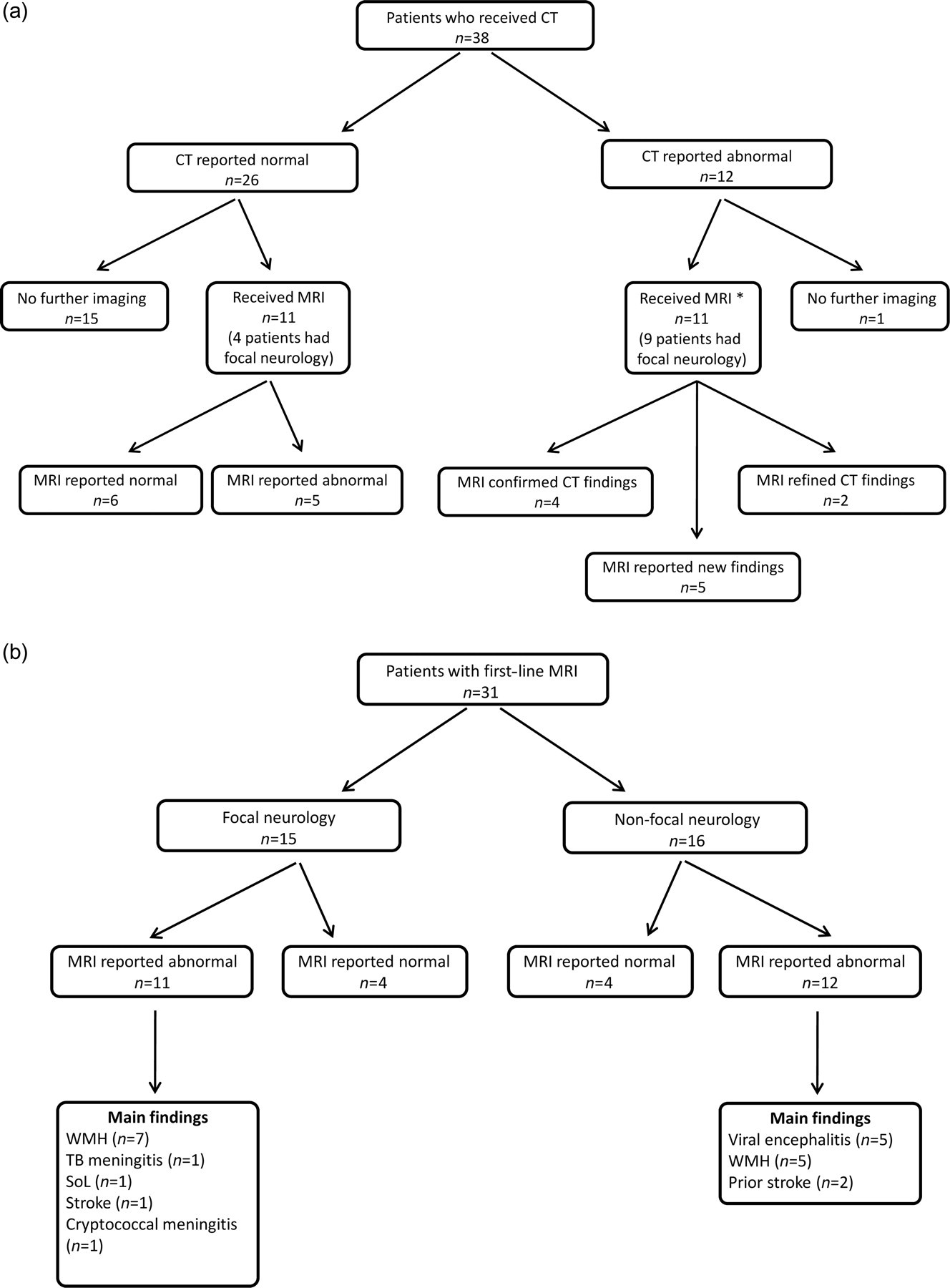
Flow charts showing how patients were imaged by neurological presentation for magnetic resonance imaging (MRI) (a) and by classification of the computed tomography (CT) report for patients undergoing first-line CT (b). WMH = white matter hyperintensities, SoL = space-occupying lesion, TB = tuberculosis. *MRI recommended on the CT report in five cases
The most common abnormal MRI findings in general were white matter hyperintensities, which were reported on a total of 16 MRI scans. The median age of patients with white matter change was 47.5 years (interquartile range = 44.5–50.25). Nine of these 16 patients presented with focal neurology and nine were receiving HAART. In the majority of these cases, the white matter changes were regarded as being due to underlying small vessel disease. A further nine patients had diagnoses of viral encephalitis or encephalopathy; several had lumbar puncture which confirmed the presence of viral nucleic acid (including HIV) in the cerebrospinal fluid.
In this cohort, replacement of CT by first-line MRI for all patients would have required an additional 16 MRI scans, although at a saving of 38 CT scans.
DISCUSSION
The results of this case review show that the majority of patients who presented to our centre with neurological symptoms required MRI brain scanning to achieve a diagnosis, even if on the current admission they underwent CT scanning. MRI provided an enhanced diagnostic yield, irrespective of clinical presentation, or level of immunosuppression.
This study shows that MRI imaging in HIV-infected patients provides additional useful clinical information compared with CT scanning and we would advocate that where possible, an MRI should be chosen in preference to a CT scan in order to avoid duplication of expensive tests and avoid patients being exposed to unnecessary radiation. Currently, few units have 24-hour urgent access to MRI scanning, but results from our study suggest that such provision could be beneficial.
MRI is also more likely to provide the best image both for diagnosis and for future comparison, if needed. MRI detected white matter changes (which may precede neurological sequelae such as stroke) 8 and viral encephalopathy in a number of patients with normal CT scans. While the immediate clinical significance of these white matter changes in patients with HIV is controversial, a recent review 9 of clinical research data underlines the wide-ranging effects of HIV infection on neurophysiology, ranging from cognitive functioning to cellular metabolic regulation.
Taken together, our study highlights the importance of first-line MRI brain imaging in HIV patients with neurological symptoms and reinforces the need for early transfer of patients from centres that do not have rapid access to (or expert interpretation of) MRI scanning, to an appropriate HIV specialist centre, which in accordance with British HIV Association guidelines for patients presenting with neurological symptoms. 10
Footnotes
ACKNOWLEDGEMENTS
We thank Fiona Henderson, Lead Superintendent Radiographer, University College London Hospitals, for help with data ascertainment. AJW was awarded the 2009 British Association for Sexual Health and HIV (BASHH) Undergraduate Medical Student Prize for this project.