
Abstract
Stigma towards people living with HIV is pervasive in China and related to poor service utilization, psychosocial distress and diminished quality of life (QOL). In an effort to identify mechanisms to reduce HIV stigma and its negative consequences, we examined whether social support mediates the relation between enacted stigma and both depressive symptoms and QOL among 120 HIV outpatients in Beijing, China. Generally, perceived social support was associated with less stigma, less depressive symptomatology and better QOL. Using multivariable regression models, we found that social support was a full mediator of the impact of stigma on both depressive symptomatology and QOL. The findings suggest social support may be an important target of interventions to reduce the impact of stigma on poor psychosocial health outcomes.
Introduction
Although the prevalence of HIV among people aged 15–49 years in China is still relatively low (0.1%) compared with in the USA (0.6%)/HIV stigma is already deeply entrenched within Chinese communities. 2 In China, areas with high rates of intravenous drug use or commercial blood donation have contributed to the characterization of HIV as a disease of the ‘immoral’ and the poor. 3 As a result, people living with HIV (PLWH) in China often experience a loss of ‘face’, which can lead to diminished value in society and ability to negotiate social networks. 4
Internalized stigma, defined as negative attitudes held by individuals about their own condition, has been associated with poor health outcomes. 5 Once a person with HIV internalizes stigmatizing public attitudes, she/he may begin to feel depressed, symptoms of which are frequently reported by PLWH in China. 6 In addition, HIV stigma has strong negative associations with quality of life (QOL), comprising a person's physical, functional, emotional and social functionality. 7 Furthermore, stigma has been associated with poor medication adherence, contributing to poor morbidity and increased mortality for PLWH. 8
Given the far-reaching impact of HIV stigma, we set out to examine factors with the potential to lessen negative consequences of stigma. Our previous research connected social support with decreased depressive symptomatology among PLWH in New York. 9 In China, high levels of support have been associated with better QOL. 10 These findings led us to hypothesize that social support might be an effective mechanism to reduce depression and improve QOL. Thus, we examined whether social support mediated the relationship between stigma and depressive symptoms/overall QOL among PLWH in China.
Methods
Procedures
This present study was part of a larger project examining a three-session nurse-delivered HIV medication adherence intervention in China. 11 A report on the effectiveness of this intervention is published elsewhere. 12 In the present report, we focused on baseline data obtained. Participants were PLWH who received care at Ditan Hospital, a facility specializing in infectious diseases in Beijing, China. Data were collected between December 2006 and April 2008. The study was reviewed and approved by the Institutional Review Boards from our institutions and the China Centers for Disease Control.
Eligible participants were HIV-positive Mandarin-speaking adults (at least 18 years of age). Participants who were cognitively impaired or actively psychotic were excluded. Participants were recruited from the AIDS clinic or from a hospital-based HIV/AIDS support group. Interviews were conducted after written informed consent was obtained, and participants were paid the equivalent of US$15.
Measures
Sociodemographic variables. We assessed participants’ age, gender, marital/partner status, highest grade of school completed, income and employment status.
Stigma. Stigma was assessed using a modified version of the HIV Stigma Scale. 13 In order to reduce patient burden, participants completed an abbreviated version of the original scale. Five items from the personalized stigma subscale were examined, with higher values indicating greater stigma. We conducted an exploratory principal components analyses for the five items, resulting in a one-factor structure that explained 61.4% of the variance with all factor loadings greater than 0.71. Internal consistency reliability was 0.84.
Depressive symptoms. The Centers for Epidemiological Studies Depression scale (CES-D) is a screening measure used to examine the prevalence of psychological distress in community samples. 14 We used the previously validated, shortened Chinese version of the CES-D.15,16 Total scores ranged from 0 to 30, with scores of 10 or above defining possible clinical depression. 17 Cronbach's alpha for the 10-item scale was 0.77.
Quality of life (QOL). The Medical Outcomes Study-HIV (MOS-HIV) health survey 18 consists of 35 questions, and has been used to measure overall QOL of persons with HIV across the globe.19–21 To score the MOS-HIV, the raw item scores of each subscale are summed and transformed into a 0–100 scale. Higher scores indicated better health.
Social support. The Chinese version of the Medical Outcomes Study-Social Support Survey (MOS-SSS-C) is a psychometrically sound measure of perceived social support for people with chronic diseases. 22 We used the 19-item survey in our study, and total scores on the scale were derived by summing the scores for all 19 items.
Data analysis
We first examined bivariate relationships between variables of interest through calculation of correlation coefficients using list-wise deletion of cases with missing data. For mediation analyses, our small sample size prompted us to follow Baron and Kenny's stepwise guidelines on investigating mediation through regression analysis. 23 We first tested whether social support mediated the impact of stigma on depressive symptoms, and then tested whether social support mediated between the impact of stigma on QOL. Each analysis involved three steps.
In Step A, social support was regressed onto stigma. In Step B, depressive symptomatology was regressed onto stigma. In Step C, we tested for formal mediation by conducting multiple regression in which depressive symptomatology was regressed onto both stigma and social support. In step C, the standardized beta weight for stigma must be less than it is in the Step B, indicating that social support is explaining some of the relationship between stigma and depressive symptoms. We then repeated this process, examining QOL scores instead of depressive symptomatology.
Results
Participants
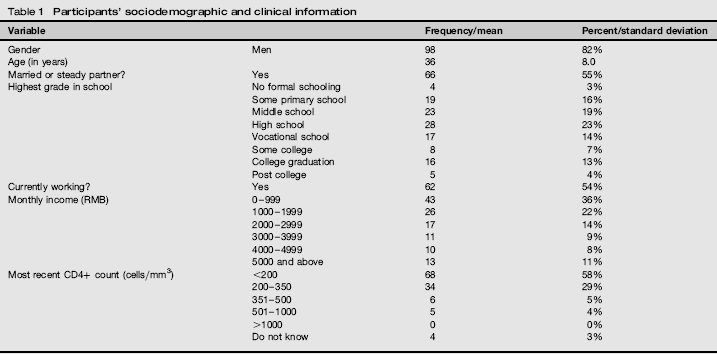
One hundred and twenty participants completed baseline assessments, with 82% men and a mean age of 36 years (SD = 8.0). Full sociodemographic and clinical information are presented in Table 1. Sixty percent of participants were on an antiretroviral therapy combination of stavudine, lamivudine and nevirapine.
Participants’ sociodemographic and clinical information
Descriptive and correlational data
The mean stigma total score was 7.6 (SD = 3.0) with scores ranging from 0 to 15, and the mean QOL score was 48.7 (SD = 23.3) with scores ranging from 0 to 100. The mean CES-D total score was 10.1 (SD = 5.8) with scores ranging from 0 to 22. Forty-nine percent of participants scored 10 or above, indicating possible clinical depression. Finally, the mean Social Support total score was 46.7 (SD = 17.0), and scores ranged from 13.2 to 100.0.
The main variables of stigma, QOL and depressive symptomatology were associated with several sociodemographic variables (see Table 2). Specifically, participants who reported experiencing more stigma were older in age (r = 0.41, P < 0.01), reported less education (r = -0.23, P < 0.05) and lower income (r = –0.23, P < 0.05). Participants reported higher mean levels of stigma and depression if they were not currently employed (t = 3.59, P < 0.001; t = 2.51, P < 0.05). Participants who reported a better QOL had more education (r = 0.25, P < 0.05) and higher income (r = 0.26, P < 0.05), and those who had lower mean levels of QOL were not currently employed (t = 0.37, P < 0.001). Participants who reported a higher mean level of social support had a steady partner (t = –3.24, P < 0.01). Social support was significantly associated with less stigma (r = –0.26, P < 0.01), less depressive symptomatology (r = –0.28, P < 0.01) and better QOL (r = 0.30, P < 0.01).
Correlations between the sociodemographic, stigma, depression and quality-of-life measures
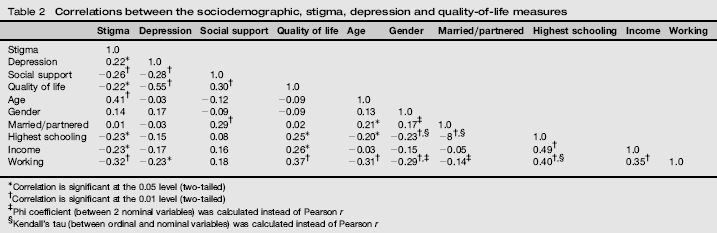
Correlation is significant at the 0.05 level (two-tailed)
Correlation is significant at the 0.01 level (two-tailed)
Phi coefficient (between 2 nominal variables) was calculated instead of Pearson r
Kendall's tau (between ordinal and nominal variables) was calculated instead of Pearson r
Mediation analyses. Using the Baron and Kenny technique, we found that stigma was associated with both social support (b = -0.26, P < 0.01) and depressive symptoms (b = 0.22, P < 0.05). With both stigma and social support in the model with depressive symptomatology, the beta for social support remained significant (b = –0.23, P < 0.05), but stigma became non-significant (b = 0.16, P = 0.09), suggesting full mediation (Figure 1a).
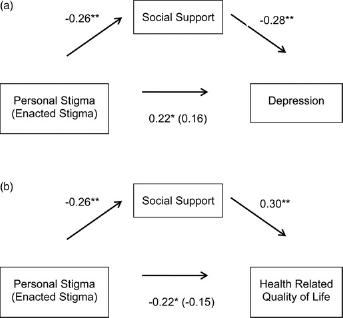
Mediation analyses among social support, stigma, and depression, (a) The standardized beta weights of each variable in the series of regression analyses are shown: *P < 0.05, ∗∗P < 0.01. (b) The standardized beta weights of each variable in the series of regression analyses are shown: *P < 0.05, ∗∗P < 0.01
Parallel analyses with QOL indicated stigma significantly predicted social support and QOL (b = -0.22, P < 0.05). When both social and stigma were included in the same model, social support remained a significant predictor of QOL (b = 0.25, P < 0.05) but stigma became non-significant (b = –0.15, P = 0.15), again suggesting full mediation (Figure 1b).
Discussion
In this study, we examined whether social support mediates the relationship between stigma, depressive symptoms and QOL among Chinese outpatients living with HIV. Consistent with previous studies, we found high levels of stigma, associated with depressive symptoms and poorer QOL.
Surprisingly, 49% of participants met screening criteria for depression in the present study. Studies in the USA have put the prevalence of major depression among PLWH at 36%. 24 The high rate of depressive symptoms among Chinese PLWH may be connected with stigma, more advanced HIV infection, or Chinese people might be more likely to endorse severe symptoms on the CES-D despite the measure's validation in China. Regardless of the cause, the high rate of depressive symptomatology clearly indicates the need for intervention.
Our results indicated that social support mediated the association between stigma and depressive symptoms/QOL. Previous studies have linked social support with stigma and depression/QOL separately in the USA and China, 9 but the present study brings these three factors together to suggest that social support may be a critical factor that can mitigate these psychosocial consequences.
Given the collectivistic nature of Chinese society, social support plays a central role, forming the structure for social support and help to occur. 25 Therefore, stigmas can be particularly problematic within Chinese culture that is oriented towards collectivism, where individuals subordinate their own interests to those of others, whose evaluations are of utmost importance. 4 As such, the availability of social support must be considered in HIV intervention development. 26
There are some limitations to note in this study. First, the relatively small sample size limited our ability to use more powerful statistical techniques, such as structural equation modelling. Second, the survey relied on interviews for data collection, increasing the likelihood for social desirability bias. Finally, causal inferences should be drawn cautiously, given the cross-sectional nature of the data.
Conclusion
Consistent with an ecological framework, our results suggest that treatment programmes should consider interactions between factors at the intrapersonal (e.g. depression, stigma) and interpersonal (i.e. social support) levels. Furthermore, these findings suggest that social support would be a critical component to stigma reduction interventions for PLWH. Multilevel methods that incorporate individual and societal level approaches are likely to yield more effective, longer lasting stigma reduction.
Footnotes
Acknowledgements
We gratefully acknowledge the providers and participants at Ditan hospital, and Bu Huang, Cheng-Shi Shiu, Wei Qu and Xin Wang for their assistance with the project. This research was supported by the National Institute of Mental Health (K23 MH 084551 PI: DR; R34 MH 074364 and R34-MH074364-S1 PI: JMS).