
Abstract
Summary
We reviewed microscopy results for symptomatic male patients in order to identify clinical correlates of urethritis as diagnosed by same-day microscopy. Higher polymorph counts were found in patients presenting with discharge, or discharge together with dysuria, but dysuria without discharge was strongly associated with negative urethral microscopy. Symptoms were strongly linked to microscopy outcome but partnerships were not linked to either symptoms or outcome.
Introduction
With the current pressure to increase efficiency and reduce costs in the National Health Service (NHS), there is further need to review established practice in the management of symptomatic patients attending sexual health services. The current national screening and testing guidelines no longer recommend that a Gram-stained male urethral smear is performed in asymptomatic men 1 but the guidance on indications for urethral smear in symptomatic men is less clear.
Methods
We aimed to establish indications for urethral smear and factors associated with negative urethral microscopy.
All symptomatic men attending a single inner-London sexual health clinic who had microscopy of a urethral smear performed during 5 March 2009-5 May 2009 were included. The local clinic protocol recommends urethral microscopy for patients complaining of urethral discharge, dysuria, penile irritation and/or testicular pain. Men with negative same-day microscopy were defined as having less than five polymorphonuclear cells per high-power field (PMN/hpf) and were referred to as the 0 polys group; they were compared with those with greater than 20 PMN/hpf (20+ polys group) with regard to age, presenting symptoms, number and type of partnerships, past history of sexually transmitted infections (STIs) and outcome of Chlamydia trachomatis nucleic acid amplification test (CT NAAT) and Neisseria gonorrhoea culture (GC) results. Patients with 5-20 PMN/hpf were excluded from the analysis in order to minimize intra- and inter-observer microscopy biases. 2
Results
Of the 323 men who had urethral microscopy performed (93% heterosexual), 120 men were eligible for our audit, with 44 patients (14%) in the 20+ polys group and 76 (24%) in the 0 polys group.
Men in the 20+ polys group were younger than those in 0 polys group and significantly more likely to present with discharge or discharge and dysuria Table 1). Patients presenting with dysuria represented 44% of patients in the 0 polys group and 14% in the 20+ polys group. 85% (34/40) of patients presenting with dysuria alone in both groups had negative same-day urethral microscopy.
Distribution of symptoms, partnerships and past sexual history data in the 0 polys and 20+ polys groups
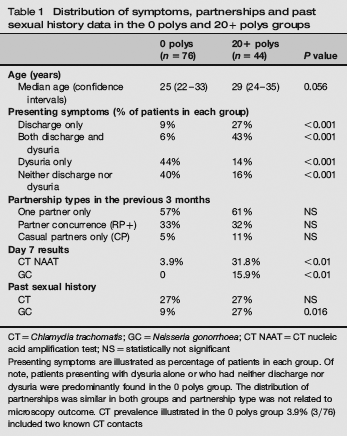
CT = Chlamydia trachomatis; GC = Neisseria gonorrhoea; CT NAAT = CT nucleic acid amplification test; NS = statistically not significant
Presenting symptoms are illustrated as percentage of patients in each group. Of note, patients presenting with dysuria alone or who had neither discharge nor dysuria were predominantly found in the 0 polys group. The distribution of partnerships was similar in both groups and partnership type was not related to microscopy outcome. CT prevalence illustrated in the 0 polys group 3.9% (3/76) included two known CT contacts
Approximately, one quarter of patients classed as ‘symptomatic’ in both groups (21/76 in 0 polys and 11/44 in 20 polys group) had microscopy performed for penile rashes, soreness, pruritus or ‘irritation’. None of them were found to have CT or GC in the 0 polys group and only one (1/44) had CT in the 20+ polys group.
There were no significant differences in the distribution of partnerships in the two groups (Table 1), with one third of patients reporting partner concurrence (defined as one regular partner together with one or more regular and/or casual sexual partners in the past three months, referred to as RP+). Relatively more men in the 20+ polys group had two or more partners (43% versus 38%, P = 0.53, non-significant). Multivariate logistic regression analysis shows no link between type of partnerships (see Table 1), symptoms and outcome, defined as positive microscopy. After adjusting for partnership type, symptoms are still significantly linked to outcome.
Three of 76 patients in the 0 polys group were subsequently found to be CT NAAT positive (but 2 out of 3 had presented as CT contacts) and none of them were GC-positive (Table 1).
Discussion
As expected, patients with positive microscopy results tended to be younger and more likely to complain of discharge or discharge and dysuria. Patients complaining of dysuria alone or having neither discharge nor dysuria were predominantly found in the negative microscopy group. This may be an apparent contrast to a previous study, 3 where dysuria was found to be as predictive as age for a subsequent diagnosis of CT, but the study 3 had been undertaken in a cohort of largely asymptomatic patients. A further study in HIV-1-positive men also did not find an association between dysuria and subsequent CT diagnosis, 4 but similar to Haddow et al. 3 confirm the association between higher polymorph counts and subsequent CT diagnosis. The prevalence of CT in symptomatic men with negative same-day urethral microscopy (excluding known CT contacts) is low (1.3%), suggesting that antibiotic treatment on the basis of symptoms alone is not warranted in this group.
Conclusions
Discharge or dysuria together with discharge but not dysuria alone were linked to high polymorph counts on same-day microscopy in male patients and number and type of partnership were not.
Urethral microscopy performed for men presenting with dysuria but without discharge or with penile skin conditions held little diagnostic benefit, both aetiologically and to identify high risk of STIs, and its indication should be carefully considered in a drive to increase efficiency.
Footnotes
Acknowledgements
We would like to thank Andrew Copas PhD for help with the statistical analysis of these data.