
Abstract
The need for viral load (VL) monitoring of HIV patients receiving antiretroviral therapy (ART) in resource-limited settings (RLS) has become apparent with studies showing the limitations of immunological monitoring. We compared the Abbott m2000 Real-Time (Abbott) HIV-1 assay with the Roche AMPLICOR Monitor v1.5 (Roche) HIV-1 assay over a range of VL concentrations. Three hundred and eleven plasma samples were tested, including 164 samples from patients on ART ≥ six months and 147 from ART-naïve patients. The Roche assay detected ≥400 copies/mL in 158 (50.8%) samples. Of these, Abbott produced 145 (91.8%) detectable results ≥400 copies/mL; 13 (8.2%) samples produced discrepant results. Concordance between the assays for detecting HIV-1 RNA ≥400 copies/mL was 95.8% (298/311). The sensitivity, specificity, positive predictive value and negative predictive value of Abbott to detect HIV-1 RNA ≥400 copies/mL were 91.8%, 100%, 100% and 92.2%, respectively. For the 151 samples with HIV-1 RNA ≥400 copies/mL for both assays, a good linear correlation was found (r = 0.81, P < 0.0001; mean difference, 0.05). The limits of agreement were −0.97 and 1.07 log10 copies/mL (mean ± 2 SD). The Abbott assay performed well in our setting, offering an alternative methodology for HIV-1 VL for laboratories with realtime polymerase chain reaction (PCR) capacity.
Keywords
INTRODUCTION
HIV viral load (VL) assays are a valuable tool in the management of HIV/AIDS patients worldwide and are necessary alongside other clinical and immunological markers in monitoring for therapeutic response to antiretroviral therapy (ART). Several studies have shown the limitations of immunological monitoring. 1–5 There is an urgent need to adopt inexpensive, reliable and accurate VL assays, which are easy to perform and use in resource-limited settings (RLS), which are also the most impacted by the HIV/AIDS epidemic. Several VL assays have been developed and marketed with some data suggesting that in areas of non-subtype B infection, the Abbott assay is superior to Roche. 6 Realtime polymerase chain reaction (PCR) offers potential advantages of efficient sample processing, improved sensitivity, increased dynamic range and reduced contamination risk over conventional endpoint PCR in the determination of plasma VL. Due to the variability in the different assays and biological differences in the various geographical areas in the world, this correlation study compared the Abbott m2000 Real-Time HIV-1 (Abbott) assay with the conventional Roche AMPLICOR Monitor v1.5 HIV-1 (Roche) assay in the Ugandan population.
MATERIALS AND METHODS
VL tests were performed on 311 plasma specimens from consenting HIV-1-infected patients in the Rakai Community Cohort of the Rakai Health Sciences Program, Uganda. All activities were approved by the US Western Institutional Review Board and the Uganda Virus Research Institute Science and Ethics Committee. The tests were performed using the Abbott assay as the test method and the ‘gold-standard’ Roche assay as the reference method. The samples were collected from HIV-1-infected patients who attend the ART clinic on a monthly basis. Whole blood was collected into EDTA Vacutainer tubes (K3 EDTA Vacutainers; Becton, Dickinson and Company, Franklin Lakes, NJ, USA) and transported to the laboratory where the plasma was separated from the cells and two separate aliquots of 600 and 200 µL were put aside for the Abbott and the Roche assays, respectively, and stored at −20°C until testing. A total of 147 samples were obtained from pre-ART HIV patients at the screening stage, while the other 164 were obtained from patients who had been receiving ART for more than six months. Linear regression analysis was used to determine the relationship between VL assay results (Figure 1). A Bland–Altman plot was used to graphically display the level of agreement between the two assays (Figure 2).
All assays were performed by trained technicians. The laboratory has participated in the Virology Quality Assessment Program based at Rush Presbyterian-St Lukes Medical Center in Chicago, IL, USA for the past four years and has remained consistently certified during this period. The Roche AMPLICOR Monitor v1.5 HIV-1 assay (Roche, Indianapolis, IN, USA) with manual extraction was performed as per the manufacturer's instructions. The lower limit of detection (LLD) was 400 copies/mL. The Abbott m2000 system extraction kits (Promega Corporation, Madison, WI, USA) were used for the manual extraction of RNA from the specimens and controls as per the manufacturer's instructions. The Abbott m2000rt Real-Time instrument was used according to the instructions for automated amplification, detection and quantitation of target HIV-1 virus in the samples and controls. The LLD for the Abbott assay was 40 copies/mL, but the results were coded as <400 or ≥400 copies/mL in order to make descriptive comparisons to the Roche test results.
RESULTS
A total of 311 plasma samples were tested with both assays including 164 samples from patients on ART for at least six months, and 147 from patients prior to initiation of ART. The Roche assay detected virus ≥400 copies/mL in 158 (50.8%) samples (Table 1). Of these, Abbott produced 145 (91.8%) detectable results ≥400 copies/mL; 13 (8.2%) samples produced discrepant results. For seven discrepant responses, the Abbott result was below the LLD (BLLD), whereas the Roche result was quantifiable between 422 and 972 copies/mL; for the remaining six discrepant responses, the Abbott result was quantifiable but <400 copies/mL (range 41–311), whereas the Roche result was quantifiable between 506 and 2146 copies/mL. Note that for 20 (6.4%) samples, the Roche result was BLLD but the Abbott result indicated detectable virus with results in the range 46–173 copies/mL. The overall concordance between the two assays for detecting HIV-1 RNA ≥400 copies/mL was 95.8% (298/311). The sensitivity, specificity, positive predictive value and negative predictive value of Abbott to detect HIV-1 RNA ≥400 copies/mL were: 91.8%, 100%, 100% and 92.2%, respectively.
Descriptive results: detection of HIV-1 RNA
Results for the 151 samples with quantifiable VLs within the dynamic range of both assays were used in the quantitative analysis. Good linear correlation was found between the two assays (Figure 1; correlation coefficient, r = 0.81, P < 0.0001; mean difference, 0.05). Results for the Abbott method ranged between 1.61 and 6.36 log10 copies/mL, and for the Roche method between 2.70 and 6.29 log10 copies/mL. According to the Bland–Altman model (Figure 2), the limits of agreement were −0.97 and 1.07 log10 copies/mL (mean ± 2 standard deviations). The differences for 140 samples (92.7%) were within the levels of agreement, while the differences for 11 (7.3%) samples were beyond the levels of agreement. Abbott results were lower than Roche for five samples, and four of these samples had Abbott results within the 41–311 copies/mL range. These results indicate good agreement between the two assays.
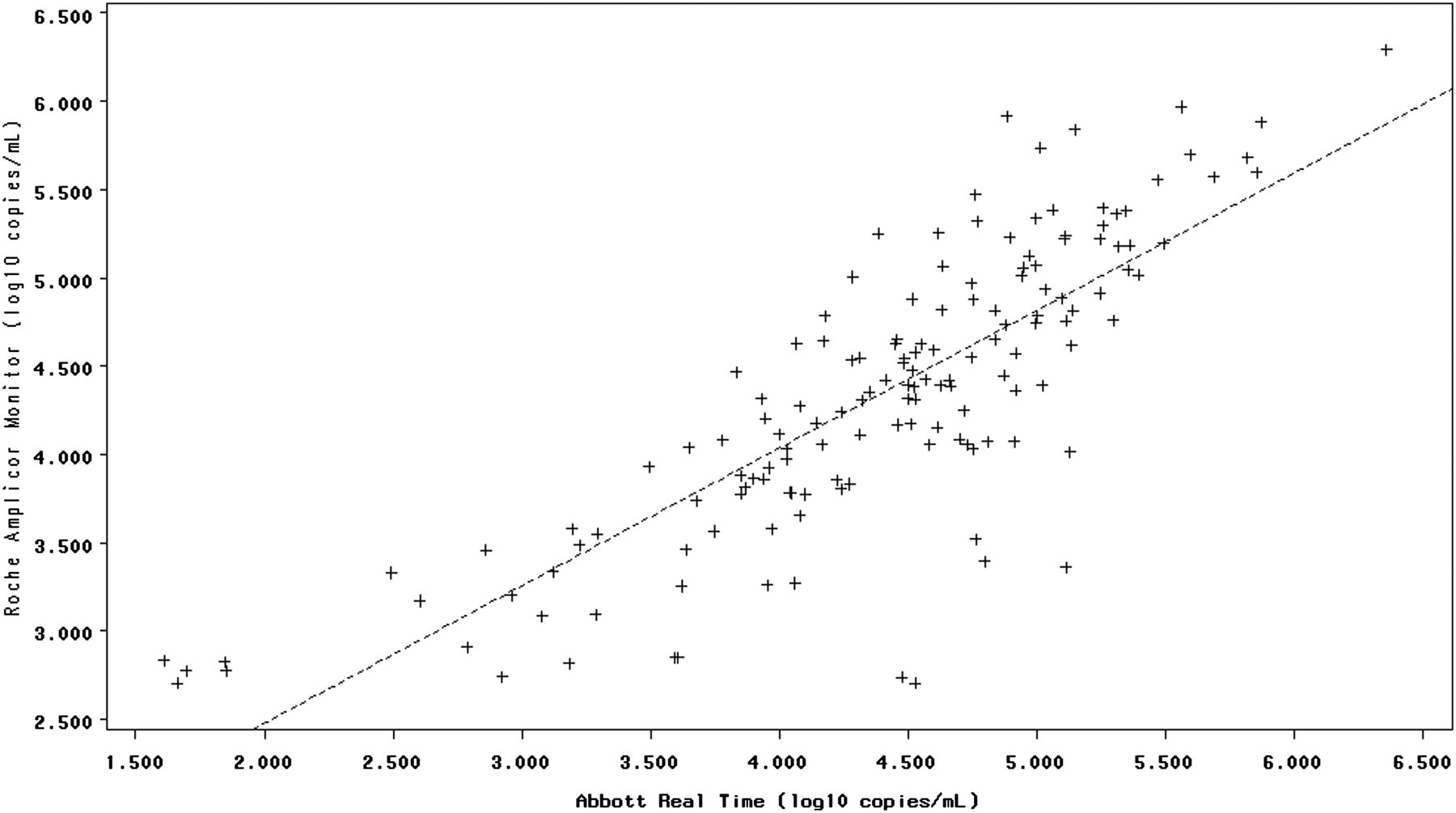
Linear relationship between Abbott m2000 Real-Time and Roche AMPLICOR Monitor v1.5 for 151 plasma samples. The dashed line represents the fitted regression line (regression equation: y = 0.7787x + 0.9211, r = 0.815)

Agreement between Abbott m2000 Real-Time and Roche AMPLICOR Monitor v1.5 according to the Bland–Altman model. Solid lines are mean ± 2SD
DISCUSSION
Global efforts to increase access to HIV treatment and care have resulted in over three million individuals receiving ART by the end of 2007. The need for VL monitoring in this setting has become apparent with several studies showing the limitations of relying solely on immunological monitoring. 1,2,4,5 There is an urgent need for accurate and cheaper methods of VL determination to support individuals receiving ART.
This study is one of the first field evaluations of the Abbott assay using manual extraction in sub-Saharan Africa. Several preliminary evaluations have compared the Abbott assay with other VL assays and its utility in quantifying the genetically diverse type M subgroups and O and N subtypes. 7–9 The distribution of subtypes within the Rakai Community Cohort, based on 812 subjects tested in 2002, was A: 23.3%; C: 0.9%; D: 62.4% and recombinant strains: 13.4%. 10 It is unclear whether subtype differences could play a role in discordant results, as we do not have subtype data for these patients.
The manual extraction method was evaluated specifically for our setting where maintaining sophisticated laboratory equipment can be costly and logistically challenging. Our results show that the assay can be deployed to monitor response to therapy in RLS with realtime PCR capacity. The Abbott assay has several advantages over the conventional ‘gold-standard’ Roche platform, which make it an attractive option for our setting. The realtime methodology lowers the risk of contamination, offers a rapid turnover time and requires less stringent technical skills on the part of operators. This assay has also been evaluated recently among Italian patients for its performance on dried blood spot (DBS) specimens 11 which is an added advantage. Correlation with traditional plasma specimens was excellent in this analysis of 169 participants. DBS specimens offer several logistical advantages for RLS by overcoming transport barriers and offering centralized testing in a sophisticated laboratory to patients receiving HIV treatment in remote locations with limited laboratory support. The Abbott assay performance characteristics were excellent and consistent with those published by other investigators. 12 Manual extraction added hands-on labour to the otherwise automated procedures but also minimized the equipment requirements in our field laboratory setting. The assay provides an additional option for laboratory monitoring of HIV patients receiving ART as the global scale-up continues.
Footnotes
The authors would like to thank Abbott Molecular Inc for providing the instruments, assay reagents and supplies to support this study. The study was supported through the Division of Intramural Research, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD. This project has been funded in whole or in part with federal funds from the National Cancer Institute, National Institutes of Health, under contract HHSN261200800001E.