
Abstract
Thirty years after the first HIV case in French Guiana, the drivers of the epidemic are not clearly known, but the epidemic is usually conceptualized as generalized. Cross-linking results from a study in the general population and a study in the HIV-infected population in Cayenne suggests that in the general population of HIV-positive men, 45% of HIV cases are attributable to having sex with someone they paid. Similarly, for HIV-positive women exchanging sex for presents or money, 10.7% of HIV cases are attributable to transactional sex. A surprising finding was that 16.8% of HIV patients had tried crack cocaine before. On the Maroni river, the female-biased sex ratio suggests the drivers in that remote area may be related to cultural polygyny. These observations have important consequences on communication and prevention strategies.
INTRODUCTION
French Guiana is a French territory situated between Brazil and Suriname. Because of its perceived riches, it attracts numerous migrants from the greater Caribbean and Brazil who come in search of a better life. Twenty-nine per cent of French Guiana's population are immigrants. With a prevalence of 1.5% in pregnant women, it is the French territory most affected by the HIV epidemic. 1 According to the UNAIDS Estimation Projection Package software, the HIV incidence rate seems to have peaked in 1995, and then dropped simultaneously with the introduction of highly active antiretroviral therapy (HAART). 2 Most of the patients (80%) are migrants. The specific prevalence in Haitian and Guyanese pregnant women oscillates between 3% and 4% and the prevalence in French pregnant women is 0.7%. Because of concerns of stigmatizing immigrants, the term generalized epidemic has been a convenient way to reduce the public's usual perception that HIV is a foreigner's disease, one of the many problems linked to immigration. However, this view that everyone in the general population is equally at risk has tended to percolate thinking about prevention and communication strategies, which have not been very proactive in targeting vulnerable groups. It has recently been emphasized that to intensify prevention it was crucial to ‘know your epidemic’. 3 Now, 30 years after the beginning of the epidemic in French Guiana, we are still not quite sure as to what is driving the epidemic, but our response aims at a generalized epidemic. However, according to UNAIDS, as with many of the Caribbean countries, we are facing a mixed epidemic. 3 Here, we review epidemiological data from French Guiana to begin answering the question of what is driving the epidemic in French Guiana. The answer to this question should greatly affect prevention priorities.
METHODS
To investigate the HIV epidemic data from French Guiana part of the French Hospital Database on HIV which has clearance with the Commission Nationale Informatique et Libertés were used. Impact measures were calculated by computing data from a cross-sectional study conducted on 95 consecutive patients (55 men and 40 women) by a physician working at Cayenne General Hospital, and data from the knowledge, behaviour, attitudes and practices in the general population of French Guiana published by the Agence Nationale de Recherche sur le Sida. In the latter study, patients were randomized using landline telephone number lists, and surveyed by telephone in 2004. Some of the questions were for men about having given money or gifts for sex and for women about having ever had sex for money or gifts. The physician asked patients in face-to-face interviews using a structured questionnaire whether at the time of diagnosis patients were using the services of sex workers or having sex in exchange for gifts or money. Questions were also asked about the use of crack cocaine at the time of the HIV diagnosis. Two other studies were used: one retrospective study in the Department of Dermatology in Cayenne evaluating the proportion of patients with prurigo or herpes zoster that were HIV positive between 1985 and 2003, and a retrospective study compiling HIV cases from the remote health posts situated on the Maroni river.
Data were analysed using STATA 9.0 (STATA Corp, College Station, TX, USA).
RESULTS
All three main centres follow >80% of foreigners. However, the profile of epidemics varies dramatically between Cayenne and Saint Laurent du Maroni. In Cayenne and Kourou, a majority of patients are Haitians (46% and 49%, respectively). In Saint Laurent, a majority of patients come from neighbouring Suriname (49.7%). In Cayenne, the sex ratio (male/female ratio) for HIV patients is 0.9, in Kourou it is 0.72, whereas in Saint Laurent du Maroni the sex ratio is 0.6. The prevalence of HIV among sex workers followed by a local non-governmental organization (NGO) (Entr'Aides) in Cayenne was estimated at 6.3% (95% confidence interval [CI] = 3–11%). HIV prevalence among prisoners fluctuates between 5% and 10% (rapid turnover).
Table 1 shows that people having paid for sex and persons receiving money or gifts for sex were at greater risk of HIV. More interestingly, the data allow one to compute exposed and population attributable risks for having had sex with sex workers. Among HIV-positive men having paid for sex, 91.9% of HIV cases are attributable to transactional sex. In the general population of HIV-positive men, 45% of HIV cases are attributable to having sex with someone they paid. Similarly, for HIV-positive women exchanging sex for presents or money, 85.6% of HIV cases are attributable to transactional sex. In the overall HIV-positive female population, 10.7% of HIV cases are attributable to transactional sex. A surprising finding was that 16.8% of HIV patients had tried crack cocaine before. This proportion is not known in the general population, therefore odds ratios and impact measures could not be measured. However, this seems a very high proportion and naturally suggests that a portion of HIV patients are greater risk takers. However, it also raises the possibility that crack cocaine is an underestimated driver of the epidemic.
Odds ratio between HIV and transactional sex
CI = confidence interval
Figure 1 shows a lag in the increase in HIV prevalence among pregnant women on the remote Maroni river when compared with the rest of French Guiana. The first cases of HIV spread to the more isolated areas by boatmen who are very mobile and often have different partners along the river. The Maroon populations of the river are often polygynous, which may have facilitated the rapid increase of HIV prevalence in the 1990s. This would also account for the female-biased sex ratio in western French Guiana. Figure 2 shows that HIV prevalence in Cayenne has remained stable in Haitians and French Guianese patients, but that it has dramatically increased during the 1990s in patients from Guyana, Suriname and the Dominican Republic.

Comparison of HIV prevalence between pregnant women from all of French Guiana and those from the Maroni river
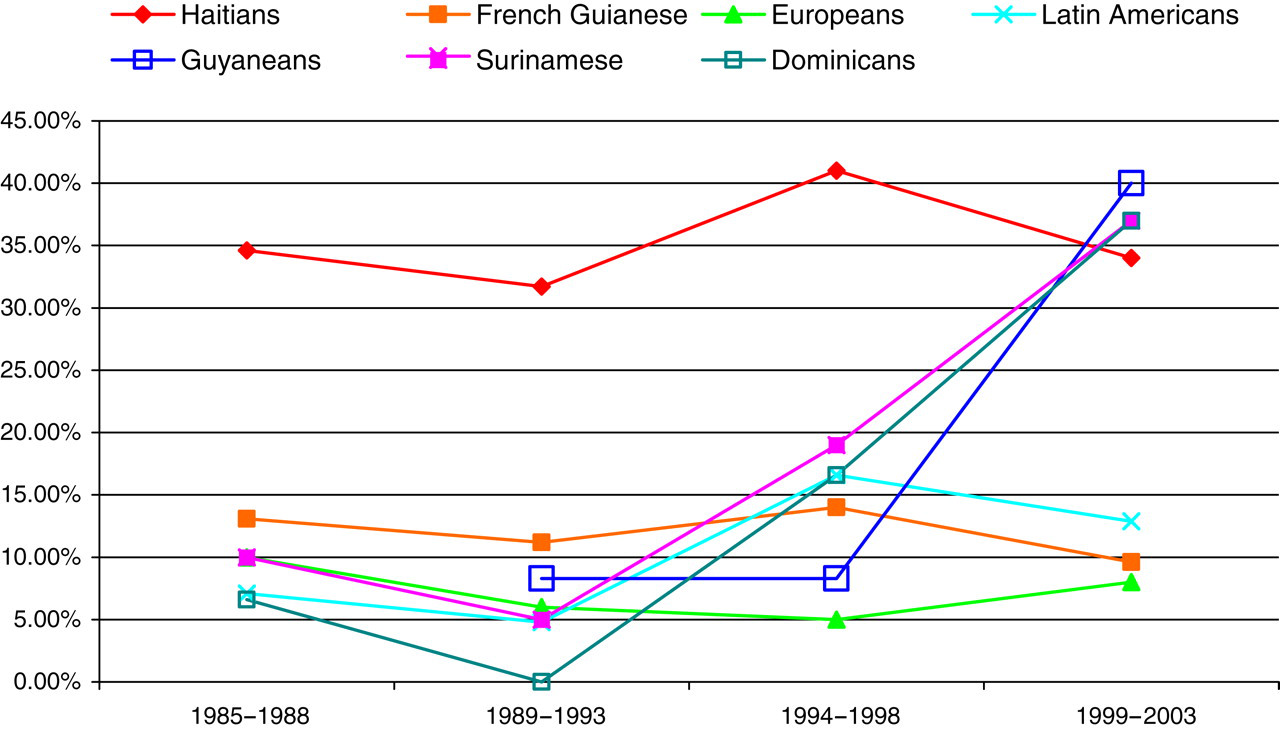
Evolution of the proportion of patients in Cayenne with prurigo or herpes zoster that are HIV positive
DISCUSSION
From our investigations of a single sparsely populated territory, we seem to observe two HIV epidemics, the first in the main city of Cayenne where transactional sex and perhaps cocaine are important drivers, and the other one on the remote rivers where concurrent partnerships may have played a key role in the rapid spread of HIV– such as on the Maroni river. 4,5 This simplified view downplays the probable complexity of these drivers, which most likely operate in both regions with different intensities. Further studies should focus on establishing a clearer picture of what is driving the epidemic in different parts of the territory and interventions should be strategically tailored to these geographical regions. To achieve this, it is essential that potential drivers of the epidemic be investigated simultaneously in both HIV-infected patients and in the general population in order to obtain the impact measures required to select the most pertinent interventions.