
Abstract
This study assessed genital shedding of HIV in patients on intermittent combination antiretroviral therapy (cART) and assessed predictors of having detectable genital HIV RNA in 156 Thai patients with CD4 > 350 cells/μL and HIV RNA ≤50 copies/mL who were randomized to continuous therapy (CT, n = 65) or CD4-guided cART (n = 91). There were 383 matched genital and plasma HIV RNA samples (CT: 158, CD4 guided: 225). In 14 samples collected within eight weeks of treatment interruption, detectable HIV RNA was present in 29% of genital samples and 71% of plasma samples. In 55 samples collected after eight weeks of treatment interruption, detectable HIV RNA was present in 60% of genital samples and 98% of plasma samples. In 110 samples collected up to 96 weeks after treatment re-initiation, detectable genital HIV RNA was found in 8% of samples and all of these were within the first 17 weeks. Independent predictors of detectable genital HIV RNA were increasing age and increasing concentrations of HIV RNA in plasma. These findings support the role of cART in maintaining undetectable HIV RNA in genital secretions.
Keywords
INTRODUCTION
Following the release of the ‘Swiss Statement’, 1 there has been vigorous debate on HIV transmission in people taking combination antiretroviral therapy (cART), and more recently there has been discussion on the role of universal treatment for preventing HIV transmission. 2 Sexual transmission of HIV is the principal mode of HIV spread worldwide, and there is an 8–20 times greater risk of transmitting HIV during primary infection due to high viral load observed in plasma and presumably the genital secretions. 3,4 In general, plasma and genital HIV RNA levels correlate, and treatment with cART leads to a reduction in HIV RNA in both compartments. The correlation between blood and genital HIV RNA is less pronounced in women, but treatment also results in a pronounced suppression of female genital HIV RNA. 5 Genital inflammation or the presence of sexually transmitted diseases (STDs) increases HIV RNA in genital secretions. 6–8 Studies in untreated patients have shown a step-wise increase in genital HIV RNA with declining CD4 cell counts. 9 In addition, poor adherence to cART leads to increases in plasma HIV RNA 10 and will also likely result in detectable HIV RNA in genital secretions, particularly if several doses of medication are missed. Even if patients are continuously treated with medication, genital shedding of virus can occur when viral load is undetectable in plasma. 11,12
STACCATO was a multicentre trial of structured treatment interruption 13 where patients were randomized to continuous therapy (CT) versus CD4-guided cART. Scheduled treatment interruption (STI) strategies have been investigated as an option for patients to temporarily stop cART to improve their quality of life, reduce toxicity and cost. 14 Almost all patients have an HIV RNA rebound in the plasma and the risk of transmission is a major public health concern. 15 However, patients on cART can also have genital shedding of virus. 16 To further explore the relationship between HIV RNA in plasma and genital secretions and inform the debate about transmission risk and HIV treatment, we analysed data from a STACCATO genital secretion substudy, exploring the relationship between plasma and genital HIV RNA levels and the influence of other patient and treatment characteristics. 6–8
METHODS
This was a substudy of STACCATO (n = 430) performed at one site in Bangkok, Thailand (The HIV Netherlands Australia Thailand Research Collaboration, HIV-NAT). STACCATO was a prospective, open-label, randomized, multicentre trial conducted in Thailand, Switzerland and Australia. 13 Patients with chronic HIV-1 infection and virological (HIV RNA < 50 copies/mL or 1.7 log10 copies/mL) and immunological response (CD4 >350 cells/μL) to cART were randomized in a 1:2 proportion to CT and CD4-guided arms. In Thailand, cART consisted of two nucleoside reverse transcriptase inhibitors (NRTIs) plus saquinavir/ritonavir 1500 or 1600/100 mg once daily. In the CD4-guided arm, patients started the trial by discontinuing cART. They restarted cART if CD4 dropped below 350 cells/μL. They stopped again after at least 12 weeks on cART and if the confirmed CD4 count rose above 350 cells/μL. STACCATO is registered at ClinicalTrials.gov with the identifier NCT00113126.
The goal of the genital secretion substudy was to compare measures of HIV infectiousness (genital viral shedding) and the relationship to stopping and starting cART and other factors in patients in STACCATO. Chulalongkorn University Ethics Committee approved the study, and all patients signed written informed consent at screening. STDs were investigated in patients with relevant symptoms. Vaginal candidiasis was also reported in the results of annual cervical Pap smears, which were offered to all women in the study.
HIV RNA levels in semen/vaginal secretions were measured at various intervals after cART in the CT arm and after cART discontinuation and re-initiation in the CD4-guided arm, but some patients opted not to contribute samples at every time point. In addition, patients were assessed for CD4 count, plasma HIV RNA, clinical and laboratory adverse events and HIV disease progression every four weeks during the first 12 weeks and then every 12 weeks thereafter.
Semen samples were processed within four hours after ejaculation. After centrifugation (1500
Statistical analysis
Datasets from clinical trial databases were analysed using SAS 9.13 (SAS Institute, Cary, NC, USA) and Stata 10 (Statacorp, College Station, TX, USA).
Rates of detectable HIV RNA in plasma and genital samples were described in paired samples by patient and treatment characteristics. To determine what factors predicted having detectable HIV RNA in genital secretions over the duration of the study, we used a longitudinal random effects logistic regression model to account for time on study and within-subject variability. Random effect models are used as they allow for both within and between patient variability appropriately and for differing numbers of HIV RNA assessments within patients. For example, some covariates such as age or sex are comparisons between patients, whereas other factors such as the patients being in a treatment interruption or still on ART are at least partially within patient. 18 Covariates tested in univariate analysis included whether patients were on or off treatment and whether this was shorter or longer than eight weeks, CD4 count at time of genital HIV RNA sample collection, age, gender, whether patients had clinical AIDS at baseline and the HIV RNA concentration in plasma. Covariates with P ≤ 0.05 in univariate analysis were adjusted for in a multivariate model. Likelihood ratio tests were used to calculate P values in multivariate models.
RESULTS
One hundred and fifty-six patients (65 from the CT arm and 91 from the CD4-guided arm) contributed a total of 383 matched genital and plasma HIV RNA samples (158 from the CT arm and 225 from the CD4-guided arm) to the study. One hundred and forty-four samples were semen and 239 samples were vaginal secretion. The baseline characteristics of patients in the study cohort are shown in Table 1.
Baseline characteristics for 156 patients in genital shedding substudy
IQR = inter quartile range; CDC = Centers for Disease Control and Prevention
Sixty-nine samples were collected from patients during a treatment interruption, and 314 samples were collected while patients were on treatment. Actual week of sample collection in the trial and whether the patient was on or off treatment at the time is shown in Table 2. One hundred and ten of these on-treatment samples were collected while the patients were being retreated after a treatment interruption. A diagrammatic representation of a treatment schedule and sample collection is shown in Figure 1.
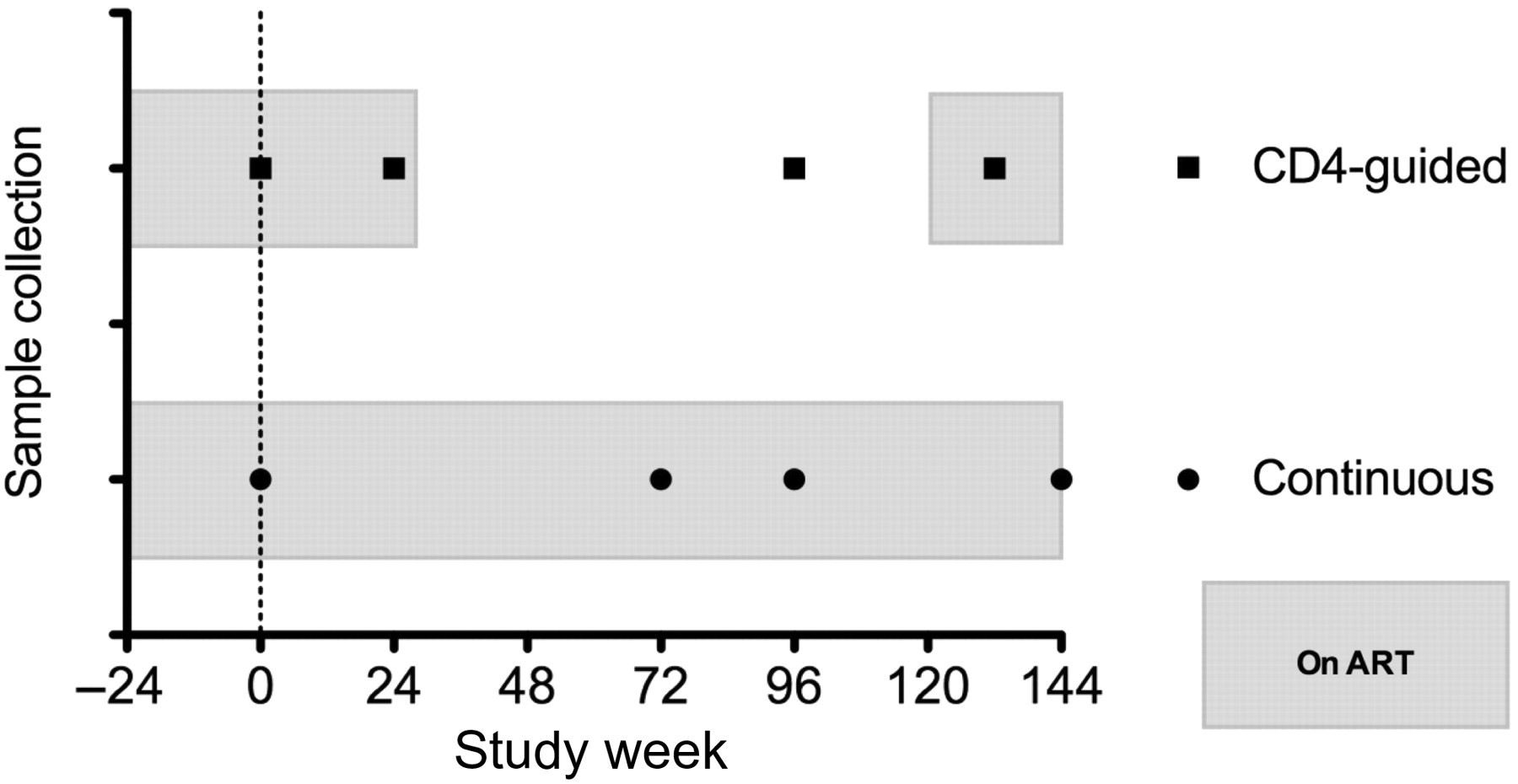
Diagram showing periods of treatment with cART and genital sample collection from two patients in the genital secretion substudy. Week 24 represents the minimum period of cART induction and week 0 represents randomization. Periods shaded in grey are while the patient is on cART (combination antiretroviral therapy)
Weeks of sample collection and whether patients were on or off cART
cART = combination antiretroviral therapy
HIV RNA in off-treatment plasma and genital samples
In 14 samples collected in the first eight weeks after treatment interruption, HIV RNA was detectable in four (29%) genital samples and 10 (71%) plasma samples. In samples collected after eight weeks, detectable virus was present in 22/33 (60%) genital samples and 54/55 (98%) of plasma samples (Figure 2a). After stopping treatment, the median inter quartile range (IQR) concentration of HIV RNA in 22 semen samples with detectable HIV RNA was 3.96 (3.33–4.61) log10 copies/mL and in 15 vaginal secretion samples with detectable HIV RNA was 3.26 (3.09–3.79) log10 copies/mL.
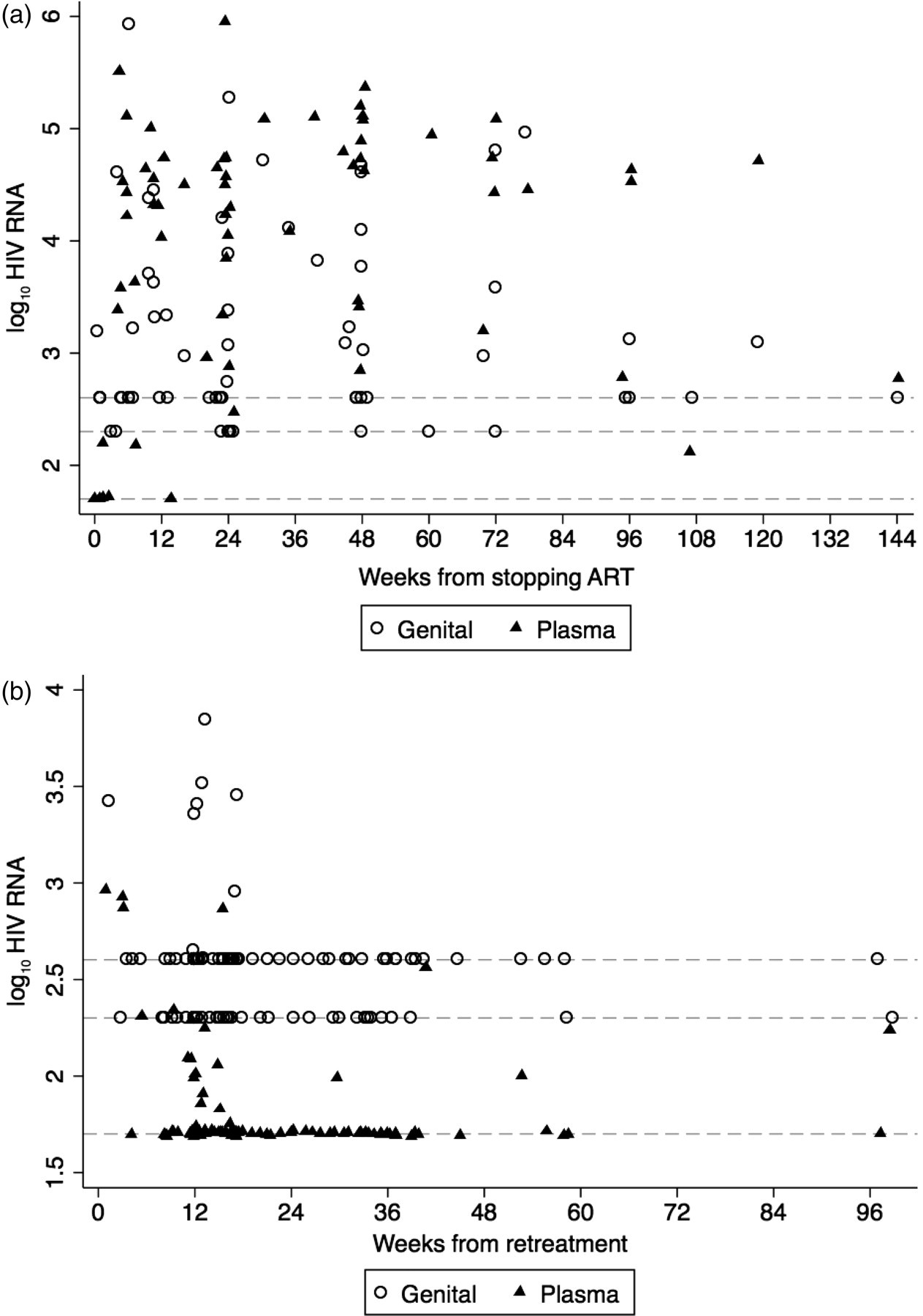
Plasma and genital HIV RNA samples in patients (a) after interrupting treatment and (b) after restarting treatment. Scales on x- and y-axis are different. Dotted lines on the y-axis from the bottom to the top represent limit of detection of HIV RNA in plasma, semen and vaginal secretions, respectively
HIV RNA in re-treatment plasma and genital samples
In 110 samples collected after treatment re-initiation in patients who experienced a treatment interruption, genital HIV RNA was detectable in nine (8%) samples and all of these were in the first 17 weeks (Figure 2b). In the matching plasma samples, HIV RNA was detectable in four (4%) samples and in 22 (20%) of the total number of samples (Figure 2b). After re-initiation of treatment, the median (IQR) concentration of HIV RNA in five semen samples with detectable HIV RNA was 3.46 (2.65–3.51) log10 copies/mL and in vaginal secretions with detectable HIV RNA was 3.38 (3.15–3.42) log10 copies/mL
HIV RNA in plasma and genital samples while patients were on continuous treatment
In samples collected when patients had been on continuous treatment, the proportion of samples with detectable genital HIV RNA was 17/204 (8.3%) and the proportion of samples with detectable plasma RNA was 11/204 (5%).
In all samples collected during the study, HIV RNA was detectable in 97/383 (25%) plasma samples and 63/383 (16%) genital secretion samples. Twenty-five percent of all genital samples collected from semen had detectable HIV RNA compared with 11% of the samples collected from vaginal secretions (P < 0.001). HIV RNA was more commonly detected in the genital secretions of older patients: the proportions of samples from those aged <30, 30–40 and >40 years were 10%, 16% and 26%, respectively (P = 0.025). Genital HIV RNA was detectable in 21/286 (7%) samples when plasma HIV RNA was undetectable. We were unable to show a linear relationship between plasma and genital HIV RNA concentrations, but the proportion of genital samples with detectable HIV RNA increased with increasing concentrations of plasma HIV RNA. When the plasma HIV RNA concentrations were between 1.7–2.99, 3–3.99, 4–4.99 and >5 log10 copies/mL, the proportions of corresponding genital samples with detectable HIV RNA were 18%, 33%, 63% and 82%, respectively (P < 0.001).
To assess the factors associated with having a detectable genital HIV RNA we applied a random effects longitudinal logistic regression model (Table 3). In univariate analysis, increased odds of having detectable HIV RNA in genital secretions were seen with time off treatment, male gender, increasing age and increasing concentrations of plasma HIV RNA. After adjusting for other variables in a multivariate model, two factors were independently associated with a detectable genital HIV RNA. These were increasing age (P = 0.005) and increasing concentrations of HIV RNA in plasma (P = 0.001). Compared with those aged <30 years, there were increased odds of having detectable genital HIV RNA in those aged 30–39 years (odds ratio [OR] 2.8, 95% confidence interval [CI] 1.1–7.5) or those ≥40 years or older (OR 6.2; 95% CI 2.0–19.2). Compared with those with undetectable HIV RNA in plasma, there were increased odds of having detectable genital HIV RNA with increasing plasma HIV RNA concentrations. The highest odds were seen in those with plasma HIV RNA >5 log10 copies/mL (OR 32.3, 95% CI 3.9–266.7).
Factors associated with detectable genital HIV RNA in univariate and multivariate analysis
OR = odds ratio; CI = confidence interval
There were no cases of concomitant STDs detected. One case of vaginal candidiasis was suggested by the presence on a Pap smear from a CT arm patient at week 48. This patient's HIV RNA in the genital compartment was 3.43 log10 copies/mL with an undetectable HIV RNA in the plasma.
DISCUSSION
Our study showed that genital secretion of HIV RNA became detectable once cART was interrupted in patients who previously had undetectable genital secretion HIV RNA while on cART. This provides evidence suggesting increased HIV infectiousness following treatment interruption. 15 In multivariate models, after adjusting for whether the patient was on or off cART and gender, the only independent predictors of detectable HIV RNA in genital secretions were older age and increasing concentrations of plasma HIV RNA.
This study is unique in that it looks at HIV RNA shedding in the genital tract following structured treatment interruption in a uniform population. After unplanned treatment interruption, HIV RNA rebound in both plasma and semen was reported in 12 men who mostly had detectable HIV RNA prior to interruption. The reintroduction of various cART regimens in seven patients resulted in HIV RNA decline. 19 The detection of HIV RNA in semen and vaginal secretions during periods of HIV plasma viremia is consistent with other studies in ART-naïve and ART-experienced populations. 8,20 Subtypes may also affect shedding of HIV in genital secretions. For instance, women with HIV subtype C were significantly more likely to shed HIV-infected vaginal cells than were those infected with subtype A or D. 19 The most common subtype in Thai patients is CRF_01AE. 21
Sexual transmission of HIV is the principal mode of HIV spread worldwide. The most important risk factors for transmission are HIV viremia and STD co-infection. We may have underestimated the occurrence of STD in our patients as we relied mainly on patient's self-report. ART suppresses HIV viremia in the plasma and in the genital tracts and likely lowers the risk of transmission. Reduced seroconversion rates were seen among HIV-negative partners of cART-treated subjects. 22 Quinn et al. 23 found a significant dose–response relationship between plasma HIV RNA and heterosexual HIV transmission with no transmission occurring among discordant couples if the infected partner had plasma HIV RNA below 1500 copies/mL. In a recent meta-analysis, Attia et al. 24 described low transmission rates in people taking cART, but increasing rates of HIV transmission as plasma HIV RNA increases in patients who were not currently taking cART.
The chance of heterosexual transmission is estimated to be one per 100 episodes of intercourse if the semen HIV RNA is 5 log10 copies/mL and three per 1000 episodes if the semen is 3 log10 copies/mL. 25 The median genital secretion HIV RNA in our patients following treatment interruption was 2 log10 copies/mL, and two and one patients had HIV RNA above four and 5 log10 copies/mL, respectively. These patients pose a risk for HIV transmission if adequate protection is not used. Indeed, unprotected sex is not uncommon; it was reported in 12% of almost 5000 HIV-infected Swiss individuals surveyed. 26 Additionally, a case of HIV transmission during treatment interruption was reported in a discordant couple who stopped practising safe sex after the infected partner became HIV RNA undetectable on cART, and continued to have unsafe sex during an STI cycle. 15 Therefore, individuals on cART should be counselled about the possibility of highly increased transmission risk if they interrupt therapy for any reason and have unprotected sex. In STACCATO, all patients were informed about this increased risk after treatment interruption.
It was uncommon for our patients to have a detectable genital HIV RNA samples if their plasma HIV RNA was undetectable. The degree of association between plasma and genital secretions HIV RNA varies between studies. A review of 19 studies showed that the best association between HIV RNA in plasma and semen was seen in those on successful cART who did not have co-occurring STDs. In a study of 145 HIV-infected men in an assisted reproductive technology programme who had undetectable plasma HIV RNA and no STD, detectable HIV RNA was found in semen in 5% of subjects who had undetectable plasma HIV RNA for at least six months. 11 Another recent report found detectable seminal HIV RNA in the presence of undetectable plasma HIV RNA in almost half of the men studied. 16 Indeed, isolated seminal shedding of HIV may be common, even after extremely prolonged suppression of HIV RNA in plasma. 12 Similar to other studies, the limits of detection of HIV RNA in semen and vaginal fluids in our study were higher than that in plasma. 27,28
Increasing age was a risk factor for detectable genital HIV RNA in our patients and this may be related to physiological processes associated with aging in HIV such as premature immunosenescence leading to poorer viral control. Patients who had genital HIV RNA above 3 log10 copies/mL were on average four years older than those with a lower HIV RNA, but their samples were also collected after longer times off therapy which may also account for this difference.
The genital compartment serves as a persistent and distinct latent HIV-1 reservoir from plasma. 7 Significant genotypic differences in HIV from matched plasma and vaginal secretions suggest that cellular replication of HIV occurs independently in these compartments. 29,30 Unfortunately, we do not have genotypic data in our patients to illustrate this finding. Genital compartment penetration differs among antiretrovirals. In contrast to protease inhibitors (PIs), nucleoside reverse transcriptase inhibitors (NRTIs) and non-NRTIs generally achieve higher drug concentrations in genital secretions. 31–33 However, a study conducted in women found less genital shedding in patients on a PI-based therapy such as the treatment used in STACCATO. 5 Whether treatment with drugs with high genital compartment penetration is necessary for suppression of genital secretion HIV RNA and control of transmission is unclear. A recent study showed that patients achieve HIV RNA suppression in semen despite undetectable antiretroviral drug level in the genital compartment. 28 Our patients were treated with two NRTIs plus saquinavir/ritonavir and for those who had undetectable plasma HIV RNA, the HIV RNA was almost always suppressed in the genital secretion.
A limitation of our study was that patients were not required to contribute genital samples for HIV RNA testing at every visit, and some patients declined to do so at some time points. For this reason the data were analysed with a longitudinal logistic regression model adjusting for time on study, rather than using a time to event approach. Nevertheless, our study provides information on the relative importance of predictors of detectable HIV RNA in genital secretion. Our results therefore, have important public health implications and further inform the debate arising from the ‘Swiss Statement’. 1 We found the odds of a detectable HIV RNA in genital secretions were significantly increased in patients with detectable plasma HIV RNA, after adjusting for gender, age and whether the patient was on or off treatment. If patients are non-adherent and accumulate resistance mutations, those with detectable HIV RNA are at increased risk of transmitting these resistant viruses.
CD4-guided treatment is currently not recommended due to the results of the Strategic Management for Antiretroviral Therapy (SMART) study showing that cART interruption causes more non-AIDS and AIDS events. The risk of these serious events increases as CD4 declines. 34 Moreover, data from cohort studies suggest that earlier cART initiation may prevent deaths from AIDS and non-AIDS illnesses 35 leading to guidelines recommending that cART initiation be revised. 36,37 As cART has the potential to reduce the spread of HIV, 38 starting therapy earlier may lower the number of new infections globally. CD4-guided treatment, however, leads to detectable HIV RNA in genital fluids and may increase the risk of sexually transmitted HIV.
Footnotes
ACKNOWLEDGEMENTS
We are grateful to the volunteers for participating in this study. We thank Dr Angele Gayet-Ageron for providing data from the STACCATO database and the following HIV-NAT staff for helping with recruitment and collection of data and specimens: Ms Sukontha Saenawat, Ms Saijai Wicharuk, Ms Siriporn Nonenoy and Ms Sineenart Chautrakarn. We thank Ms Piraporn Ohata for formatting this manuscript.