
Abstract
Patients with HIV/AIDS are often afflicted with oesophageal disorders. Opportunistic infections such as candidiasis, herpes simplex, cytomegalovirus, mycobacterial infections, Kaposi sarcoma or lymphoma involving the oesophagus, motility disorders and reflux oesophagitis are the usual culprits. Eosinophilic oesophagitis (EE), a recently recognized entity, is an important cause of dysphagia, food impaction and chest discomfort. We report the case of an HIV-infected man who had persistent dysphagia for six months despite treatment with proton pump inhibitor. He was diagnosed with EE after having endoscopic evaluation and biopsy of his oesophagus and was successfully treated with swallowed fluticasone. This case represents the first reported case of EE in an HIV-infected individual.
INTRODUCTION
Oesophageal disease is common in patients with AIDS, often presenting as dysphagia, odynophagia and retrosternal discomfort. Opportunistic infections are the leading causes with oesophageal candidiasis being the most common, followed by viral (herpes simplex virus, cytomegalovirus), mycobacterial or other fungal aetiologies. HIV itself can be responsible for ulcerative oesophagitis. Other oesophageal maladies include reflux oesophagitis, Barrett's oesophagus, motility disorders and malignancies (Kaposi sarcoma, lymphoma). 1
We report the case of an HIV-infected patient who presented with intractable dyspepsia despite six months of proton pump inhibitor (PPI) therapy. He was finally diagnosed with eosinophilic oesophagitis (EE). To our knowledge, this is the first report of EE in an HIV-positive patient in the English literature.
CASE SUMMARY
A 40-year-old Caucasian man presented with a six-month history of intractable dyspepsia associated with retrosternal pain, dysphagia and odynophagia. He had no relief with PPI therapy. The patient's past medical history was notable for HIV infection, naïve to antiretroviral therapy, with a CD4+ T-cell count of 395 cells/μL and an HIV viral load of 69,208 copies/mL, as well as osteoporosis and allergic rhinitis. His medications included esomeprazole, calcium gluconate, vitamin D and weekly alendronate. He did not report nausea, vomiting, food impaction, fevers or weight loss. Physical examination revealed no oral thrush, no abdominal pain or organomegaly. The peripheral eosinophil count was 700 cells/μL and ESR 35 mm/hour. Immunoglobulin E levels were normal, and anti-gliadin antibodies were negative. Allergy skin testing was unrevealing. Despite intensifying PPI therapy, discontinuing the alendronate, increasing physical exercise and avoiding the usual food allergens, his symptoms persisted.
Upper gastrointestinal endoscopy showed slight nodularity of the oesophageal mucosa (Figure 1), erythematous gastric mucosa and normal duodenum and jejunum. Histological evaluation from the gastroesophageal junction showed squamous mucosa with basal hyperplasia, moderate chronic inflammation and many intraepithelial eosinophils numbering an average of 20–30 per high power field (HPF) (Figures 2 and 3). These findings are compatible with EE. The gastric oxyntic and antral mucosae showed mild chronic gastritis but the duodenum had no pathological findings and no evidence for celiac disease. Stains were negative for acid-fast organisms, fungi, Helicobacter pylori and intestinal metaplasia.
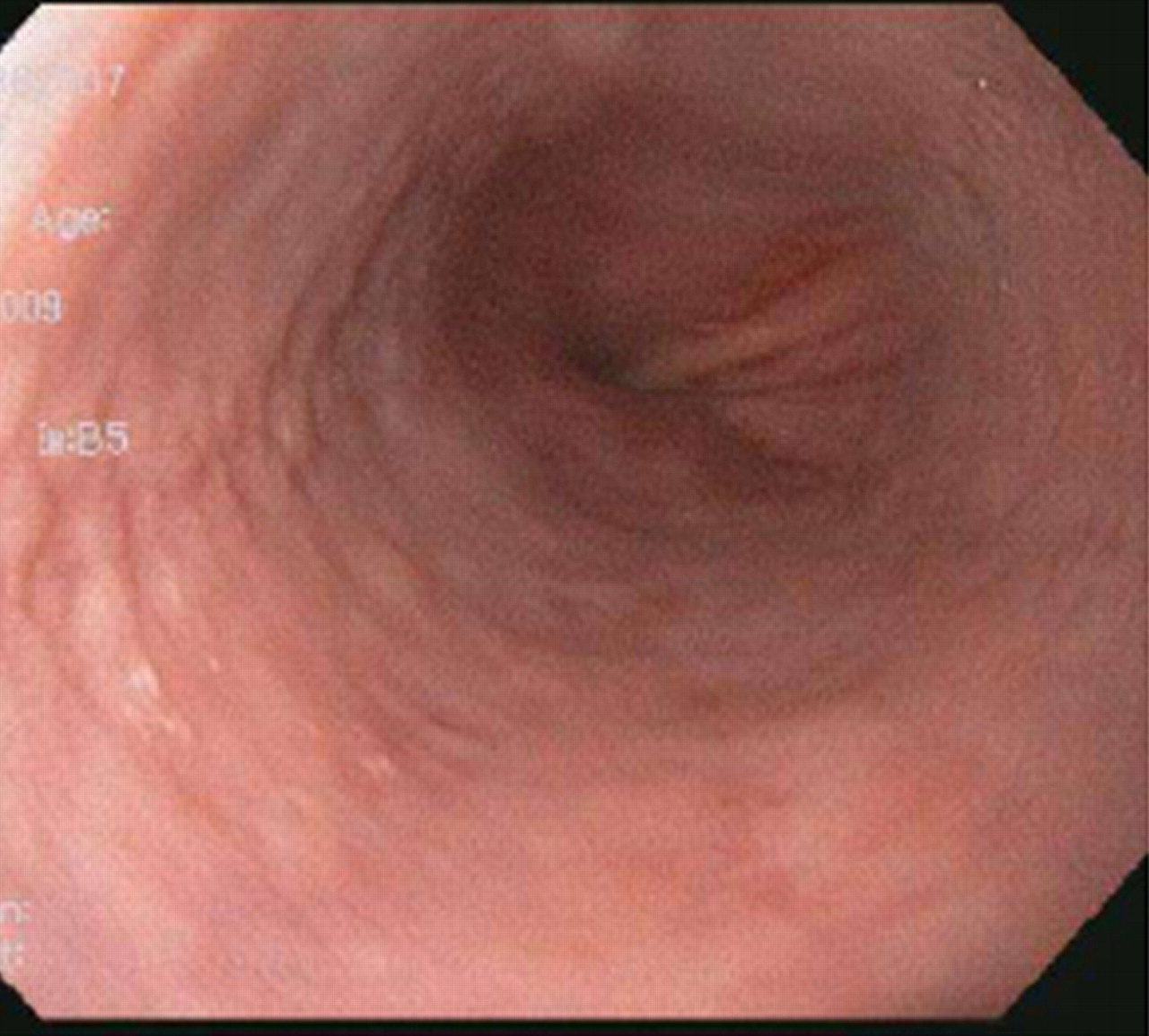
Upper gastrointestinal endoscopy demonstrating nodularity of the oesophageal mucosa

Low-power histological view of oesophageal biopsy specimen showing papillary lengthening and basal hyperplasia with multiple aggregates of eosinophils throughout the mucosa (haematoxylin–eosin, original magnification × 20)
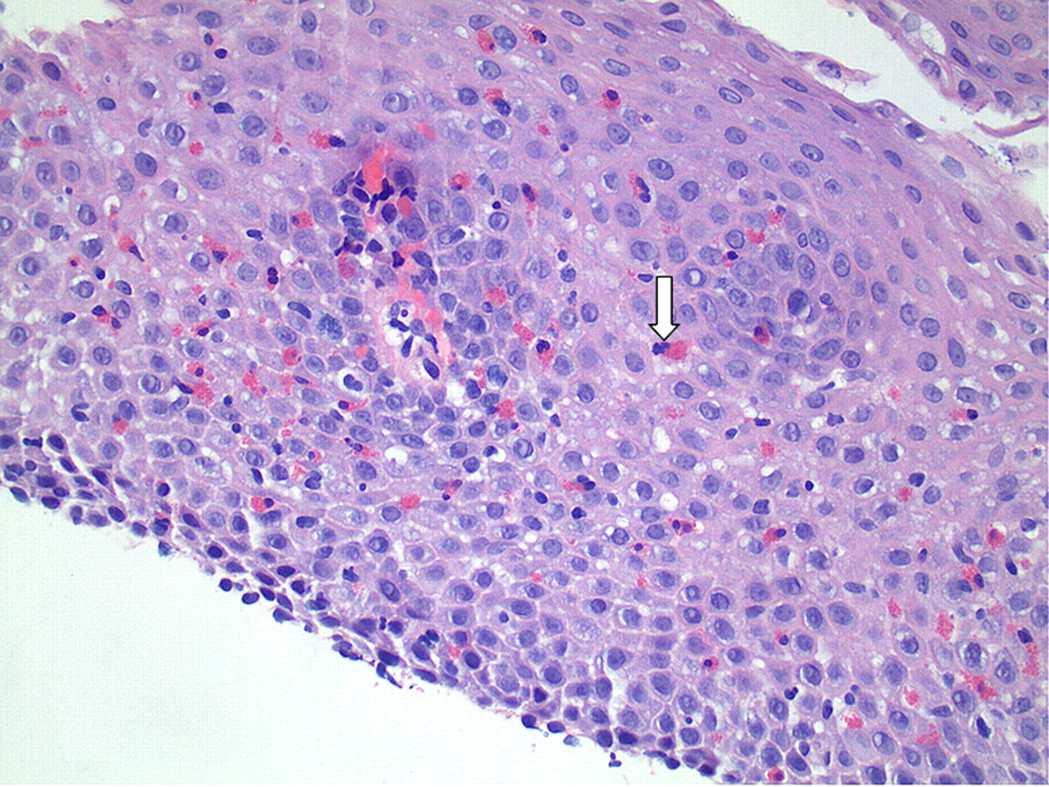
High-power histological view of oesophageal biopsy demonstrating numerous (more than 25 per high-power field) intraepithelial eosinophils (see arrow), present mainly in a superficial distribution (haematoxylin–eosin, original magnification, ×40)
The patient was started on swallowed fluticasone (220 µg twice daily), montelukast and combination antiretroviral therapy (cART) with lopinavir/ritonavir and tenofovir/emtricitabine. He completed a two-month course of swallowed fluticasone with resolution of the upper gastrointestinal symptoms. The steroids were stopped; there was no occurrence of Cushing's syndrome during concurrent fluticasone and lopinavir/ritonavir treatment. His CD4+ T-cell count had increased to 722 cells/μL and the HIV viral load decreased to 261 copies/mL. Due to the finding of mild gastritis he was maintained on PPI therapy and continued for six more weeks after fluticasone was stopped. There was no recurrence of symptoms after stopping PPI therapy. The HIV viral load became undetectable and there was no virological failure on PPI therapy. Of interest, histological evaluation of the gastroesophageal junction one year later showed no features of EE.
DISCUSSION
EE is a clinicopathological entity characterized by symptoms of gastroesophageal reflux disease and dense oesophageal eosinophilia on histology, both unresponsive to proton pump inhibition. The incidence of the disease can vary from 1 in 10,000 per year in children to 1 per 100,000 adults. 2,3 Adult cases usually present in the third and fourth decades of life. EE is more prevalent in the Caucasian population. 4 A male predominance (74%) has been observed in both adults and children. 5,6 Most cases of EE are seen in developed countries, likely secondary to an increased prevalence of atopic conditions like asthma.
The exact pathogenesis of EE is uncertain but a single-nucleotide polymorphism in the gene that regulates eotaxin-3 (a chemokine critical for eosinophil migration) is associated with disease susceptibility. 7 Studies have demonstrated an association between the infiltration of the oesophagus with eosinophils and an allergic predisposition to both food and aeroallergens. 8–10 The most commonly identified food allergens include milk, soy, eggs, wheat, peanuts and shellfish. 11,12 In one report, 50% of the children and adults with EE had been diagnosed with other allergic conditions like asthma, allergic rhinitis and eczema. 5,13 The most common presenting symptoms of EE in adults include dysphagia, heartburn, food impaction and chest pain. Patients could also experience nausea, vomiting, abdominal pain, asthma, allergic rhinosinusitis, hoarseness, cough, urticaria and atopic dermatitis. 5 The most common endoscopic findings include linear longitudinal furrows, mucosal rings or ‘trachealization’ of the oesophagus, small calibre oesophagus, white plaque/nodule-like exudates, crêpe-paper mucosa and strictures.
The diagnosis is made by histology: the criteria (although not standardized) require the presence of more than 15–20 intramucosal eosinophils per HPF. Another histological feature is the superficial layering of the eosinophils. Thickened epithelium, abnormally long papillae, eosinophilic microabscesses and extracellular eosinophilic granules can also be seen. Subepithelial fibrosis might contribute to decreased compliance of the oesophagus and the subjective symptoms of dysphagia. 14
There are no standardized treatment protocols for EE but a variety of dietary, pharmacological and endoscopic interventions can be used alone or in combination. Most patients are treated with swallowed fluticasone, dietary modifications and avoidance of allergens, if identified. Antireflux therapy usually achieves only a partial response. Restriction diets, however, have not been successful in adults. 15 A PPI can be helpful as the already affected oesophageal mucosa could be further damaged by acid exposure. Furthermore, the pathological diagnosis of EE should be established after a patient has been on PPI therapy for at least four weeks.
Systemic steroids and topical corticosteroids have been proven to relieve the symptoms and improve the histological findings in case series and controlled trials. For topical use the inhaled steroid formulations are swallowed to provide a coating of the entire oesophageal mucosa. A potential side-effect is the development of esophageal candidiasis; therefore we chose to start antiretrovirals in our patient to minimize this risk. We hypothesize that EE may have been a presentation of symptomatic HIV disease in our patient: while steroids and montelukast were instrumental in alleviating symptoms immediately after diagnosis, HIV suppression (with immune reconstitution) might have led to ongoing remission and normal oesophageal lining 12 months after diagnosis. Swallowed fluticasone has a negligible oral bioavailability due to poor absorption and hepatic first-pass inactivation by cytochrome P450 isoenzyme CYP3A4. 15 Ritonavir is a potent inhibitor of CYP3A4 and can increase plasma concentrations of fluticasone. 16 Our patient received fluticasone and ritonavir for two months without untoward side-effects; a higher dose of fluticasone was likely achieved, thus aiding in alleviating symptoms.
The symptoms of EE can recur after discontinuation of steroids and patients may require repeated courses or long-term therapy. As the immunological pathogenesis of EE is better understood, specific immunomodulatory strategies will likely be the future source of therapeutic intervention. 17
CONCLUSION
Opportunistic infections, reflux oesophagitis and AIDS defining maladies can cause significant discomfort in affected patients. Upper endoscopy and biopsy are often necessary to establish the correct diagnosis. EE is increasingly being recognized. Clinicians should also consider EE as another possible oesophageal disease that can cause dysphagia symptoms in our HIV-infected population.
Footnotes
ACKNOWLEDGEMENTS
The authors thank Dr. Gabriel Ionescu for the endoscopy picture and Nancy Murphy, NP, for pre- and post-case data contribution.