
Abstract
Through clinical practice, it is often perceived that patients with diabetes are more likely to suffer from severe and recalcitrant warts. This study was set up to investigate if genital warts were more common in patients with diabetes and to determine if patients with diabetes and genital warts required more treatment than those without diabetes. Only female patients with diabetes and genital warts were investigated and were compared to the non-diabetic population. Results suggested that patients with diabetes had more extensive warts and recurrences. This study will hopefully further inform the debate surrounding preferential use of quadrivalent human papilloma virus (HPV) vaccine as opposed to bivalent HPV vaccine especially in the setting of a Diabetes Young Person's clinic.
INTRODUCTION
Human papilloma virus (HPV) infection is a common sexually transmitted infection in the UK. A total of 48,744 male and 43,781 female cases have been diagnosed in the UK in 2008, with the highest case burden between the ages 20–24 in women and 25–34 in men. 1 The cellular immune response is an important factor in controlling HPV infections. There are certain conditions that may predispose an individual to the acquisition or worsening of the HPV infection. These include immunosuppressive states, such as HIV infection, the use of immunosuppressant agents and pregnancy. 2,3
There is a perception among doctors working in sexual health that genital warts are more common and more difficult to treat in patients with diabetes mellitus (DM). Diabetes has been considered as an immunocompromised state. A review paper by Geerlings et al. 4 stated that patients with DM have more infections than those without DM, probably from a defective immune system. Patients with DM who develop genital herpes have more severe infections, require prolonged treatment and are more likely to develop complications such as ketoacidosis. 5
A PUBMED search looking for evidence to suggest patients with DM suffered with more severe warts found three reports from 1978 6 , 1988 7 and 2008. 8
We had previously looked at the management of genital warts in 50 patients under the age of 18 and had noted that three out of 50 had diabetes. 9 The current study was therefore set up first to investigate if genital warts was more common in our patients with DM in comparison to the general population and second to determine if female patients with DM and genital warts required more treatment than patients without DM.
METHOD
We looked through the patient diagnosis report (KC 60) from the Countess of Chester Hospital Sexual Health Clinic between 1 September 2007 and 1 September 2009, and found 562 female patients who were diagnosed with first occurrence or recurrence of genital warts. All 562 case sheets identified were then examined individually for evidence of the patient having a documented history of either type 1 or type 2 DM.
Data collected on patients with DM and genital warts were then compared with the Sexual Health Audit and Education (SHAPE) data, which previously audited the treatment of genital warts of 200 patients in the same unit. The audit results were compared with a gender-matched population where possible.
RESULTS
Twelve of these 562 patients had diabetes. Of these, nine had first occurrence of anogenital warts and three had presented with wart recurrences. The median age was 32 years, with an age range of 13–59 years. There were eight patients with type 1 DM and four patients with type 2 DM. Sixty-six percent of the patients were non-smokers (8 out of 12).
Sixty-six percent of patients (8 out of 12) had a moderate to extensive number of warts that occurred around the vulval, vaginal and perianal area. In comparison to the female patients in the SHAPE data, 63% tended to have only a single or few warts (<5). Forty-one percent (5 out of 12) of the patients with DM had perianal involvement in comparison to 12% of the general population.
Ten of 12 patients were treated with conventional methods of treatment. Conventional treatments used include ablative methods such as cryotherapy, topical chemical treatments such as podophyllotoxin 0.15%, imiquimod 5% cream and trichloroacetic acid 90%. Patient 9 declined treatment. She was psychologically traumatized from a sexual assault and found physical examination and wart treatment too invasive and therefore declined therapy. The other was patient 12 (Table 1).
Clinical course of 12 women with diabetes and genital warts
Patient 7 had multiple attendances over the last 16 years, with recurrence or persistence of warts. She also had previous surgical resection of her warts
Patient 11 was diagnosed in 2004 and has multiple occurrences since then
Patient 12 had extensive vulval and perianal warts and was referred to a surgeon for surgical management
We looked at the duration in weeks it took for the patients with diabetes to clear their genital warts. Sixty percent of patients (6 out of 10) took 12 weeks or less from the time of presentation for clearance of warts. Two patients were lost to follow-up (1 patient declined treatment and the other did not return for her follow-up appointment). Four patients took longer than 12 weeks at 20, 24 and 28 weeks, respectively. Patient 12 is yet to clear her warts.
The majority of the patients took three visits or less to completely clear their warts for that particular episode. For the four patients who took more than 12 weeks to clear their warts, three of the patients had four visits and one patient had 10 visits.
Twenty-five percent of patients (3 out of 12) had recurrences from the initial episode. All three patients had type 1 DM. Two patients had a wart recurrence within three months and one patient within eight months. The most number of recurrences for an individual patient from their initial episode was two.
DISCUSSION
The prevalence of DM in our patients with genital warts was 2% (12 out of 562). This prevalence is lower than in the general population (4–5%) 10 and does not suggest that patients with genital warts have a higher rate of diabetes.
It is not clear from this study if there is an increased prevalence of genital warts in patients with diabetes as we cannot be sure that all patients with diabetes who are afflicted with genital warts will necessarily visit sexual health services. To answer this question, a larger survey would need to be done, preferably through a young person's diabetic clinic.
The median age for this group is 32. Yearly Health Protection Agency epidemiological data reveal that the bulk of the genital wart diagnoses occurs in those under the age of 24; however, in this cohort of patients with DM, the diagnosis seems more common in the older age group.
Our data seem to suggest that patients with diabetes tend to suffer with more extensive warts when compared with patients without diabetes.
Reynolds et al. 11 showed that with appropriate treatment, warts generally clear within three months. Their audit reported 18% of female patients still had warts after three months of wart treatment when a systematic treatment algorithm was followed. Forty percent of our patients took 12 weeks or more for wart clearance. These patients were also managed according to a local treatment algorithm. All four of these patients had high wart burden at presentation. This would reflect the findings reported by Wilson et al. 12 Furthermore, the SHAPE audit data revealed that 94% of the female patients took 12 weeks or less for wart clearance. This seems to suggest that patients with diabetes may take a longer time than patients without diabetes to clear their warts.
We investigated the number of visits patients took to achieve complete clearance of their warts and found 60% took three visits or less to completely clear their warts for that particular episode. The number of visits by patients who took more than 12 weeks to clear was not necessarily reflected in the number of visits as two of the patients were poor attenders and one patient had ulcerated and extensive warts, which needed surgical intervention. This also highlighted the popularity of home-based topical treatments in treatment choice of patients.
Patient 12 had extensive warts and was referred for surgical resection (Figure 1). She had a high body mass index with poor glycaemic control and this contributed to the secondary infection of the warts, which eventually became an ulcerated mass (Figure 2). She was deemed a high anaesthetic risk due to various other co-morbidities. This patient experienced significant pain as a consequence of her warts and needed specialist pain control input. We initiated treatment with topical imiquimod. Biopsy of the ulcerated mass confirmed the presence of HPV type 6. In view of this finding, we offered her Gardasil® vaccine in an attempt to stimulate an immune response. She underwent partial surgical debulking of her warts. Histology from the segments concluded the presence of giant perianal condyloma with focal moderate epithelial dysplasia (anal intraepithelial neoplasia grade II).

Ulcerated and infected perianal warts extending up to the anal verge
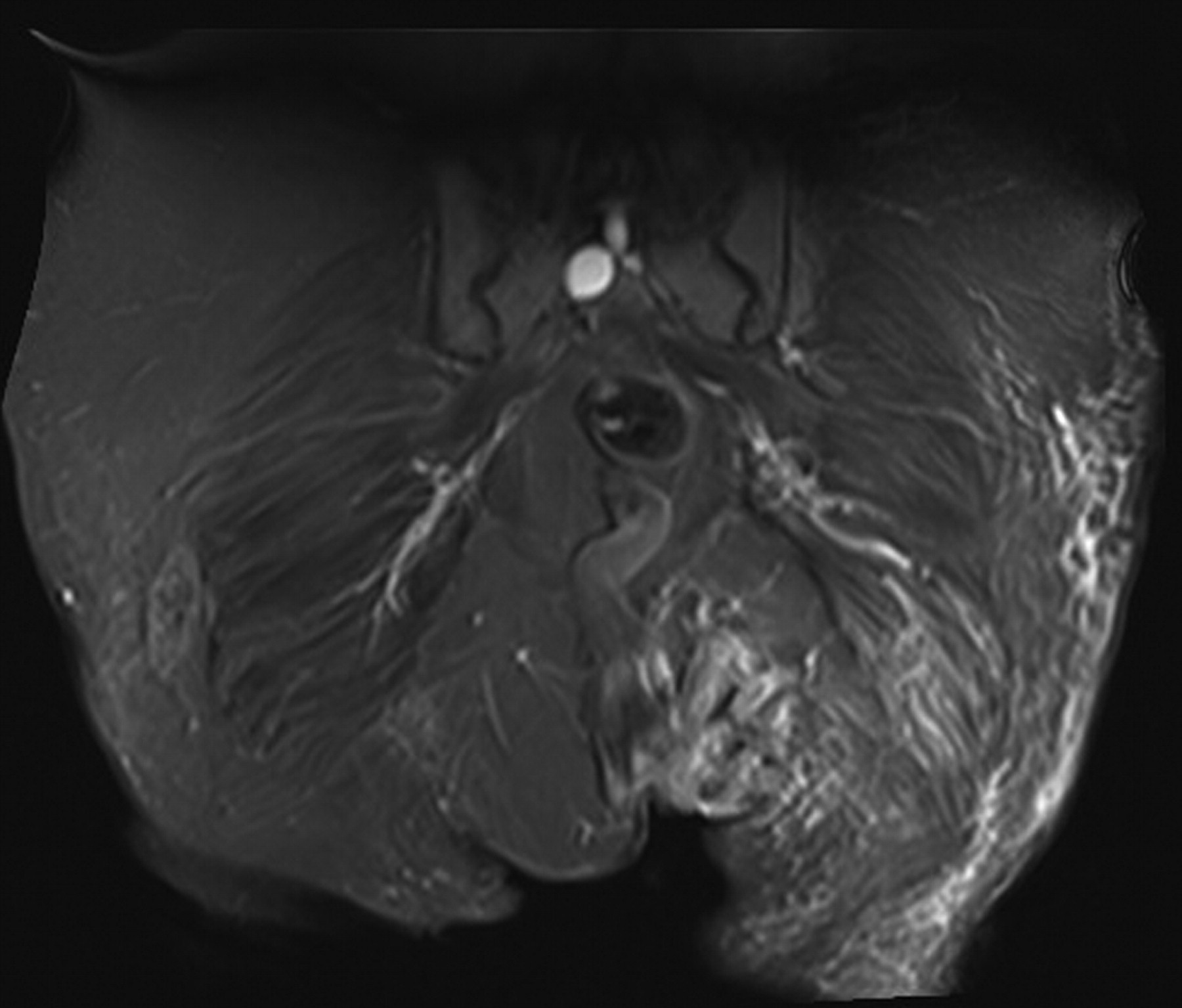
Magnetic resonance imaging of pelvis shows an abnormal area on the left vulva extending from the left labium majorum around the anus and towards the coccyx: this represents an infected site
The patient subsequently underwent a major operation to have a defunctioning colostomy as her residual warts were just too extensive and required a major flap surgery. Owing to poor glycaemic control, the area was slow to heal and she required prolonged periods of inpatient admission. The cost of managing her HPV 6 infection so far has been £85,000, and if the warts are ever cleared she will need further admission for a stoma reversal.
CONCLUSION
Although the number of patients with diabetes in our study is small, these data suggest that these patients did worse than the patients without diabetes. They had more extensive disease, required more treatments, had more recurrences and in some cases the warts lasted for a prolonged period of time.
It is accepted that even in patients without diabetes, warts can be recalcitrant and may occasionally require surgical intervention, but the presence of diabetes increases an individual's risk of having more complications postsurgery and in patient 12's case it was not just a simple wart resection.
The quadrivalent vaccine Gardasil® was administered in an attempt to help stimulate an immune response in the hope that it may lessen or eliminate the risk of recurrence. To date, there is little evidence demonstrating the successful use of preventive vaccines being used therapeutically in the clearance of warts. However, there was a report in 2009 suggesting that women who have been treated previously for cervical, vulval or vaginal intraepithelial neoplasia or genital warts may benefit from receiving the quadrivalent vaccine. 13 A smaller study has suggested the effective use of vaccine in the treatment of high-grade vulval intraepithelial neoplastic lesions. 14
In the economic evaluation of determining the cost of genital warts treatment by Jit et al., 15 genital warts were costed at £134 per case. This cost was used to justify the choice of vaccine used for a national HPV vaccination programme. It seems clear that in certain groups of patients (such as those with DM), the cost for genital warts treatment might be higher.
The National HPV Vaccination Programme in the UK currently uses Cervarix™, which is a preventive vaccine for HPV types 16 and 18. There was some disappointment in sexual health circles as it was felt that this decision was short-sighted. 16 If Cervarix™ continues to be the chosen vaccine, we would suggest that Gardasil® should be considered for certain categories of patients (such as patients with DM) in both the school vaccination and the catch-up programmes. Relevant issues such as preconception planning and contraceptive advice in young women with DM are discussed in Diabetes Young Person's clinics and Diabetes Transitional Care clinics. These clinics would offer a unique opportunity to vaccinate these patients with the quadrivalent vaccine Gardasil® as opposed to the bivalent vaccine Cervarix™, if needed.