
Abstract
The objective was to determine the occurrence of four urethral pathogens in urine specimens from symptomatic men using transcription mediated amplification (TMA) assay. Urethral swab and urine specimens from 300 men presenting to a family practitioner were Gram stained and tested for Neisseria gonorrhoeae, Chlamydia trachomatis, Trichomonas vaginalis and Mycoplasma genitalium using three TMA assays respectively. Except for T. vaginalis, the other recognized pathogens viz. N. gonorrhoeae, C. trachomatis and M. genitalium were detected in significantly larger numbers of patients with urethral discharge than in those with burning on micturition (BOM). The overall prevalences were 16.7% for N. gonorrhoeae, 12.3% C. trachomatis, 8.0% T. vaginalis and 17.3% M. genitalium. With regard to microscopic evidence of urethritis, significant associations were found for N. gonorrhoeae and C. trachomatis, but not for M. genitalium and T. vaginalis. This study demonstrated that in symptomatic men attending family practice, M. genitalium and T. vaginalis are also important aetiological agents of urethritis and hence treatment strategies be they syndromic management or laboratory directed should cover for these causative agents. The microscopic diagnosis of urethritis may not be important for treatment strategies. The current syndromic treatment guidelines for developing countries including South Africa need modification.
Keywords
INTRODUCTION
Adult male urethritis is one of the commonest sexually transmitted diseases (STDs) and accounts for 60% of sexually transmitted infection (STI) presentations at health care facilities in Gauteng Province of South Africa. 1 At health care facilities in South Africa, syndromic management for STDs is widely practiced and the protocols for adult male urethritis with/without burning on micturition (BOM) are the administration of cefixime and doxycycline. Such a strategy caters for treating Neisseria gonorrhoeae and Chlamydia trachomatis. Information regarding the other causes of urethritis such as Mycoplasma genitalium is lacking for South Africa. Furthermore, in view of the widespread use of syndromic management of STIs, microscopy of the urethral smears is not used.
Guidelines for the syndromic management of STDs for controlling STIs in South Africa were first formulated in 1996 by the National Department of Health. 2 Formulating these guidelines requires knowledge of the aetiologies of the common clinical syndromes and antimicrobial susceptibility profile of the prevalent pathogens. 3
Rapidly advancing molecular detection methods have greatly contributed to establishing prevalence data for urethral pathogens. Many studies using commercial assays (Abbott-LCX, BD Probe Tec and Roche Cobas Amplicor) for the simultaneous detection of N. gonorrhoeae and C. trachomatis have been published from the developed countries. 4–6 Polymerase chain reaction (PCR) and realtime PCR assays for the detection of Trichomonas vaginalis and M. genitalium have been developed. 7–9 These assays are all based on the amplification of DNA using a DNA polymerase. However, transcription mediated amplification (TMA) assays have been shown to be highly sensitive and specific for the detection of sexually transmitted pathogens. 10,11 In this study, we have used TMA assays to determine the prevalence of urethral pathogens in urine specimens obtained from symptomatic South African men attending a family practice in Pretoria, Gauteng Province.
METHODS
Study population
Patients presenting to a family practitioner in Pretoria, South Africa, with urethral discharge and/or complaints of BOM were recruited. These were first-time attendees who did not receive antimicrobial therapy in the preceding month. The study was carried out between August 2007 and June 2008 and recruited patients gave verbal consent for participation.
Specimen collection
After a general examination, an endourethral swab specimen was taken from each patient for microscopic examination following Gram staining. Thereafter a first-catch urine sample was collected for TMA testing into a urine collection tube (Gen-Probe Inc, San Diego, CA, USA). The specimens were delivered to the laboratory within 24 hours.
Laboratory methods
Microscopic examination of Gram-stained smears was performed by two microscopists independently. In the case of discrepant results, the slide was read by a third microscopist. Urethritis was diagnosed when four or more polymorphonuclear leukocytes (PMNLs) were present per high-power field (hpf; ×1000 magnification). Five fields were read and the mean number of cells calculated. Urine samples were tested for N. gonorrhoeae and C. trachomatis using the APTIMA® Combo 2 assay (GenProbe Inc) and for T. vaginalis and M. genitalium using transcription-mediated amplification-based analyte-specific-reagent testing (GenProbe Inc) as described previously. 12,13 TMA values >30,000 relative light units (RLUs) were considered positive for T. vaginalis and >50,000 RLUs positive for M. genitalium. Purified nucleic acids from a laboratory T. vaginalis isolate and M. genitalium genome (ATCC G-37, 33530D) were used as positive controls in the research TMA assays.
Data analysis
The specimens were grouped based on clinical and microscopic evidence of urethritis. Statistical analysis was performed using the χ 2 test to determine whether there was any relation between two categorical variables.
Approval to perform this study was obtained from the Medical Research and Ethics Committee (MCREC) of the University of Limpopo (Medunsa Campus): MCREC/P/85/2007:PG.
RESULTS
When 300 specimens were collected from consecutive symptomatic male patients, the study was stopped. Of these, 94 were from patients with visible urethral discharge and the remaining 206 patients complained of BOM without visible discharge on examination. Patients' ages ranged from 19 to 64 years old, with a mean of 37 years.
Overall, one or more pathogens were detected in a total of 138 (46%) patients. M. genitalium was the most frequently detected pathogen, 52 (17.3%), followed by N. gonorrhoeae, 50 (16.7%); C. trachomatis, 37 (12.3%); and T. vaginalis, 24 (8.0%). Single infections were seen in 110 (36.7%) of the specimens with M. genitalium the most common, 37 (12.3%), followed by N. gonorrhoeae, 29 (9.7%); C. trachomatis, 26 (8.7%); and T. vaginalis, 18 (6.0%).
Microscopic evidence of urethritis was seen in a total of 54 patients; 35 (37.7%) from patients with discharge (n = 94) and 19 (9.7%) from those with BOM only (n = 206).
The breakdown of pathogens based on clinical symptoms is shown in Figure 1. A single pathogen was detected in 61 of the 94 (64.9%) patients with discharge. N. gonorrhoeae only was detected in 27 (28.7%) of these, followed by M. genitalium only 17 (18.1%), C. trachomatis 13 (13.8%) and T. vaginalis four (4.3%). Mixed infections were seen in 17 (18.1%) patients, with a dual infection with N. gonorrhoeae and M. genitalium the most frequent (7; 7.5%), followed by N. gonorrhoeae and C. trachomatis (5; 5.3%). Among the 206 patients without discharge, single infections were seen in 49 (23.8%). M. genitalium only was detected most frequently 20 (9.7%), followed by T. vaginalis 14 (6.8%), C. trachomatis 13 (6.3%) and N. gonorrhoeae two (1.0%). Mixed infections were seen in 11 (5.3%). There were significant differences for the detection of N. gonorrhoeae, C. trachomatis and M. genitalium but no significant difference for T. vaginalis detection between the two groups. Mixed infections were also significantly more seen in the group with discharge.

Pathogens detected according to symptoms (n = 300). *With or without BOM; †denotes single infections. a P < 0.0001; b P = 0.03; c P = 0.9; d P = 0.04; e P = 0.001; f P < 0.001. BOM = burning on micturition
Figure 2 shows the pathogens in relation to microscopic evidence of urethritis. Only N. gonorrhoeae and C. trachomatis were significantly associated with microscopic evidence of urethritis.
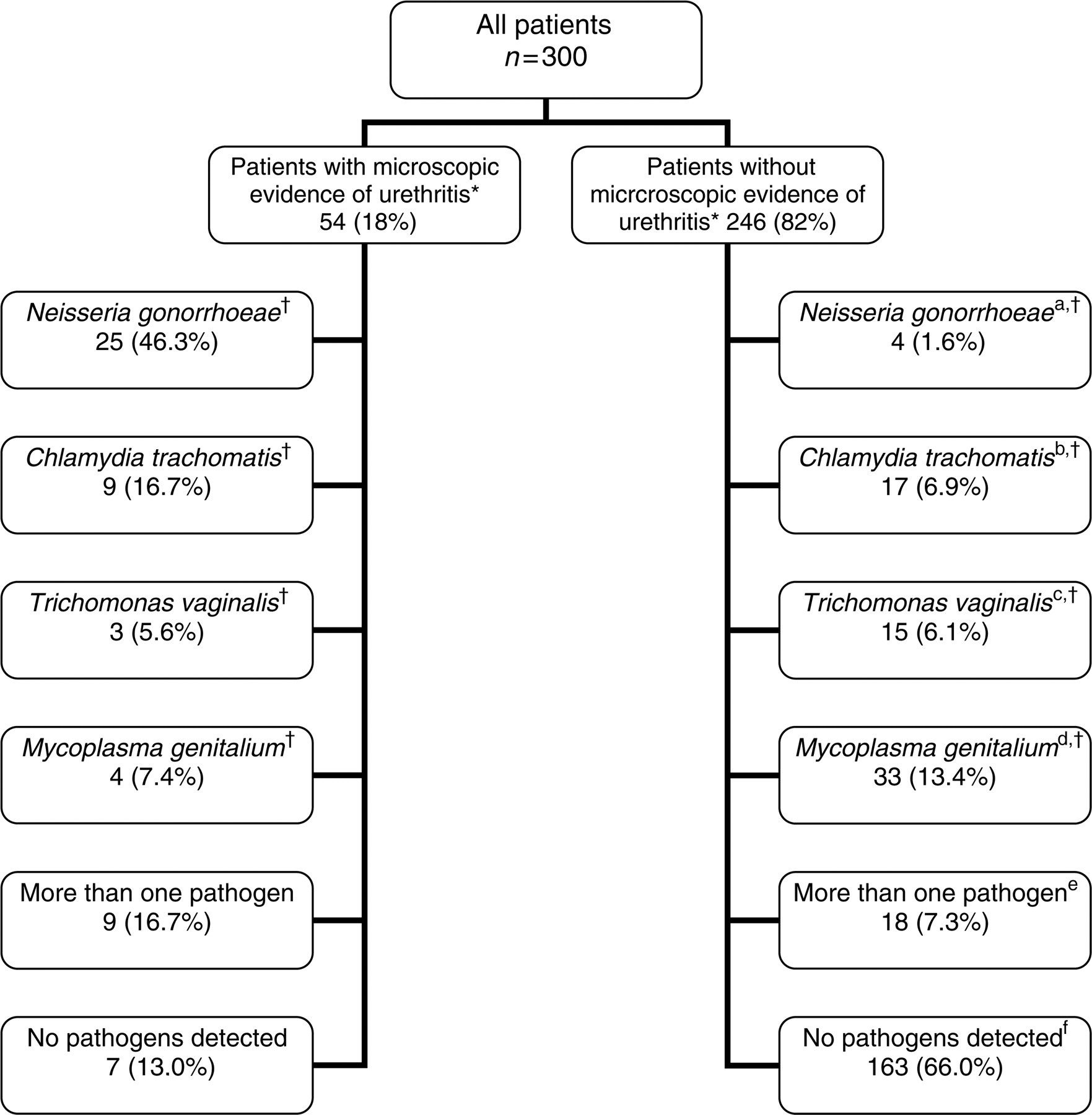
Pathogens in relation to microscopic evidence of urethritis (n = 300). *>4 PMNLs/hpf; †single infections. a P < 0.0001; b P = 0.02; c P = 0.8; d P = 0.2; e P < 0.02; f P < 0.001. PMNL = polymorphonuclear leukocyte
Mixed infections were seen in 9.3% (28/300) of all the specimens. It was significantly more in those with discharge (17/94; 18.1%) than in those with BOM only (11/206; 5.3%). The most common mixed infection was with N. gonorrhoeae and M. genitalium (11/300; 3.7%), followed by N. gonorrhoeae and C. trachomatis (6/300; 2.0%).
DISCUSSION
This study evaluated urethral pathogens according to urethritis based on clinical signs and symptoms and urethritis based on microscopic evidence. N. gonorrhoeae, C. trachomatis and M. genitalium were detected significantly more in men with urethral discharge, while only N. gonorrhoeae and C. trachomatis were significantly more associated with urethritis based on microscopy. There was no significant difference for the detection of M. genitalium or T. vaginalis whether there was microscopic evidence or not. This is contrary to European studies where M. genitalium has been shown to be associated with microscopic evidence of urethritis. 14 N. gonorrhoeae causes florid signs and symptoms with patients presenting with complaints of urethral discharge 15 while non-gonococcal urethral pathogens produce fewer symptoms and hence infected persons may not present with complaints.
The number of patients with discharge and symptoms of urethritis who had >4 PMNLs/hpf was low. This could be due to a number of factors. This study recruited men attending a family practitioner unlike other studies that recruit men attending genitourinary/STD clinics. 16,17 Furthermore, a significant number of the male population in South Africa consists of migrant workers from rural areas and visit health care facilities prior to them returning to their spouses (unpublished data). There could be other causes of urethral symptoms and it has been shown that in a fair number of symptomatic men no recognized pathogen is detected. 18 In a study by Bradshaw et al. 19 it was shown that 38% and 44% of men infected with adenovirus and herpes simplex virus (HSV), respectively, had fewer than 5 PMNLs/hpf.
In developing countries including South Africa health care practitioners have neither the time nor the skills to define urethritis based on microscopy, and use symptoms for diagnosis and treatment. This is shown by the syndromic management protocols. 2 As shown in this study, if microscopy was used as the only criteria for diagnosis, many T. vaginalis and M. genitalium infections would have been missed. The value of the Gram-stained urethral smear for the management of men with urethritis has been shown to be of limited value 20 and we concur with this finding.
In keeping with the findings of many studies from developed and developing countries, there is a high burden of urethritis pathogens among men presenting with urethritis, be it a discharge or BOM. M. genitalium was the commonest pathogen detected (17.3%) from all patients studied and was found in higher percentage of men with non-gonococcal urethritis than C. trachomatis. As expected, among men with visible discharge, N. gonorrhoeae was the most frequently (44.6%) detected pathogen. Despite the use of the sensitive TMA assays employed in this study, no pathogen was detected in 57% of all patients studied. However, it must be emphasized that we did not test for other possible less likely causes of urethritis, e.g. genital HSV and ureaplasmas.
Urine collected in the GenProbe tubes proved to be an easy specimen to work with. The urine is stable for 28 days at room temperature, and can be used to test for all four pathogens. The TMA assays make use of magnetic beads and a target capture system before amplification to exclude inhibition, eliminating the incorporation of individual amplification controls. 21 However, a study by Jang et al. 22 has shown that inhibition may still occur, albeit in a small proportion of patients (≤1%), compared with about 12% by the Cobas Amplicor assay. Their study was performed on women, and it has been reported that urine inhibition plays a bigger role in urine specimens from women than in men, especially for the testing of N. gonorrhoeae. 23,24
The GenProbe Aptima assays for the detection of N. gonorrhoeae and C. trachomatis in urine specimens have been evaluated and compared with other commercial assays and showed high sensitivities and specificity. For C. trachomatis sensitivities and specificities ranged from 92.1% to 100% and 98.9% to 100%, respectively, and for N. gonorrhoeae 98.5% to 100% and 91.3% to 100% respectively. 10,25–27 Sensitivity and specificity of the TMA assay for detection of T. vaginalis have been reported as 98.6% and 99.1% with the TMA assay identifying more positives than PCR, indicating that the TMA assay may be more sensitive. 28 TMA was also shown to be a reliable test for detecting M. genitalium in urine specimens. Wroblewski et al. 29 showed a 96% agreement between PCR and TMA in urine specimens from men. Hardick et al. 13 reported sensitivity of 100% and specificity of 97.9% when using TMA to test for M. genitalium in male urine samples, indicating the usefulness of this assay to test for male urethal pathogens in urines.
Only a few studies on the aetiology of male urethritis which included M. genitalium have been done in South Africa. 16,17,30 In all these studies, N. gonorrhoeae and C. trachomatis were the most frequently isolated pathogens. In our study, N. gonorrhoeae was only detected in 16.7% of all patients, which is much lower than that in the above-mentioned South African studies (47.2% to 62.3%). However, in patients with urethral discharge N. gonorrhoeae was detected as sole pathogen in 28.7% and in total in 44.6% of patients in our study, a prevalence similar to that found in the other South African studies. In previous studies in Pretoria, N. gonorrhoeae was found in 39.0% and 44.7% of men with urethritis. 18,31 Furthermore, it ought to be noted that in the current study the number of patients with visible discharge was smaller than those with symptoms of only BOM.
C. trachomatis only was detected in 13.8% of patients with discharge, and in 12.3% of all patients which falls in the same range as shown by the other South African studies (7.7–19.3%). In the 1996 STD review by Pham-Kanter et al. 32 prevalences of 12–13% were reported. These studies used various diagnostic methods such as antigen detection and culture for diagnosing chlamydial infection while our study used the TMA assay.
T. vaginalis was seen more frequently in this study at 8.0% overall, and alone at 6.0% compared with 4.9–6.0% in other studies. M. genitalium, the most commonly detected pathogen in all patients in this study, was also more prevalent (17.3%) overall and as single pathogen (12.3%) than that reported in the other South African studies (5.0–14.4%).
Multiple infections in men with urethritis have been reported previously in South Africa. 17,18,30 In this study, multiple infections were seen in 9.3% of patients, with a combination of N. gonorrhoeae and M. genitalium being the most common combination.
This study highlights the necessity of epidemiological studies of this nature for the proper understanding of the aetiology and management of adult male urethritis. The study by Djajakusumah et al. 33 demonstrates this most appropriately. Currently the syndromic management for adult male urethritis in our country consists of a single dose cefixime (400 mg, oral) and a seven-day course of doxycycline (100 mg twice daily, oral). Although doxycycline is the antibiotic of choice for the treatment of C. trachomatis, it has become apparent that M. genitalium often persists in the urethra of infected men after treatment. 34 Azithromycin as a single dose has become the antimicrobial of choice for the treatment of male urethritis in some countries. 35 However, Jensen et al. 36 have shown the emergence of resistance of M. genitalium to azithromycin, and advocate a longer treatment duration.
In clinical settings such as ours where microscopy is not used at all for the management of adult male urethritis, this study has shown that the treatment of patients with BOM should be re-visited. In patients with visible urethral discharge the current therapeutic regimen is appropriate. Although T. vaginalis infection will not be covered, its prevalence is lower than that of the other pathogens. However, for patients presenting with BOM and absence of discharge, the administration of a long course azithromycin plus metronidazole would be appropriate as this combination will cover the commoner pathogens such as M. genitalium, C. trachomatis and T. vaginalis. Such a regimen should be cost-effective and prevent the development of antimicrobial resistance by removing selective pressure.
Footnotes
Acknowledgements
The authors wish to thank Z Adams for assisting in specimen collection and Yusuf Dangor and Marie de Jongh for assisting with microscopy.