
Abstract
In order to discriminate general from aetiology-specific risk factors for immune reconstitution inflammatory syndrome (IRIS), we followed up, during six months, 99 patients with advanced HIV infection commencing antiretroviral therapy (ART) without active opportunistic infections or evident inflammation. IRIS predictors were determined by univariate analysis using clinical data from 76 ART-responding patients either completing follow-up or developing IRIS, and by multivariate analysis of inflammation, disease progression and nutrition status variables. We identified 23 primary IRIS events (30.3%). Univariate predictors for all IRIS events were higher platelet counts and lower CD4/CD8 ratio, whereas subclinical inflammation was the multivariate predictor. Platelets, alkaline phosphatase levels and %CD8 T-cells in univariate analysis also predicted mycobacteria-associated IRIS independently, remaining elevated during follow-up. Herpesvirus IRIS was predicted by platelets and inflammation. Indicators of advanced HIV disease and subclinical inflammation jointly predict IRIS, and some are specific of the underlying microbial aetiology, possibly explaining previous reports.
INTRODUCTION
Immune recovery of patients with HIV by highly active antiretroviral therapy (ART) can be accompanied by clinical deteriorations jointly termed immune reconstitution inflammatory syndrome (IRIS). 1 Since IRIS can be severe, life-threatening or fatal, 1,2 it is of great importance to identify its risk factors. Numerous risk markers have been reported, 1,3–14 but their diversity precludes their generalization, as well as assessing their possible role in IRIS pathogenesis. There are several possible causes of this diversity. Attention has been paid to the heterogeneity of IRIS case definitions, and efforts have been made to eliminate this source of bias. 15,16 However, it is also possible that different IRIS instances are determined by different risk factors, which would make their identification dependent on the prevalence of particular IRIS-associated aetiologies in the studied population.
Many of the reported risk markers can be grouped either as indicators of HIV disease progression, or as indicators of underlying infections and immune responses to them. Such is the case of low CD4 T-cell counts, increased viral loads, 3,4,6–10,13,14,17 starting ART less than two months after treating opportunistic infections or the presence of active infection. 4,5,7,11,13,18 Therefore, in this study we aimed at determining if different variables associated with HIV disease progression or with subclinical inflammation may jointly predict IRIS in a cohort of patients with advanced stage HIV infection who initiate ART. We also determined if some risk markers could differentially predict IRIS instances with particular underlying aetiologies.
In order to avoid the biases of retrospective studies, 19 we identified IRIS cases and IRIS-free controls by prospective follow-up.
METHODS
ART cohort and follow-up
A prospective longitudinal observational study was conducted with a cohort of 99 HIV+ ART-naive adults (>18 years) who reached the recommendation for antiretroviral treatment (ART) initiation according to the contemporary International Guidelines 20,21 (with either >350 CD4 T-cells/μL blood in the presence of symptomatic disease or <350 CD4 T-cells/μL blood regardless of symptoms) at the National Institute for Respiratory Diseases in Mexico City. Patients complying with these inclusion criteria were recruited if they did not show evident inflammatory processes, if they were already at the maintenance phase of successful antituberculous treatment (see below) or had experienced positive clinical response to treatment of other opportunistic infections, like cytomegalovirus retinitis or Pneumocystis jirovecii pneumonia. Active tuberculosis was ruled out in patients recruited after hospitalization if the following criteria were met: resolution of fever, cough, sputum and dyspnoea, plus improvement of opacity, nodules, cavitation and pleural effusion as shown by chest X-ray examination, as well as resolution of lymph node enlargement (cervical, axillary and inguinal), and absence of thoracic rales and dullness to percussion under physical examination. All these symptoms had to be absent in patients recruited without previous hospitalization.
Follow-up visits were scheduled at baseline (on the day of ART initiation), and on weeks 4, 8, 12, 24, 39, 52 and 104 after ART initiation. Additionally, for more accurate determination of onset times, and avoidance of underreporting, unscheduled visits took place if a patient presented signs of IRIS before a scheduled visit. For the present study, data from the whole 24-week follow-up were used, at the time when all participants had reached it. During each visit, patients underwent a comprehensive clinical evaluation by attending physicians, and blood samples were drawn for routine laboratory analyses including CD4 T-cell and CD8 T-cell counts (TriTest kit, FACSCalibur system, Becton Dickinson, San José, CA, USA), and plasma viral loads (Cobas Amplicor-PCR-Monitor HIV-1 system, Roche Diagnostics, Indianapolis, IN, USA), for the whole duration of the follow-up. Blood chemistry, complete blood count and liver function were evaluated during the 24-month follow-up. Additionally, baseline determinations of C-reactive protein, erythrocyte sedimentation rate and chest radiography were performed at week 0. Clinical evaluation included relevant clinical data and findings allowing the identification of IRIS (see IRIS definition below), which were recorded using standardized Case Report Forms. Deviations from the scheduled follow-up time of no more than 10% (3 days for the 4-week visit, 6 days for the second visit, 9 for the third and so forth) were permitted. This was required for inclusion of the data in the cohort.
Study population
To assure detection of symptoms clearly appearing after treatment initiation, a study population was defined, consisting of individuals not showing the following exclusion criteria: baseline inflammatory processes made evident later by initial laboratory studies (active hepatitis), not showing satisfactory response to ART; namely, those not showing a sustained decrease in viral load of at least 1 Log units, 22 not reaching less than 200 HIV RNA copies/mL blood at week 24, and receiving immunomodulatory drugs. This study population was used for all reported analyses, and excludes worsening IRIS cases, leaving only unmasking ones. Further, when physicians did not agree on whether a clinical event constituted IRIS using the case definition, the corresponding case was excluded to avoid misclassification.
IRIS definition
Differences in case definitions are a possible source of discrepancies between studies. 15,16 Since the present study comprised different identifiable IRIS cases, and consensus work definitions are available only for particular instances, 15 we focused on the concurrent points among the main reported definitions 6,9,10,15,,16,23 : appearance or worsening of an inflammatory condition or an AIDS defining illness, that the event is not attributable to newly acquired infections or drug side-effects, and that, given a satisfactory response to highly active antiretroviral therapy (HAART) the condition is attributable to immune reconstitution. Thus, IRIS was defined as the appearance of signs or symptoms consistent with inflammation, appearance of new opportunistic infections or worsening of previously controlled ones during satisfactory ART. The symptoms could not be attributed to a newly acquired opportunistic infection, according to clinical antecedents and to contemporaneous CD4 T-cell counts, nor to known drug side-effects. This definition and the characteristics of the study population targeted mainly the identification of unmasking IRIS cases. Agreement of physicians participating in this study (at least 3 persons of which 2 consistently participated in all decisions) was necessary to classify a patient as an IRIS case.
Statistical analysis
We examined four different response variables for IRIS, each one consisting of groups of related aetiologies: all IRIS cases, mycobacterial-related IRIS, herpesvirus-related IRIS and other dermatological IRIS. The aetiologies comprised by each response variables were:
Mycobacteria-related IRIS: Mycobacterium tuberculosis (MTB), Mycobacterium avium complex (MAC); Herpesvirus-related IRIS: Herpes zoster, herpes simplex, cytomegalovirus, Kaposi's sarcoma; Other dermatological manifestations (microbiologically unrelated): Molluscum contagiosum and folliculitis. Underlying inflammation: Serum albumin, leukocyte, lymphocyte, and platelet count, C-reactive protein, lactate dehydrogenase and alkaline phosphatase (ALP); Nutritional status: Albumin, haematocrit, haemoglobin, cholesterol, triglycerides, body mass index (BMI); HIV disease progression: CD4 and CD8 T-cell counts, %CD4+ and %CD8 T-cells, CD4/CD8 ratio, HIV viral load.
To account for the fact that standard laboratory variables may be highly correlated, some measure different aspects of the same biological process, or some are function of others, we defined sets of predictive variables for multivariate logistic models as follows:
For each of the response variables (aetiology groups) and each set of predictor variables, we carried a backward stepwise strategy based on the resulting Akaike information criteria (AIC). We report the lowest AIC scoring model and the independent univariate predictors. Only significant predictors are reported. All statistical analyses were carried out with R statistical environment 2.8.0, using Package Design version 2.1–2. 24 IRIS predictors were compared between patient groups at different treatment time points using either Mann-Whitney test for two-group comparisons or Kruskal-Wallis test for three-group comparisons.
RESULTS
IRIS clinical presentations and frequency
Between July 2005 and October 2008, the complete cohort of 99 patients was recruited, initiated HAART and was followed up for at least six months, which was used as cut-off time for analysis. (At this time 26 patients had finished the complete 104-week follow-up.) Twenty patients were excluded (6 due to thalidomide intake as part of co-participation in another study, 5 due to poor treatment response, 3 patients had baseline active hepatitis later revealed by laboratory analyses and 6 were lost to follow-up). Three of the remaining 79 patients could not be classified due to a lack of consensus among attending physicians and were thus excluded for final analysis. This left a study population of 76 patients reaching a follow-up of six months (76.8% of the original cohort), with three patients (3.9%) dying from a condition identified as IRIS before six months (Figure 1, Table 1). The male/female proportions found in the initial cohort and in the study population were characteristic of the Mexican AIDS epidemic,
25
with a high percentage of males, which makes the results potentially different from those populations with a larger female population.
Summary of patient recruitment and disposition. ART= antiretroviral therapy; IRIS = immune reconstitution inflammatory syndrome Demographic and clinical characteristics of the study population, consisting of ART-responding HIV+ patients among which IRIS could be identified unequivocally IQR= interquartile range; VL = viral load; PCP = Pneumocystis jirovecii pneumonia; MAC = Mycobacterium avium complex; CMV = cytomegalovirus; NRTI = nucleoside analogue reverse transcriptase inhibitor; EFV = Efavirenz; PI = protease inhibitor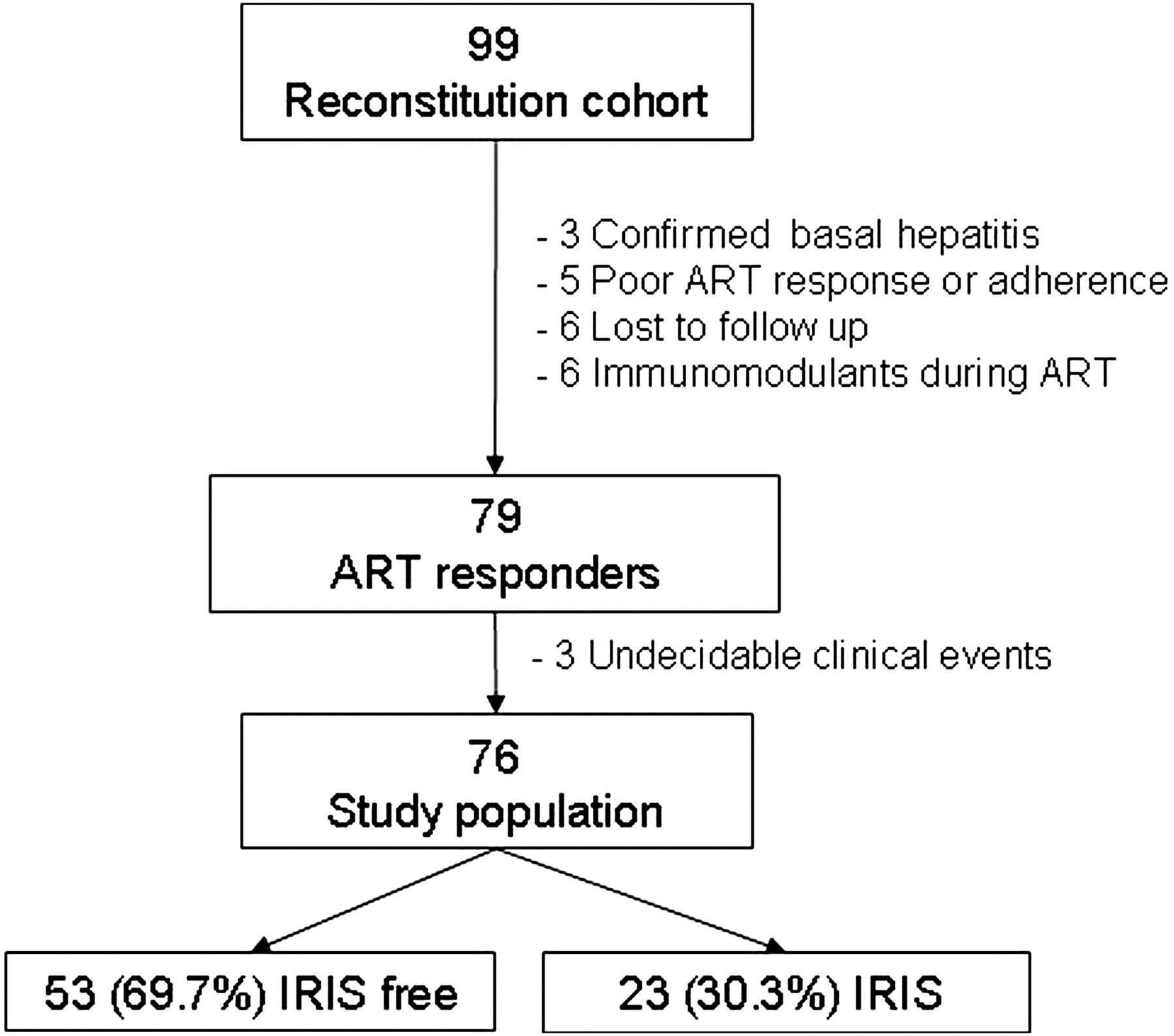
Twenty-four IRIS events were identified in 23 patients, constituting 30.3% of the study population. Median onset time was 47 days (interquartile range 28–56). Of the six tuberculosis cases, one was pulmonary (cough, fever, diaphoresis, hiliar opacity), two meningeal (headache and fever in both, one showing positive cerebrospinal fluid [CSF] polymerase chain reaction [PCR] for MTB, the other with vomiting, weakness of pelvic limbs and death after cerebral vasculitis), two cases with painful lymph node enlargement (MTB-positive) and one disseminated tuberculosis (abdominal pain, lowered peristalsis and gut perforation upon laparotomy, MTB-positive sputum and bone marrow). Only the disseminated TB IRIS and the deceased meningeal case had pre-ART active (pulmonary) tuberculosis. The meningeal case had multidrug-resistant MTB, with culture-negative sputum at baseline and culture and PCR-negative CSF. Two cases of MAC-associated IRIS manifested as cervical lymphadenopathy (culture positive) with pain and fever, and two as disseminated MAC with pulmonary involvement and culture-positive bone marrow (one with fever, the other with dyspnoea, white sputum and nausea); MAC antecedents. Three cases developed herpes simplex virus IRIS: two with cutaneous herpes simplex and one retinal necrosis consistent with herpes simplex virus. Three patients developed retinitis consistent with cytomegalovirus while receiving valganciclovir started before ART. Pre-ART antecedents were one CMV pneumonitis, and two CMV retinitis cases. One case of Kaposi's sarcoma consisted of a 2 cm diameter lesion on the hard palate without pre-ART antecedent lesions. Of three folliculitis cases, one was diagnosed as Malassezia sp. folliculitis by histopathology, one as suppurative and the other as superficial eosinophilic.
Grouping the associated aetiologies, 10 IRIS cases (41.7%) were related to mycobacteria (MTB, MAC, with 1 patient presenting both), nine (37.5%) with a herpesvirus (cytomegalovirus, herpes simplex virus, herpes zoster virus and Kaposi's sarcoma-associated herpesvirus) and the remaining five cases (20.8%) consisted of diverse unrelated dermatological manifestations (molluscum contagiosum and folliculitis). All 76 patients showed satisfactory response to ART, including an increase in CD4 T-cell counts, with no significant differences in viral load or CD4 T-cell counts between patients developing IRIS and IRIS-free patients at any time (Figure 2a and b).
Satisfactory response to combined (highly active) ART in the two groups comprising the study population. (a) Viral load throughout follow-up. (b) CD4+ T-cell recovery during follow-up. Points and error bars represent mean ± SEM. Groups were compared using Mann-Whitney test. ART= antiretroviral therapy; IRIS = immune reconstitution inflammatory syndrome
IRIS risk factors
Clinical variables predicting IRIS in the study population
AIC= Akaike information criteria for multivariate models in logistic regression; Plat= blood platelet count; CRP= C-reactive protein; Lym = blood lymphocyte count; ALP = blood alkaline phosphatase levels; Alb = serum albumin concentration; Trig = serum triglycerides; BMI = body mass index; Hb= haemoglobin; Hcri = haematocrit; OR = odds ratio; CI = confidence interval; IRIS= immune reconstitution inflammatory syndrome
Predictor sets correspond to conditions to which variables in the models are related
Patients were grouped either according to whether they had presented any IRIS manifestation or not, or according to groups of IRIS-related aetiologies (herpesviruses, mycobacteria or other dermatological instances) or no IRIS
CD4 T-cell counts were not predictive of IRIS. However, other variables related with HIV disease progression, CD4/CD8 ratio and %CD8 T-cells were predictive of IRIS. While CD4/CD8 ratio independently predicted occurrence of any IRIS instance, %CD8 T-cells was an independent specific predictor of IRIS instances associated with mycobacteria.
The two mycobacterial IRIS-specific predictors, %CD8 T-cells and ALP levels, were dependent. A model with ALP and %CD8 T-cells was a very good predictor of mycobacteria-associated IRIS (R 2 = 0.43, P = 0.00028, in contrast with R 2 = 0.167 for ALP alone, and R 2 = 0.35 for %CD8 T-cells alone, not shown). Mycobacteria-associated IRIS was also predicted by a model using several variables related with nutrition status: serum albumin, triglycerides, BMI, haemoglobin and haematocrit, none of which was able to predict IRIS independently.
Individually predictive variables over time are shown in Figure 3. Platelet counts were significantly different between patients who develop IRIS and IRIS-free patients at baseline (P = 0.0042), and four weeks after ARV treatment initiation (P = 0.0207), followed by a sustained tendency to higher platelet counts in patients developing any IRIS (Figure 3a). A similar tendency was seen in the CD4/CD8 ratio, albeit with no significant difference between groups (Figure 3b). Notably, %CD8 T-cells were significantly higher in mycobacterial IRIS patients than in patients with other IRIS or no IRIS at all follow-up points (P = 0.0095 week 0, P = 0.0035 week 4, P = 0.0234 week 8, P = 0.0063 week 12, P = 0.0063 week 24, Figure 3c), and ALP levels were higher in mycobacteria-IRIS group at weeks 0 and 12 (P = 0.0184, P = 0.0341 correspondingly), tending to be higher at all other times (Figure 3d).
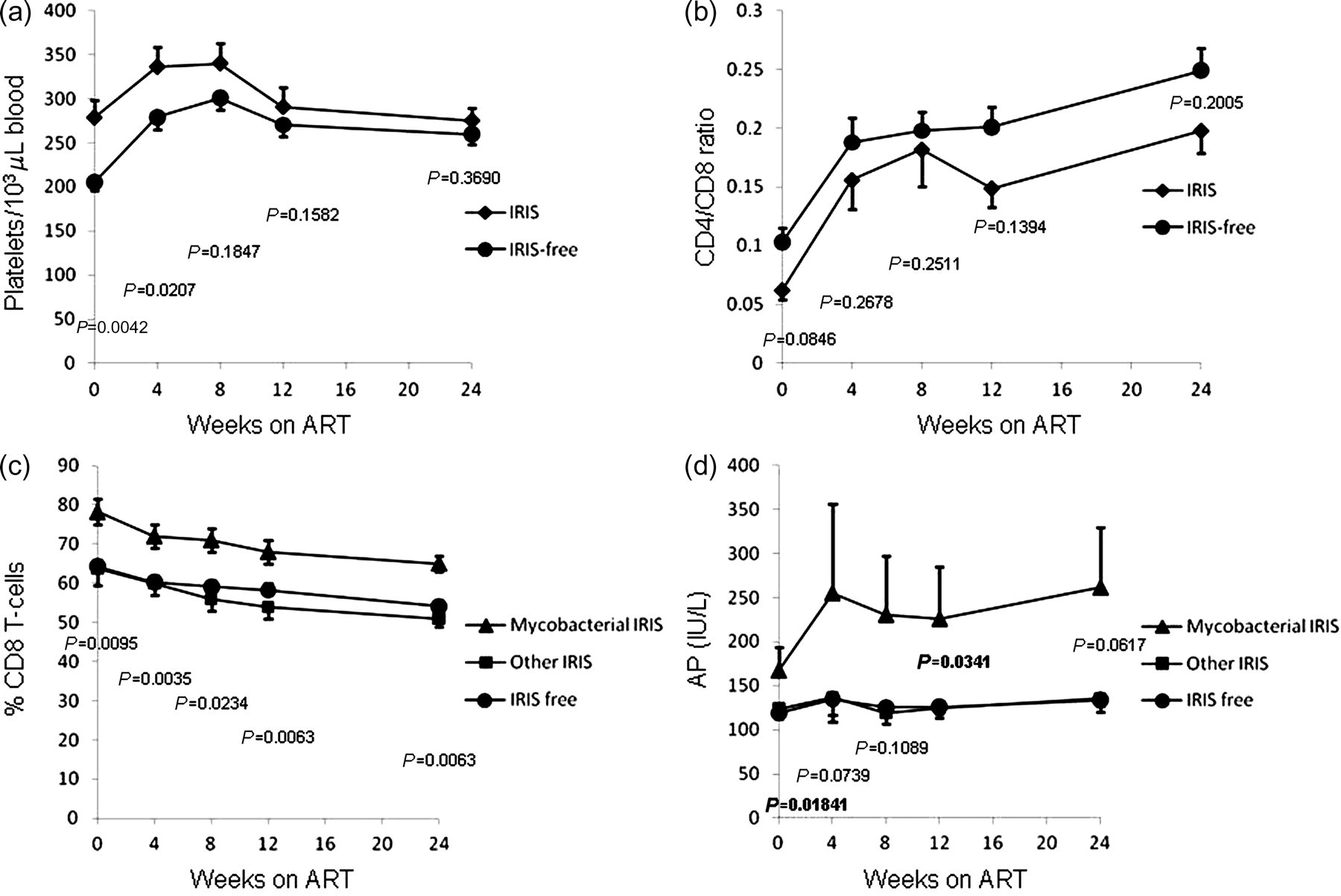
Development of IRIS-predictive variables during follow-up (mean ± SEM), in different subsets of the study population, defined according to the predictive capacity of variables and IRIS-related aetiology. (a, b) Variables predicting any IRIS manifestation; groups were compared at each follow-up point using Mann-Whitney test. (c, d) Variables specifically predicting IRIS associated with mycobacterial infections; groups were compared using Kruskal-Wallis test. AP= alkaline phosphatase levels in blood; ART= antiretroviral therapy; IRIS = immune reconstitution inflammatory syndrome
DISCUSSION
Many of the IRIS risk factors so far reported are related to HIV infection progression, such as lower nadir CD4 count, CD4/CD8 ratio, 9 %CD4 T-cells 8,9,17 and higher baseline viral load. 4,6 The present cohort initiated HAART in an advanced stage of HIV infection (Figure 3). While CD4 T-cell count and viral load were not predictive, the relative proportions of CD4 and CD8 T-cells, reflected by CD4/CD8 ratio and %CD8, clearly predicted IRIS. Considering that they also indicate disease progression, our results agree with previous reports. 26
Other reported risk factors are related to the presence of the aetiological agent whose symptoms constitute the IRIS manifestation, like higher concentrations of antigen 6 or frequency of disseminated MTB, 4 fungemia 27 and incomplete control of the opportunistic pathogen at ART initiation. 5,11,13,18 Here, we found a predictive model that groups variables related with inflammatory processes: platelet and lymphocyte counts, blood C-reactive protein and ALP. Additionally, platelet counts were a consistent and strong independent predictor of all IRIS manifestations. Thus, the risk factors in the present study may reveal a common determining condition unifying previous findings; namely, underlying inflammatory responses to opportunistic infections later unmasked by immune reconstitution.
Percentage CD8 T-cells and blood ALP levels were very specific predictors of mycobacteria-associated IRIS. It is worth mentioning that some cohorts focus on single IRIS-associated aetiologies, 4,6,7,8,11,13,28–32 while others include diverse IRIS manifestations. 1,3,9,10,14,33 The latter would find aetiology-specific predictors only if their corresponding manifestations are sufficiently represented. Thus, some variables may be predictive depending on the particularities of a given cohort.
All predictors showed consistent tendencies to differ between risk groups during the whole follow-up, with %CD8 showing a sustained significant increase in the patients who developed mycobacteria-related IRIS. This not only rules out the possibility of circumstantial baseline differences, but also points to a causal link between these predictive variables and IRIS occurrence, a characteristic of risk factors. 19 In this regard, platelets, a general predictor with an expectable broader involvement, have been found to participate in the induction of diverse inflammatory phenomena. 34–41 Their increased presence, albeit within normal ranges, in people at significant risk of developing IRIS seems to be related to different subclinical inflammatory processes.
Interestingly, higher %CD8 T-cell predicts mycobacteria-associated IRIS independently of other variables, and remains significantly higher in the mycobacteria-related IRIS group during follow-up. This could be reflecting selective migration of CD4+ T-cells to inflammed tissues, as occurs in response to BCG 42 and in active tuberculosis. 43–45 Over representation of CD8+ T-cells among blood T-cells may again reflect pre-existing subclinical inflammation.
ALP levels, a specific risk factor for mycobacterial-IRIS, tended to remain higher during ART in people who developed mycobacteria-associated IRIS, with significance at month three. While this could be an effect of hepatotoxic medication (isoniazid, rifampicin, pirazinamide, etc.), increased serum ALP may originate in lymphocytes 46 or neutrophils 47,48 participating in the response to mycobacteria. 49 The aetiology specificity of some IRIS risk factors agrees with the view that different pathogenic mechanisms may underlie different IRIS manifestations. 50 They also suggest the possibility of scoring risk. However, given the relatively small size of the groups and the cohort, further inference based on multivariate logistic analysis will require the cautious study of a larger population.
In summary, prospective follow-up of a cohort of patients with advanced HIV infection allowed the identification of IRIS risk factors possibly revealing underlying subclinical inflammatory processes, some of which were specific to the aetiology associated with IRIS onset. This offers an explanation to the heterogeneity of reported IRIS risk factors.
Footnotes
ACKNOWLEDGEMENTS
Work funded by Grant P50478III from Consejo Nacional de Ciencia y Tecnología (Conacyt), Mexico, Comisión de Equidad y Género, Honorable Cámara de Diputados, Mexico, and Fundación México Vivo. We thank Claudia Escamilla and Susana Páez from the Clinical Laboratory of the National Institute for Respiratory Diseases for timely availability of data. EE and CEO contributed equally to this work.