
Abstract
The aim of this work was to survey current service provision and adherence to the British HIV Association (BHIVA) guidelines for the management of HIV and hepatitis B/C co-infected patients in the UK. Sites were invited to complete a survey of local care arrangements for co-infected patients. A case-note audit of all co-infected attendees during a six-month period in 2009 was performed. Data including demographics, clinical parameters, hepatitis disease status, antiretroviral and hepatitis B/C therapy were collected. Using BHIVA guidelines as audit standards, the proportion of sites and subjects meeting each standard was calculated. One-hundred and forty sites (75%) responded and data from 973 eligible co-infected patients were submitted. Approximately a third of sites reported not re-checking hepatitis serology or vaccination titres annually. Of all co-infected patients, 122 (13%) were neither vaccinated nor immune to hepatitis A and 26 (5%) of patients with hepatitis C were neither vaccinated nor naturally immune to hepatitis B. Of HBsAg-positive subjects, 25 (6%) were receiving lamivudine as the sole drug with antihepatitis B activity. In the UK, the management of HIV and hepatitis B/C co-infection remains highly variable. Optimizing the care of this high-risk patient group is a priority.
INTRODUCTION
Chronic infection with viral hepatitis B and C remains an important global cause of morbidity and mortality. It is estimated that there are currently over 350 million individuals chronically infected with hepatitis B (HBV) and 170 million with hepatitis C (HCV) worldwide. 1,2 In the UK, the current prevalence of HBV is approximately 0.3% and HCV 0.4%. 2,3
Due to their similar modes of transmission, HBV and HCV are highly prevalent in HIV-positive individuals. In different HIV populations and cohorts, reported rates of HBV/HIV co-infection vary between 6% in London, 4 9.1% in European clinics 5 and over 20% in Malawi. 6 The prevalence of HCV/HIV co-infection has been reported at 8.9% in UK clinics; 7 however, this varies according to an individual's risk-acquisition group, with particularly high rates observed in injecting drug users and recipients of contaminated blood products (e.g. men with haemophilia). Furthermore, in recent years there have been reports of HCV infection acquisition in HIV-infected men who have sex with men (MSM) linked to sexual transmission and associated with the use of non-parenteral recreational drugs. 8,9
Irrespective of transmission route, a diagnosis of HIV and HBV/HCV co-infection has major health implications and liver disease has emerged as an important cause of death in the combination antiretroviral therapy (cART) era. 10 Individuals with co-infection are at risk of accelerated liver disease progression to fibrosis and cirrhosis as well as an increased rate of hepatoma. In addition, they are at increased risk of drug hepatotoxicity that may complicate the successful administration of cART and other antimicrobial treatments. The Strategic Management of Antiretroviral Therapy (SMART) study recently demonstrated interrupting cART is associated with an increased incidence of clinical events and this risk is further enhanced for co-infected individuals. 11
In 2005, the British HIV Association (BHIVA) published separate guidelines on the management of HIV co-infection with HBV and HCV. 12,13 These guidelines were amalgamated and revised in 2010. 14 Such guidelines endeavour to offer recommendations, based on available evidence and expert opinion, with the intention of optimizing patient care. The aim of this work, therefore, was to describe care arrangements nationally and to audit adherence to 2005 BHIVA Guidelines audit standards and recommendations for the management of co-infected patients in the UK.
METHODS
Clinic survey
All UK sites known to BHIVA as providers of adult HIV services were included and an online survey sent to the clinical lead of HIV services at each site. The survey contained questions regarding the description of clinical site (outpatient department, HIV centre, other), the size of patient caseload and details of service provision for patients co-infected with HIV and hepatitis B/C.
Case-note audit
Sites were asked to complete a retrospective case-note review for consecutive eligible patients who attended HIV services between 1 April and 30 September 2009, up to a maximum of 25 per site. Eligibility criteria required subjects to be HIV-1 antibody positive adults (aged over 18 years) and HBsAg positive and/or HCV antibody positive. Subjects were excluded where the HIV diagnosis was before 1999, if hepatitis B/C infection had cleared before their HIV diagnosis was made, or if a hepatitis B/C polymerase chain reaction (PCR) test was negative at the time of their first positive serology, and was never subsequently positive.
Clinical information was submitted electronically. This included demographic details (gender, dates of HIV and HBV or HCV diagnoses, HIV-acquisition risk group), clinical parameters (current and first plasma CD4+ lymphocyte count, hepatitis serology and PCR test results, current hepatitis A/B vaccination status) plus details of current antiretroviral therapy and hepatitis B/C therapy.
Data were analysed using Microsoft Excel (2003). Selected recommendations from the 2005 BHIVA Guidelines 12,13 were assessed (Table 1), and the percentage of sites and subjects meeting each recommendation was calculated. Results for each clinical site were then stratified and returned to clinicians for local dissemination with colleagues.
Audit standards selected from 2005 BHIVA guideline recommendations
BHIVA = British HIV Association; HBV = hepatitis B virus; HCV = hepatitis C virus; cART = combination antiretroviral therapy; 3TC = lamivudine; FTC = emtricitabine
RESULTS
Clinic survey
Overall 140 (75%) of 186 UK sites providing HIV care completed a clinic survey. When asked to classify site-type, 68 (49%) selected HIV outpatient department, 59 (42%) HIV centre and 13 (9%) chose neither option. The majority (91%) of HIV outpatient departments had a patient caseload below 500 in contrast to HIV centres, where 44% had patient caseloads in excess of 500. Each site described how hepatitis treatment is provided for their patients. Overall, 47% of sites reported that HBV treatment is provided within their HIV unit and 30% refer patients to a regional hepatology/infectious diseases centre. By contrast only 20% of sites reported that HCV treatment is provided within the HIV unit, with the majority being provided in regional or local hepatology/infectious diseases centres. Thirty-three (24%) sites refer to joint HIV/hepatology clinics.
Overall, 71% and 66% of sites reported performing HBV and HCV serology at least annually in non-immune patients, respectively. Sixty percent of sites monitor anti-HBs titres annually in vaccinated patients. Clinicians from 15 (10%) sites reported restricted availability of HBV DNA, HCV RNA and/or HCV genotype tests and some such test(s) were unavailable at two (1%) sites.
Case-note review
Patient demographics
Data on 973 eligible HIV-positive patients were submitted; 498 (51%) were HCVAb-positive, 451 (46%) were HBsAg-positive and 24 (3%) were positive for both. Patient demographics and clinical parameters are shown in Table 2. Sixty-four percent of patients with HBV/HIV were men, 66% heterosexual and 32% MSM. By contrast, 79% of patients with HCV/HIV were men, 24% MSM and 32% current or former injecting drug user. Of all co-infected patients, 801 (82%) were receiving cART at the time of audit.
Patient demographics and clinical parameters of co-infected subjects in audit
HBV = hepatitis B virus; HCV = hepatitis C virus; IDU = past/current injecting drug user; MSM = men who have sex with men; cART = combination antiretroviral therapy
*Subjects with HBV and HCV are included in both categories
†Some totals do not sum to 100% due to missing data
Management of HBV and HCV co-infected patients
HBeAg status and HBV DNA testing had been assessed in 453 (95%) and 444 (93%) of HBV/HIV patients, respectively. Of 522 patients with HCV/HIV, 512 (98%) had had a HCV RNA test, but only 454 (87%) an HCV genotype. A liver biopsy had been performed in 205 (21%) of all co-infected patients and a non-invasive fibrosis assessment had been performed in a further 149 (15%).
A discussion regarding alcohol avoidance was documented in the case-notes of 489 (50%) of all patients (HBV 41%, HCV 58%) with the majority of discussions being within the past year. It was documented that partner notification had been initiated in 52% of cases and risk reduction had been discussed with 58%.
Of the co-infected patients included in the audit, 122 (13%) were reported as neither immune nor vaccinated to hepatitis A. Similarly, 26 (5%) of patients with HCV/HIV were reported as neither vaccinated nor naturally immune to HBV. A further 111 (22%) of HCV/HIV patients were considered by clinicians to be vaccinated against HBV, but not fully protected. Although date of hepatitis diagnosis was not known for all subjects, no association between recent hepatitis diagnosis and incomplete vaccination status was observed (data not shown). Of the 43 patients with known cirrhosis in this audit, 29 (67%) had had both liver ultrasound study imaging and alpha-foetoprotein (AFP) levels within the past year, four (9%) had imaging but not AFP, four (9%) had AFP but not imaging, and six (14%) had neither.
HBV treatment
Of 475 HBV/HIV patients, 413 (87%) were receiving HBV treatment at the time of audit (Figure 1). One subject was receiving cART without the inclusion of anti-HBV agents (ritonavir-boosted darunavir and raltegravir). Of the 62 HBV/HIV patients not receiving HBV treatment at the time of audit, 16 (26%) were HBeAg positive and 16 (26%) had high (>/104copies/mL) HBV DNA levels (8 subjects had both features). Three of these subjects had most recent plasma CD4 + cell counts below 200 cells/µL and 10 subjects between 200 and 350 cells/µL. Reasons given for non-treatment included assessment/referral in progress, patient decision, poor clinic-attendance, therapy adherence problems and therapy considered unnecessary.
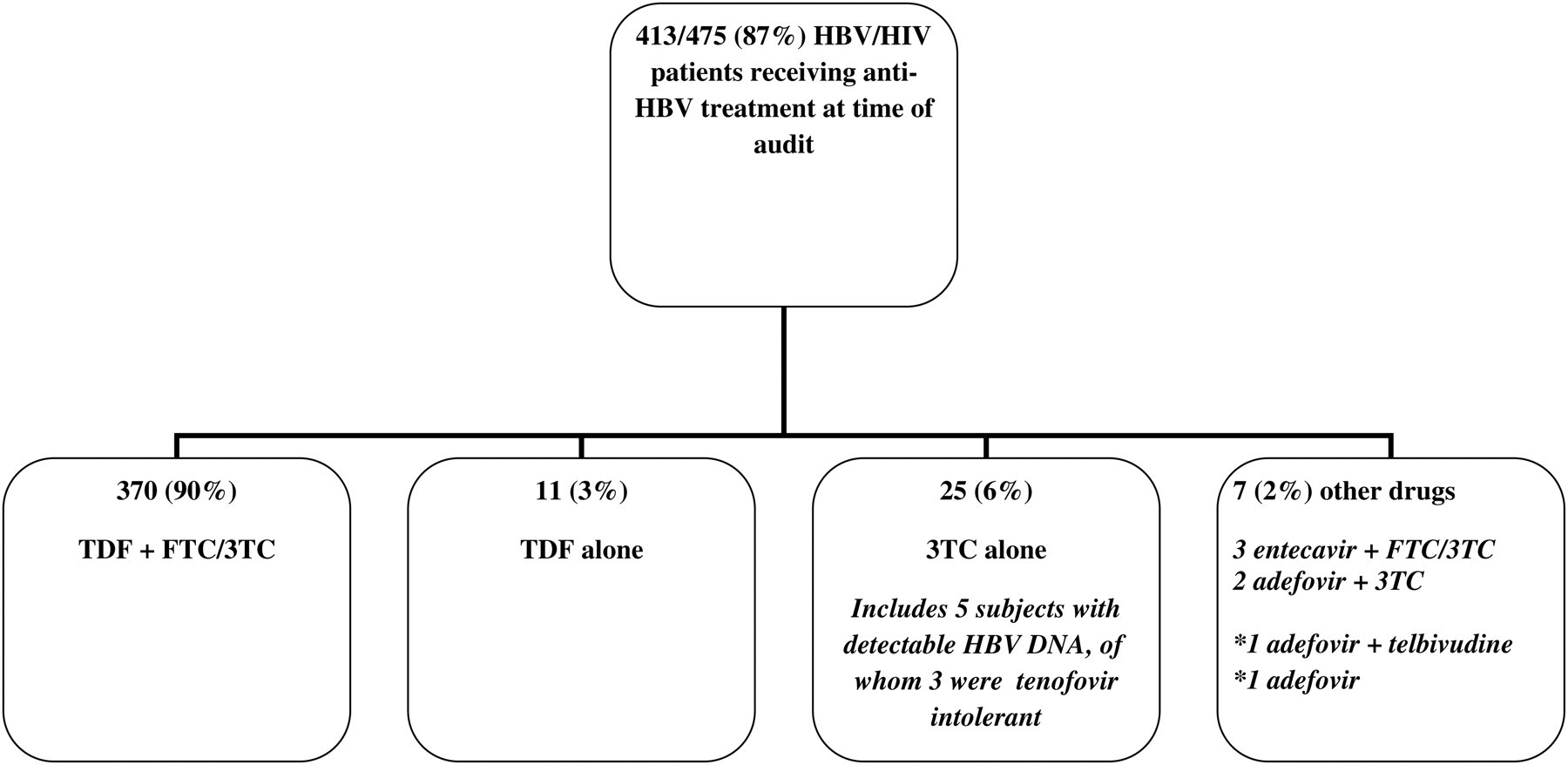
Details of current HBV treatment in HBV/HIV co-infected subjects. HBV = hepatitis B virus; TDF = tenofovir; FTC = emtricitabine; 3TC = lamivudine. All as part of cART except*
HCV treatment
Of the 522 patients with HCV/HIV, 225 (43%) had received treatment for HCV (either in the past or currently). A variety of reasons were provided for the remainder of patients being HCV-treatment naive including patient refusal, clinical decision due to mild liver disease in genotype 1 or 4, assessment/referral in progress, poor clinic attendance, spontaneous HCV clearance, mental health concerns and low plasma CD4 + cell counts.
DISCUSSION
We report the findings of a large national survey assessing the current provision of hepatitis testing for HIV patients and the arrangements for providing hepatitis treatment in HIV and hepatitis B/C co-infected adults. We also report the results of a case-note audit on the current management of 973 co-infected patients. While it is reassuring that the majority of such patients are being managed and treated according to national guidelines, some areas of concern have been highlighted.
Firstly, approximately a third of all UK sites reported not to be performing annual hepatitis B/C serology in non-immune patients and annual vaccination titre levels as the guidelines recommend. This finding is consistent with a recent study which reported that in 2007, over 20% of HIV-infected subjects attending UK clinics remain untested for HCV status. 7 Reasons for this suboptimal finding may include the absence of technologies to automatically remind clinicians when annual tests are due, a clinical decision that a subject is at ‘low risk’, for example to HCV, thus making the test a low priority and other general time constraints in the outpatient setting. It is likely that in future, with wider use of automated reminder systems to alert practitioners that annual hepatitis serology/titre checks are required (in addition to other tests e.g. cervical cytology) this service will improve.
Secondly, it was reported that 13% of co-infected patients had not been vaccinated against hepatitis A despite being non-immune. Furthermore, 5% of HCV patients were neither vaccinated nor immune to HBV – a vaccination that should be routinely administered to all non-immune HIV-positive individuals, irrespective of a diagnosis of chronic viral hepatitis. 15 Both these important public health failings in our cohorts are clear examples of clinics not adhering to existing national guidelines.
Suboptimal rates of documentation were found regarding discussion of public health issues (contact tracing) and health promotion (alcohol avoidance). While this may simply reflect incomplete documentation of consultation details and/or having separate hepatitis treatment records, without further information it is possible that important health advice is not being disseminated to all co-infected adults. Trends toward higher rates of documentation in more recent calendar years were observed (data not shown), which may reflect improving documentation and clinical care, or alternatively notes being more accessible for those with a recent diagnosis.
Just over a third of co-infected subjects included in this audit had ever undergone an assessment for liver fibrosis. In the recently revised BHIVA national guidelines, 14 this assessment is now recommended for all chronically co-infected individuals to evaluate disease status and inform decisions regarding treatment. As awareness of this recommendation improves, and facilities become more widely available, it is anticipated that fibrosis assessment will be routinely assessed in all, rather than just in clinician-selected ‘high-risk’ cases.
Interestingly, 6% of patients were receiving lamivudine (within cART) as their sole HBV treatment, which is not recommended in 2005 or 2010 guidelines. While it is reassuring that the majority of such subjects were reported to have a negative HBV DNA level when most recently tested, such a strategy may lead to the development of HBV drug resistance, limiting future therapeutic options. 16 In addition, HBV treatment was not being prescribed in a small number of individuals that are HBeAg positive and have high levels of HBV DNA replication. Such findings highlight the importance of conducting national audits of clinical practice, and particularly the need to disseminate results to all centres to ensure awareness of guidelines to all colleagues managing co-infected patients, recognizing that not all have specialist expertise in both HIV and hepatology.
There were various reasons why only 43% of HCV/HIV patients had received HCV treatment. However, advanced HIV disease (making cART initiation a greater priority) was cited for only 15 individuals. Issues around clinic attendance and referrals in progress were more frequently reported, suggesting a possible need for local investigation of whether HCV treatment uptake can be improved to reduce the future burden of chronic liver disease.
Limitations of this work include the six-month period of attendance required for inclusion and the restriction of subjects per site to a maximum of 25. These factors may have introduced a sampling bias (of recent and regular attendees) and limited our sample size; however, the limits were introduced in order that audit participation is not too time-consuming for staff.
In summary, the appropriate provision of services and treatment remains paramount to prevent excessive morbidity and mortality in HIV and hepatitis B/C co-infected subjects and national guidelines exist to provide a consensual opinion on current practice and optimal management. This project has demonstrated that while the majority of HIV-positive individuals in the UK are being tested and treated for hepatitis according to both the 2005 and 2010 guidelines, several potential areas for improvement remain and training in the appropriate management of HIV and hepatitis B/C co-infected patients remains essential.
Footnotes
ACKNOWLEDGEMENTS
The BHIVA Audit and Standards Sub-Committee: M Johnson (Chair), M Backx, C Ball, G Brook, D Churchill, A De Ruiter, S Ellis, A Freedman, L Garvey, P Gupta, K Foster, V Harindra, C O'Mahony, E Monteiro, E Ong, K Orton, R Pebody, F Post, C Sabin, A Schwenk, A Sullivan, R Weston, E Wilkins, D Wilson, M Yeomans. The authors and subcommittee would like to thank clinicians who completed the survey and the Department of Health for financial support for the BHIVA audit programme