
Abstract
We present a case of acute limbic encephalitis secondary to HIV seroconversion. The patient made a gradual neurological recovery following treatment with antiretroviral therapy, steroids and intravenous immunoglobulin.
INTRODUCTION
Limbic encephalitis (LE) encompasses a variety of disorders where inflammation predominantly affects the limbic area of the brain (amygdala, hippocampus, hypothalamus, parahippocampal and cingulate gyri). 1 Many cases are auto-immune or paraneoplastic in nature but some are associated with viral infections such as HSV-1 and human herpesvirus-6. 2 We present a case of LE associated with HIV seroconversion; we are aware of only one other case described in the literature. 3
CASE
A 28-year-old man with no past medical history presented with acute onset of fever, confusion, agitation and reduced level of consciousness following a one-day history of lethargy and vomiting. There were no typical features of HIV seroconversion and routine bloods were normal apart from an elevated alanine transaminase and mild lymphopaenia.
He was transferred to the intensive care unit and treated with cefotaxime and aciclovir for presumed meningo-encephalitis. Subsequent cerebrospinal fluid (CSF) analysis revealed a white cell count of 32 cells/mm3 (29 lymphocytes), a protein of 0.91 g/L and glucose of 4.2 mmol/L (serum 7.3 mmol/L). CSF Gram and auramine stains, bacterial, mycobacterial and fungal cultures, and polymerase chain reaction testing for herpes simplex virus, cytomegalovirus, Epstein Barr virus, varicella-zoster virus, human herpesvirus-6, Mycobacterium tuberculosis and Treponema pallidum were all negative (as was syphilis serology on serum). Magnetic resonance imaging (MRI) of the brain showed symmetrical areas of abnormality in the medial temporal lobes with high signal on (fluid-attenuated inversion recovery) FLAIR and T2-weighted sequences with no gadolinium enhancement (see Figure 1).
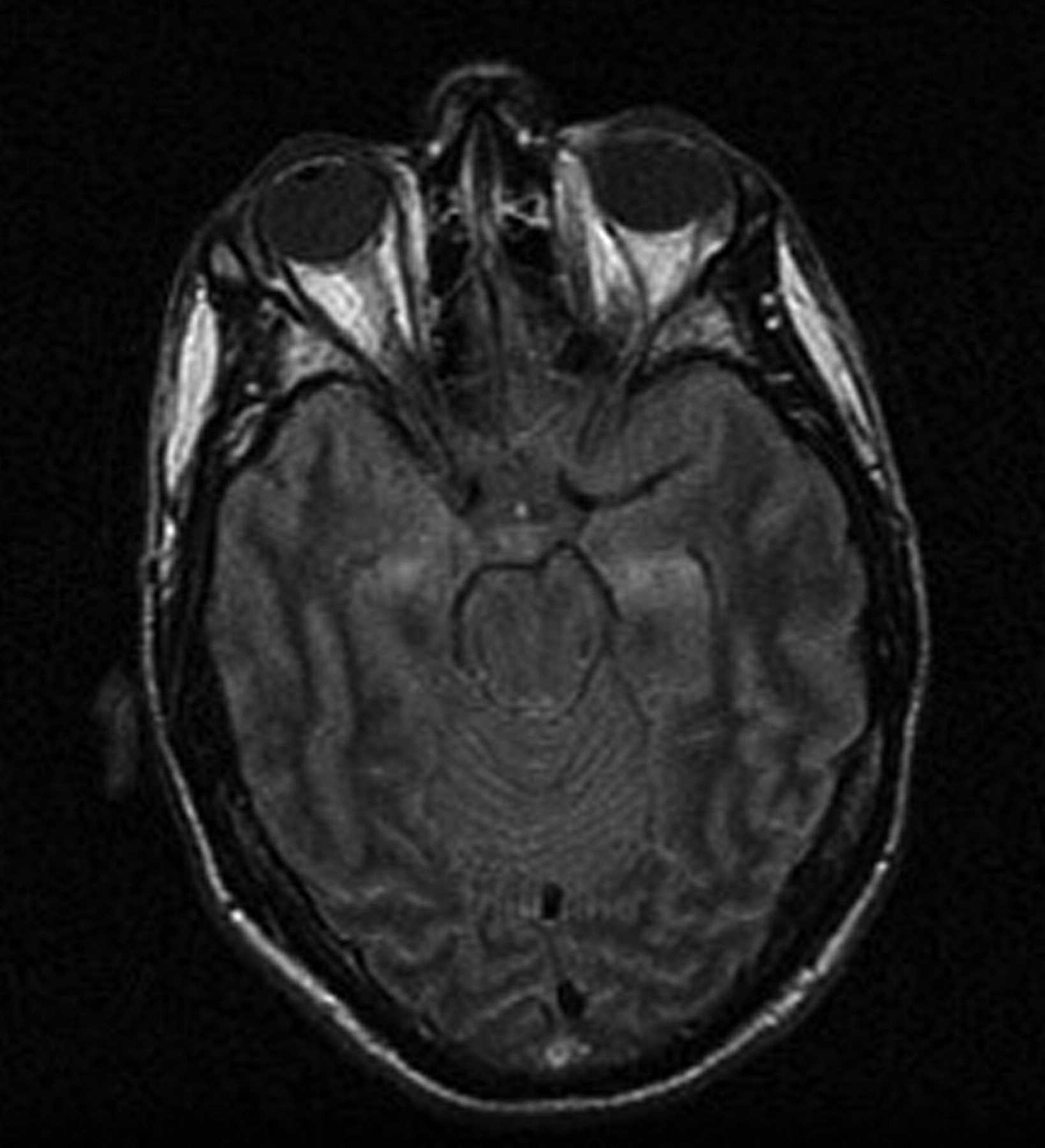
MRI brain. Fluid attenuated inversion recovery (FLAIR) T2-weighted image, demonstrating symmetrical abnormalities in the medial temporal lobes consistent with limbic encephalitis. MRI = magnetic resonance imaging
With compatible clinical, CSF and radiological features a diagnosis of LE was made. A computerized tomography scan of the chest, abdomen and pelvis and ultrasound of the testes showed no sign of occult malignancy. Anti-Hu, anti-Yo, anti-Ri antibodies (immunohistochemistry with confirmatory Western blot), anti-N-methyl-
Zidovudine, lamivudine, darunavir and ritonavir were started along with high dose steroids. However, after extubation a week later, significant problems with short-term memory were revealed. Although able to hold a superficial conversation the patient was unable to retain any new information (including his new HIV diagnosis), and asked repetitive questions about why he was in hospital. Formal cognitive assessment confirmed this, along with difficulties in verbal fluency: mini mental state examination (MMSE) 24/30, Addenbrooke's cognitive examination (ACE-r) 64/100, HIV dementia score 6/16.
Given the ongoing symptoms a five-day trial of intravenous immunoglobulin was instigated but had no immediate effect. He was discharged to the care of his family with outpatient neuro-rehabilitation. However, over the next two months he steadily improved with repeat cognitive assessment revealing an MMSE of 28/30, ACE-r of 79/100 and an HIV dementia score of 14/16.
DISCUSSION
The diagnosis of LE is based on the combination of typical neurological symptoms (memory impairment, confusion, behavioural change and seizures), temporal lobe abnormalities on MRI, and lymphocytic CSF with raised protein and oligoclonal bands. 1,2,4 LE was initially described as a paraneoplastic condition, 5 most commonly seen with lung or testicular malignancies and frequently associated with anti-neuronal antibodies such as anti-Hu, -Yo and anti-CV2/CRMP5. 1,2,4 However, there are an increasing number of cases described with no evidence of malignancy and a variety of auto-antibodies to cell surface antigens. In contrast to the paraneoplastic form, autoimmune LE often has a good response to immune-modulatory treatments such as steroids, immunoglobulin and plasmapheresis. 1,2
The most commonly described antibodies are anti-voltage gated potassium channels antibodies (anti-VGKC). 1,2,4,6 However, recent work has revealed that the target of this antibody is actually a secreted neuronal protein called LGI-1 (leucine-rich glioma inactivated 1) rather than the VGKC. 7,8 Although this protein has a close association with the VGKC it has no affect on its function and instead acts as a ligand between two other neuronal membrane proteins ADAM 22 and 23. 8 There are now calls to rename and reclassify these group of disorders. Anti-GAD antibodies have occasionally been described in cases of LE 9,10 but are more commonly associated with type 1 diabetes mellitus and Stiff man syndrome. 6,11 Ideally their level should also be measured both in the CSF and the serum to quantify intrathecal production.
There have been many described neurological complications of HIV infection; however, we are aware of only two published cases associated with LE: one with longstanding HIV infection, positive anti-VGKC antibodies and improvement with plasma exchange; 12 the other during seroconversion. 3 Although our case may have been caused by a direct effect of HIV we feel the relatively low CSF viral load and anti-GAD antibodies raise the possibility of a postinfectious immune disorder. This has previously been described following other viral infections (enterovirus and adenovirus), which improved with immune suppression. 13,14 As our patient received both antiretroviral and anti-inflammatory treatment it is not possible to know which treatment (if indeed any) contributed to his neurological improvement.
This case further illustrates the vast range of neurological complications seen with HIV infection. It re-emphasizes the importance of HIV testing in patients presenting with neurological syndromes, and the requirement for further research into the neuropathophysiology of HIV.