
Abstract
Summary
We investigated how young adults aged 18-29 years would like to be notified of chlamydia screening test results, and, when they test positive, their willingness and preferred mechanism for informing their partners. We conducted a cross-sectional survey of 6085 young adults and found that a call to their mobile phone was their preferred way of receiving positive test results (selected by 50%), followed by email. Text messages (short message service [SMS]) and calls to landline phones were unpopular options, selected by between 5 and 10%. Over 75% of respondents stated they would inform their current partner of a positive chlamydia diagnosis, and 50% would inform their previous partners. Most were willing to receive yearly reminders to go for a chlamydia test. Young adults preference for being informed of chlamydia test results by mobile phone call, rather than by email or SMS text, especially if they test positive, suggests they place high value on the security of the communication mechanism. Offering a range of mechanisms for receipt of test results may increase the acceptability and coverage of sexually transmitted infection (STI) control strategies.
Introduction
Individuals who take part in chlamydia screening programmes need to be notified of their test results, and efficient mechanisms for contact tracing are needed for those who test positive. Technologies such as email, cell (mobile) phones and short message service (SMS), also known as text messages, have become widespread, particularly among young people, and could provide effective and acceptable methods of communicating test results. In 2009, there were around 3.6 billion SMS users worldwide, which was double the number of Internet users. 1 In one UK study in an inner London sexual health clinic, 98% of surveyed users owned a mobile phone. 2 It is likely that these technologies will at least supplement and could supplant traditional means of client-clinic communication, such as letters and calls by patients to landline phones.
Lim et al. 3 have demonstrated in a randomized controlled trial (RTC) that SMS texts improve young people's (16-29 year olds) sexual health knowledge, sexually transmitted infection (STI) treatment seeking and STI-testing behaviour. Gold et al. 4 followed up their RTC with focus group research on women and men, aged 16-24 years, who were attending a music festival, which explored and confirmed the acceptability of SMS messages for sexual health promotion in this age group. 1 Menon-Johansson et al. 2 demonstrated with clients of a UK genitourinary (GU) medicine clinic that the use of text messages to communicate chlamydia test results to patients reduced the time-to-treatment of those with genital infection (and also saved staff time), compared with the standard recall methods – a request to return in person or to phone the clinic for the result.
However, it has also been suggested that the transmission of sensitive information, such as STI results by new technologies such as SMS messages, could cause some patients unnecessary anxiety and reduce their cooperation in STI control strategies. 5 Research to date on how young people would like to be notified of their chlamydia test results has been primarily qualitative and conducted among small groups of young people, mainly women, recruited from clinical settings.6-8 This paper reports the findings of a large cross-sectional survey of young men and women aged 18-29 years, including samples drawn from five universities and one equivalent third-level college (all termed universities here); and from patients attending a range of primary care settings. The study, which was conducted during the design phase of a chlamydia screening programme, aimed to measure young adults’ preferences around different mechanisms for receiving chlamydia test results (positive and negative), partner notification and receipt of reminders to go for chlamydia testing.
Method
We recruited 18-29 year olds attending one GU medicine clinic and five primary care settings (together termed ‘healthcare service attendees’) in two regions of Ireland over a two-week period in March 2009: one family planning clinic, one gay men's health clinic and three general practices (GPs) – one urban working class, one urban middle class and one rural. The advice from a senior barrister (a legal expert) was that uncertainties in Irish law around the age at which young people could consent to participating in a research study, compounded by the sensitivity of the topic, precluded surveying 16 and 17 year olds. We focused on 18-29 year olds because in 2008 the highest number of STIs, including chlamydia, that were notified to the Irish Health Protection Surveillance Centre was in 20-29 year olds. 9
Clinic attendees were invited to self-complete a paper version of a questionnaire and the university students were invited via their institutional intranets to complete a web-based version of the questionnaire, which was hosted online at the website ‘sur-veymonkey.com’. Survey questions were derived from the Irish Study of Sexual Health and Relationships; 10 from case proformas used in the UK National Chlamydia Screening Programme; and from earlier exploratory qualitative research.11-13 The research ethics committees of the Royal College of Surgeons in Ireland and the Irish College of General Practitioners approved the study.
Eligible patients attending the primary care facilities were given an information sheet by reception staff, which informed them about the study and invited them to complete the questionnaire while they waited to see a healthcare professional. The participating universities sent their students an email containing information about the study and a hyperlink to the online version of the questionnaire. Students clicking on the hyperlink were first directed to an online version of the project information sheet and were required to read this before proceeding to the questionnaire proper. Students were advised that they should only take part in the study if they were between 18 and 29 years of age. The hardcopy and online versions of the questionnaires were divided into two sections: one section asking respondents where they thought chlamydia screening services should be located and who should offer them the test; and another asked them about their test notification preferences. Respondents’ screening location preferences are reported elsewhere. 14 The notification section of the questionnaire began with a five-item closed response set that asked respondents how they would like to be contacted about their chlamydia test results, first if the result was negative and then if it was positive (see Table 2 for options); and asked them about their willingness to be placed on a register to receive yearly reminders to go for chlamydia testing (Table 3). A three-item question was then used to ask them about their notification preferences for current and previous partners (Table 3). The same questions were asked in both the online and hardcopy versions of the questionnaire. All respondents who participated in the study were invited, if they wished, to put their contact details (a mobile phone number) into a draw to receive one of five €100 prizes.
Respondents’ contact preferences
Partner notification and registration preferences
The healthcare service attendees’ responses were entered, and the survey monkey data were imported, into the SPSS statistical package 17 (SPSS Inc, Chicago, IL, USA) and data were analysed using simple descriptive statistics: frequencies (mainly yes/no responses) and chi-square cross-tabulations with 95% two-tailed tests of statistical significance (P<0.05 considered significant). The principal independent variables were gender (male/female), age (18-22 and 23-29 years), setting (healthcare facility and student intranet) and numbers of sexual partners.
Results
Sample profile
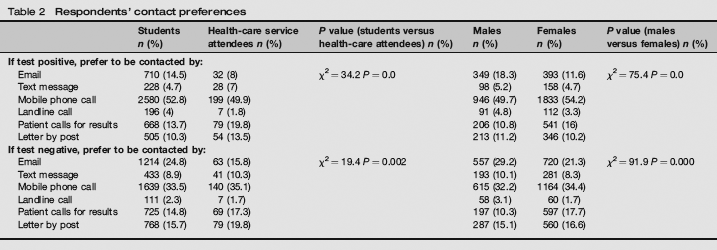
Questionnaires were completed by 5685 students and 400 healthcare service attendees at: a family planning clinic (20.8%), an urban working class GP (22.0%), an urban middle class GP (16.5%), a rural GP (14.3%), a GU medicine clinic (17.5%) and a gay men's health clinic (9.0%). Responding students, at 21 years old (mean 20.8) were younger than healthcare service attendees at 24 years (mean 23.8); and a higher proportion of students (40.2% versus 23.5%) were male (see Table 1). Two or more sexual partners in the previous year were reported by around 30% of respondents. Table 2 shows respondents’ preferred methods of being contacted to receive a positive and a negative chlamydia test result.
Respondents’ demographic profile

Positive test results
Respondents’ preferred mechanism for receiving positive test results was by a call to their mobile phones (52.8% of students and 49.9% of healthcare service attendees). A minority of students (24.0%) and healthcare service attendees (33.3%) opted for more traditional mechanisms – either postal results or calling in to a health service for the result. Email was more popular among students than among healthcare service attendees (14.5% versus 8.0%), and also among male respondents (18.3% versus 11.6% of females). The least preferred options for receiving positive test results were calls to landlines (preferred by 2-5% of respondents) and SMS messages (preferred by 5-7% of respondents).
Negative test results
Respondents’ preferred option for receiving negative test results was getting a call to their mobile phone; however, this was preferred by a lower proportion of respondents (around one-third) than when the test was positive (over half). Email was the second most popular choice, which was again more popular among students (24.8% versus 15.8%) and among men (18.3% versus 11.6%). An SMS message was a less popular choice for receiving negative results (preferred by only 8-10% of respondents), although both SMS and email were more popular when receiving a negative than a positive test result. In the case of a negative result, the least popular method was getting calls to landlines (preferred by only 1-2% of respondents).
Partner notification
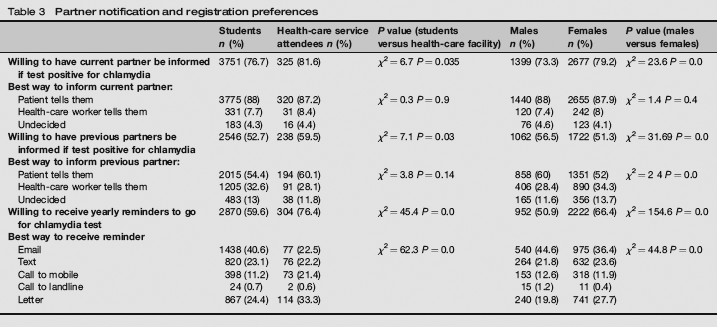
Respondents’ partner notification preferences are outlined in Table 3, as is their willingness to receive yearly reminders to go for chlamydia testing. Around four-fifths stated that they would be willing to have their current partners informed; and over half of respondents indicated that they would be willing to let their previous partners be informed, if they themselves tested positive for chlamydia. A slightly higher proportion of healthcare service attendees answered yes to both questions. A significantly higher proportion of female than male respondents were willing to have a current partner informed if they tested positive (79.2% versus 73.3%, P < 0.001); whereas men were significantly more likely than women to agree to previous partners being informed (56.5% versus 51.3%, P < 0.001). The majority (87-88%) responded that they would inform their current partners themselves. In the case of previous partners, a broadly similar percentage of healthcare service attendees (28.1%) and students (32.6%) would prefer a healthcare worker (defined as either a doctor or a nurse) to inform their previous partner; whereas significantly more women than men would prefer this option (34.3% versus 28.4%, P < 0.001).
Test recalls
Over half of respondents indicated that they would be willing to have their names placed on a database to receive yearly reminders to go for chlamydia testing. Women (66.4% versus 50.9% of men, P < 0.001) and healthcare service attendees (76.4% [79.0% of female attendees] versus 59.6% of students, P < 0.001) were significantly more likely to agree to this. Emails, texts, letters and calls to mobiles were all popular options for receiving screening reminder messages; whereas calls to landlines were unpopular, being the preferred option of only about 1% of respondents. The main variations among the respondent categories were the significantly greater popularity (P < 0.001) of emails among students (40.6%) versus healthcare service attendees (22.5%) and among male (44.6%) versus female respondents (36.4%). Conversely, a postal invitation was somewhat more popular among healthcare service attendees and female respondents (see Table 3).
Discussion
We believe this to be the first large survey conducted with young men and women in a wide range of healthcare services and university settings, where their views and preferences were elicited around how they would like to receive chlamydia test results. Most previous studies on this topic have been small qualitative studies that were conducted with young people, usually women, recruited from clinical settings.6-8 A clear finding of this study was that respondents would prefer to receive their chlamydia test results by calls to their mobile phones, and this preference was stronger if the result was positive. Previous research suggested several reasons why respondents might prefer receiving calls to their mobile phones. For many young people mobile phones are their primary (and in some cases only) means of contact. 15 A mobile phone gives a young person a chance to question the person communicating the test result, such as requests for guidance on what steps the young person should take in the case of a positive result. 13 It also enables potentially stigmatizing information (such as the fact that a young person had sought chlamydia testing) to be transmitted securely and privately between doctor/nurse and patient.7,8
The relatively low popularity of SMS or text messages, compared with other options, was surprising and appears to contradict the findings of Gold and co-workers,1,34 who found SMS both popular and effective for sexual health promotion, and the study by Menon-Johansson et al., 2 who demonstrated its effectiveness in communicating test results. Firstly, we must consider the different study methods and samples: ours was a broad range of young Irish people surveyed in different settings who were asked a hypothetical set of questions, whereas the Australian and UK studies tested a specific communication mechanism (SMS messaging). Both factors – context and the actuality of the choice on offer – could have influenced the findings. However, secondly (and of particular importance) is that our study offered the respondents a choice from a range of modern as well more traditional mechanisms. The findings are plausible in that a more sensitive message (a positive STI test result) was associated with a preference for what could be considered a more confidential mechanism (a call to one's mobile phone). Young people might perceive there to be a greater risk with SMS of unwanted disclosure, i.e. by someone, such as a parent or partner, reading one's SMS messages, yet a corresponding lesser risk of someone answering one's phone. 8 Pavlin et al.‘s 6 qualitative study found that the main reason that young women did not want to receive chlamydia test results by SMS was because of privacy concerns.
More traditional methods, including returning to clinics for test results and receipt of results by letter, were also popular options (preferred by between a tenth and a fifth of respondents). Likely reasons, again, are their greater confidentiality compared with SMS messaging and the opportunity of a health facility visit to question healthcare professionals. 7 It is also possible that a higher proportion of young Irish people are less comfortable with mobile phones than was the case in Australia or the UK, though there are no reasons to conclude this. The greater popularity of a letter or visit among those surveyed while attending a healthcare service, their greater popularity among young women who may be more used to invitations and visits to the doctor for contraception and cervical smear tests; and the greater popularity of emails among students and men also point to the importance of context and setting. Together, the findings point to the value of offering a range of communication options to suit different young people's needs and preferences.
Respondents’ partner notification preferences in our study largely corresponded with findings from previous studies of STI testing, 5 including our own earlier qualitative work. 8 Most patients were willing to inform their current partners of positive test results and to a lesser extent their previous partners. The great majority (88%) said they would prefer to inform their current partners themselves. This corresponds with previous studies where those who test positive regard personal notification as ‘the right thing to do';6,8 and the only appropriate way to notify someone about such a personal, sensitive issue as a chlamydia diagnosis. Only a slightly lower proportion of men than women in our study were willing to have a current partner informed if they themselves tested positive. This suggests that young Irish men as well as women are positively disposed towards positive STI control practices.
Concerns about notifying previous partners could stem from fears about stigma, embarrassment about bringing up the topic of chlamydia with people who could be relative strangers,16,17 and the fact that respondents might no longer have close emotional ties with their previous partners. 6 Qualitative studies have reported that partner notification is often the most negative and nerve-wracking part of the STI-testing process for patients. 18 While not a topic investigated by this study, new communication technologies, such as anonymous email and text messaging, could encourage some young people to inform their previous partners.19-22 In a follow-up pilot chlamydia screening study, we used calls to index cases’ mobile phones as the primary mechanism to initiate and complete partner notification (forthcoming publication).
A substantial number of young adults (more than half the respondents in this survey) were willing to be placed on a register to receive regular reminders to go for chlamydia testing, which suggests a population of at-risk young persons who are positively disposed to using sexual healthcare services. Such a register could provide a means of efficiently re-contacting what is often a highly mobile population, and help to ensure that young people regularly re-test even after time-limited screening campaigns finish. The positive attitude to a register among women and healthcare attendees (79% of female attendees expressed willingness to be reminded) probably reflects their greater familiarity with such processes, possibly through attending for contraception and cervical smear checks. Other factors that we did not measure, such as previous experience of undertaking a STI test, could also have accounted for differences in willingness to attend for STI testing. The study's strengths and limitations are outlined in detail in our article published elsewhere. 14
Conclusion
Early studies have demonstrated the effectiveness of SMS text messaging for sexual health promotion and STI case management. Our study concludes that the acceptability to young people of a range of mechanisms for receiving STI test results should be ascertained, both in the different cultural and country contexts and in the different healthcare service and non-healthcare service settings where chlamydia screening and testing might be delivered. It would be inadvisable to assume that SMS messaging, which is a clearly popular mechanism for sexual health promotion, will be as popular for the communication of STI test results, especially if they are positive. We suggest that a range of options be offered to young people for receipt of STI test results, so as to increase the acceptability, effectiveness and coverage of chlamydia testing and screening. Given that such strategies also need to be cost-effective from the provider (healthcare service) perspective, we recommend that a call to a mobile phone be a routinely offered mechanism for communicating STI test results and that its acceptability and cost-effectiveness be tested in future RCTs. There would be value, also, in testing out some of the hypotheses we have proposed, around young people's concerns about the confidentiality of different communication mechanisms, so as to identify the optimal range to be offered.
Footnotes
Acknowledgements
We would like to thank the young people, the higher education institutes and the healthcare settings who took part in the study. We would also like to thank the two anonymous referees for their insightful critiques of the paper and the editor for editorial advice. The Irish Health Protection Surveillance Centre supplied funding for the study. The Irish Health Research Board managed the study.