
Abstract
During the 1990s, cases of infectious syphilis were uncommon in Wales. In 2002, an outbreak occurred in a sexual network of men who have sex with men (MSM) attending a sauna. A multidisciplinary outbreak control team was convened to raise awareness of the outbreak among MSM and health professionals, assess the extent of outbreak, and initiate surveillance measures. It is likely that early intensive control efforts dampened the epidemic curve. However, since 2006 the number of cases has increased steadily to a peak of four cases per 100,000 population in 2008. The majority of cases continue to occur in MSM (81% in 2009) and in those attending genitourinary (GU) medicine clinics in south east Wales (76%). Traditional sexual networks such as saunas, bars/clubs and cruising grounds remain frequently reported, but Internet-based networks are assuming increasing importance. Public health interventions have been sustained, using traditional partner notification, health promotion initiatives, and more innovative Internet network tracing methods.
INTRODUCTION
During the 1980s and 1990s there were very few cases of infectious syphilis (<0.5 per 10,000 population per year) diagnosed in genitourinary (GU) medicine clinics in Wales. 1 By the late 1990s, a small increase in the number of cases in men reporting sex with men (MSM) was observed in clinics in north Wales. The close social and economic links between north Wales and north west England make it likely that these cases were linked epidemiologically to a large MSM outbreak in Manchester. 2,3 By contrast, syphilis remained rare in the urban centres of south Wales during the 1990s with a small number of sporadic cases, usually reporting a history of exposure abroad.
Between January and June 2002, four cases of early syphilis were diagnosed in Cardiff: two in heterosexual men and two in MSM. Intensive contact tracing found no evidence to link these cases. However, in October 2002, early infectious syphilis was diagnosed by Cardiff GU medicine clinic in a man who reported sexual contact with men in Manchester in July 2002 and in Newcastle in August 2002. This man (index case) also reported 20 MSM contacts at various locations in south Wales in the preceding three months, including a gay sauna. One week later, Swansea GU medicine clinic diagnosed early infectious syphilis in a MSM patient. This man reported sexual contacts at the same sauna in late August/early September 2002 as well as three other sexual contacts following his sauna visit. Identifying the sauna as a possible focus of transmission raised the possibility of an ongoing outbreak of syphilis among MSM in south Wales.
We describe the changing epidemiology of syphilis in Wales over the last decade, including the public health response to an outbreak that heralded the re-emergence of syphilis as a public health problem.
METHODS
Outbreak response
An outbreak control team was convened in October 2002 comprising physicians and health advisers from Cardiff GU medicine clinic, outreach and health promotion specialists, health protection specialists and epidemiologists. The outbreak team had four objectives: (i) to raise awareness of the outbreak among local primary care services and the gay community in south Wales; (ii) to provide outreach testing; (iii) to develop an enhanced surveillance scheme for syphilis across Wales, and; (iv) to carry out surveillance of risk behavior in the sexual network associated with the sauna.
General practices and dental practices in south east Wales were informed by letter of the re-emergence of syphilis in Wales and were alerted to the signs and symptoms of early syphilis. GU medicine physicians across Wales were alerted by email. On-site syphilis testing (enzyme-linked immunosorbent assay [ELISA], Venereal Disease Research Laboratory test [VDRL] and Treponema pallidum particle agglutination assay [TPPA]) and HIV antibody testing (ELISA) were offered to men attending the sauna over four days in November 2002. A short questionnaire was administered to each man providing a blood sample, based upon that developed by the Health Protection Agency. 4 Only those men who were happy to provide a contact telephone number or address were tested.
Enhanced surveillance
All GU medicine clinics across Wales were invited to participate in a scheme for enhanced surveillance of infectious syphilis using a data collection form based on that used in a London outbreak. 5 Data collection commenced in December 2002, with retrospective data collection from January 2002. The aim of the scheme was to improve the timeliness of surveillance of new cases of infectious syphilis (compared with the routine quarterly, aggregate data returns based on Korner Codes [KC60]) and to provide more detail on the behavioural characteristics of cases.
Behavioural survey
A behavioural survey was carried out in March 2003 using a short questionnaire to characterize the men attending the sauna for sex and to quantify rates of risk-taking behaviour among this sexual network. The questionnaire requested information on demographics, frequency of attendance, participation in sexual activities at the sauna, sexual health status and any sexual contacts or networks. Permission was obtained from the owner/manager of the sauna and outreach workers were present at the sauna throughout the study period to explain the purpose of the study and answer any queries regarding the study or sexual health issues in general. Data from completed questionnaires were entered into a database by electronic scanning using the optical mark reader software product ‘Eyes and Hands’ (ReadSoft International, Helsingborg, Sweden) 6 and analysed using STATA 8 (Stata Corp, College Station, TX, USA). 7 The Mann-Whitney U test was used for comparisons between self-reported homosexual and bisexual men, and between those with or without a previous sexually transmitted infection (STI). The chi-square test was used to compare reporting rates for previous STI and previous HIV test between homosexual and bisexual men. Data on total sauna attendances during the study period were calculated from entrance receipts. Results from the behavioural survey were fed back to sauna attendees through posters displayed at the sauna, to further raise awareness of risk behaviour and provide opportunities for discussion. Attendees disseminated this information informally to the wider gay community in south Wales.
RESULTS
Outbreak response
As a result of increased publicity, 11 men attended Cardiff GU medicine clinic between October and December 2002 with concerns about syphilis, and two tested positive for early syphilis. One of these identified the index case as his source of infection. Thirty-two men were tested for syphilis at the sauna; eight men on each occasion the venue was visited. Three men had serological evidence of syphilis, a seroprevalence of 9.4% (95% CI: 3.2–24.2%). However, there was evidence to suggest that all three men had acquired infection several years previously. One had evidence of past treated infection (VDRL negative, ELISA positive, TPPA 1:160), and two had active infection, including one with evidence of early latent infection (VDRL positive, ELISA positive, TPPA 1:640) and one with an untreated late latent infection (VDRL negative, ELISA positive, TPPA 1:40). Neither reported symptoms of syphilis or had previously attended a GU medicine clinic. Of the 32 men tested for syphilis, two reported being HIV-positive. Twelve men accepted the offer of a HIV antibody test and no new positives were identified.
Behavioural survey
During March 2003, customers made a total of 236 visits to the sauna and 144 questionnaires were completed. Following adjustment for those individuals reporting more than one visit, the estimated participation rate was 64%. Age (reported by 97% of participants) ranged from 15 to 69 years (median: 38 years). Participants were predominantly from south Wales, but some lived as far afield as west Wales and south east England, and five reported living abroad. Sexual orientation was reported by 75% as exclusively homosexual and by 25% as bisexual. Most men attending the sauna reported no regular partner (62%). Of those reporting frequency of attendance at the sauna, 15 (10%) were attending for the first time, eight (6%) had been once before, 45 (32%) attended less than once a month, 32 (22%) once a month, 31 (22%) once a week and 12 (8%) more than once a week.
Most respondents reported having oral sex at the sauna (94% receptive oral sex, 91% insertive oral sex), 62% reported having receptive anal sex, and 73% reported having insertive anal sex. Of those having oral sex at the sauna, 90% reported on their use of condoms: 25 (22%) always used a condom for oral sex (either insertive or receptive), 35 (31%) mainly or occasionally used a condom and 57 (50%) never used a condom. Of those having anal sex at the sauna, 98% reported on their condom use: 63 (72%) always used a condom for anal sex (either insertive or receptive), 25 (28%) mainly or occasionally used a condom and nine (10%) never used a condom.
Around one-fifth of respondents (22%) reported a previous STI including: non-specific urethritis (10 men), crabs (7), gonorrhoea (4), syphilis (3), chlamydia (2), warts (1), herpes (1), hepatitis B (1) and thrush (1). Men who were exclusively homosexual were more likely than bisexual men to have had an STI (27 versus 9%; P = 0.03). Homosexual men also reported attending GU medicine clinics more frequently than bisexual men (P = 0.002). Nearly half (49%) of the respondents reported having had a HIV test. Respondents reported a mean of eight male sexual contacts in the previous three months (median 4, range 0–150) (calculated from 123 responders). There was no significant difference in the number of male contacts in the previous three months between homosexual and bisexual men (P = 0.09). Respondents with a previous STI reported more partners in the previous three months than those without an STI (P = 0.009). Seven of 131 respondents (5%) reported sex with a sex worker in the previous year, 83 of 136 respondents (61%) reported having attended gay pubs/clubs and 61% reported attending other gay saunas in the previous month.
Re-establishment of syphilis as a public health problem in Wales
A total of 523 infectious syphilis episodes were diagnosed in GU medicine clinics between 2002 and 2009 and reported to the Public Health Wales enhanced syphilis surveillance scheme (Figure 1). The number of episodes increased to a peak in late 2003 but declined in 2004 and 2005, before gradually increasing again to a peak of 120 (3.7 per 100,000 population) in 2008 (Figure 1). This trend is corroborated by routine reporting of primary and secondary syphilis by GU medicine clinics (KC60 data), which also peaked in 2008 (Table 1). Since 2008, the number of episodes has declined to 55 in 2009 and 50 in 2010 (provisional data). Diagnoses of infectious syphilis appear to demonstrate seasonal variation, and in recent years have peaked in May/June (Figure 1). It is not known whether this represents clustering of transmission events or changes in health seeking behaviour.
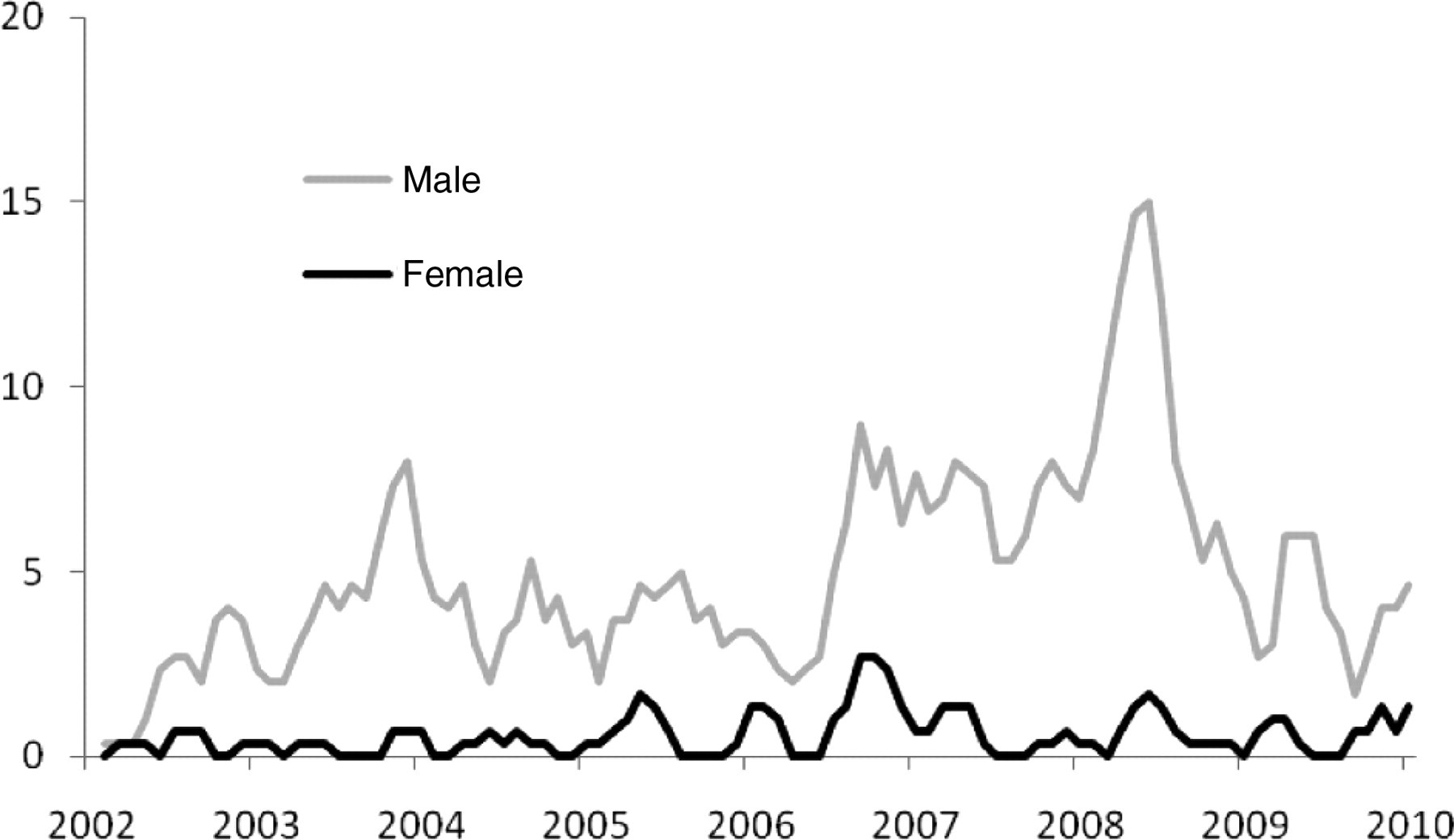
Epidemic curve: cases of infectious syphilis reported to Public Health Wales by genitourinary medicine clinics in Wales1 by month of diagnosis, 2002–092. 1Source: enhanced surveillance of infectious syphilis in Wales. 2Monthly cases represented as three-month rolling means
Cases of syphilis diagnosed in genitourinary medicine clinics in Wales in pre- and post-outbreak periods*†‡
*Source: from KC60
†Data for 2009 are provisional
‡Primary, secondary and early latent syphilis reported together for period 1991–94
The majority of syphilis episodes (470; 90%) occurred in men. The median age of cases was 34 years (range 14–79 years) and did not vary significantly by year (Kruskal–Wallis equality-of-populations rank test, P = 0.09). Information on stage of infection was available for 482 episodes. Of these, 46% were primary infections, 29% secondary syphilis and 25% early latent infections (Figure 2). Most episodes (391; 75%) were reported from clinics in south east Wales, 73 (14%) from clinics in mid and west Wales and 58 (11%) from clinics in north Wales. Sexual orientation was available for 99% of cases and included 324 episodes (62%) in men defining themselves as homosexual and 59 (11%) episodes in men defining themselves as bisexual. However, 87 men and 50 women (26% of all episodes) reported acquiring syphilis through heterosexual sex. Heterosexuals with syphilis were younger (median: 32 years) than homosexual or bisexual men (median ages: 35 and 40 years, respectively). Most (97%) MSM cases were white, whereas 22% of heterosexual cases were from a non-white ethnic group. Nearly one-fifth (99; 19%) of syphilis cases were known to be HIV-positive.

Percentage of infectious syphilis cases reported to Public Health Wales by genitourinary medicine clinics in Wales1 diagnosed at the primary stage of infection (bars) plotted with epidemic curve (line): 2002–20092. 1 Source: Enhanced surveillance of infectious syphilis in Wales. 2Epidemic curve presented as annual trend
Sixteen percent of cases reported acquiring syphilis through participation in a sexual network. Between 2002 and 2009, the most commonly reported sexual networks were saunas (40 cases), bars/clubs (36 cases), cruising grounds (19 cases), the Internet (12 cases), sex workers and group sex (7 cases each) and among students (5 cases). Use of cruising grounds has decreased in frequency in recent years but use of the Internet to find sexual contacts has increased (Table 2).
Membership of sexual networks reported by newly diagnosed syphilis cases in Wales, by year of diagnosis: 2002–09
MSM = men who have sex with men
Source: enhanced surveillance of infectious syphilis in Wales
DISCUSSION
In many ways the syphilis epidemic in Wales mirrors that in other parts of the UK. 8–13 However, the epidemic in Wales has been characterized by two phases of public health intervention. First, a phase of early, intensive action to raise awareness and assess the extent of the outbreak. Second, a phase of more sustained action including health promotion and action to trace sexual networks at greatest risk of syphilis.
A single sauna was identified early in the 2002 outbreak as a possible focus of transmission. Targeting the sauna provided both a way of controlling the outbreak in its early stages and a convenient sampling frame for evaluating the extent of the outbreak and characterising the sub-population of MSM taking part in high-risk sexual behaviour. The sauna also provided a more suitable venue for disseminating health promotion messages, particularly among regular attendees, than the relatively uncontrolled environment of a cruising ground.
The behavioural survey of sauna attendees highlighted the mobility of MSM sexual networks and the limitations of geographically focused interventions. Men reported travelling large distances to attend the sauna and local men reported high rates of sexual contact outside south Wales and abroad. Defining networks geographically may not be relevant for this population group, particularly with the increasing use of social networking sites on the Internet.
Data from the enhanced surveillance scheme confirm an increasing trend in the use of the Internet to find sexual partners. In 2007, there was a sharp increase in the number of MSM newly diagnosed with HIV in south Wales. An outbreak investigation was initiated and partner notification carried out using the provider referral method by mobile phone. Most contacts reported meeting sexual partners on the Internet. The investigation identified five new cases of syphilis, three in individuals also newly diagnosed with HIV. 14 Interestingly, this outbreak coincided with a peak in syphilis diagnoses, although it is difficult to say whether this was due to concurrent outbreaks of syphilis and HIV in MSM in south Wales or whether intensive contact tracing around the HIV cluster led to improved ascertainment of syphilis cases.
The ongoing challenge is to maintain a public health response to the syphilis epidemic. Data from the enhanced surveillance scheme indicate that the proportion of cases that were primary has declined in recent years. It is possible this decline may reflect a decrease in awareness and highlight the need for sustaining public health intervention. 15
Uncomplicated infectious syphilis is treatable with antibiotics. The prevention and control of syphilis relies on a number of well-established strategies. Since the 1940s, antenatal screening for syphilis has been carried out to prevent congenital disease and to identify and treat heterosexually acquired syphilis. 16 Screening of blood donations is also carried out to prevent health care associated infection and men who have ever had oral or anal sex with another man are no longer eligible to donate blood in Wales. 17 Both of these screening programmes aim to prevent ongoing transmission of heterosexually acquired syphilis. Although most cases of syphilis diagnosed since 2002 have been in MSM, a significant number continue to be diagnosed in bisexual men and heterosexual men and women, so these screening programmes remain an important component of syphilis control. 18
The increased incidence of syphilis in Wales since 2002 has prompted a new focus on prevention and control, including the introduction of new initiatives. Several STI health promotion campaigns have been carried out in Wales in recent years. Some, such as the BBC Wales ‘Come clean campaign’, 19 have been targeted at young people and have been fairly neutral in terms of gender and sexual orientation. However, following the 2002 outbreak, Terrence Higgins Trust Cymru has continued to conduct outreach work at gay venues in Wales and has rolled out a number of UK-level syphilis awareness campaigns targeted at MSM.
Partner notification is central to STI control and is mainly carried out by health advisers at GU medicine clinics. Tracing, notifying and treating people who have had contact with a newly diagnosed case of syphilis is a complex and skilful activity, traditionally carried out by the provider referral method using letters and home visits. In recent years, mobile phones have been increasingly used to contact partners. Partner notification works best when a case is able to provide information on recent sexual contacts. However, many MSM with syphilis report large numbers of anonymous sexual contacts, often only defined as sexual networks, associated with a particular venue or Internet website. In response, Cardiff GU medicine clinic has been piloting partner notification via Internet sites. Health advisers use a generic profile name and attempt to make contact with the profiles notified by an index case. Once the correct profile is identified, up to three messages are left asking the person to contact a telephone number to discuss, in confidence, a health-related matter. If the contact responds, the health adviser will arrange an appointment at the GU medicine clinic. If the contact accesses their message but does not respond they are classed as ‘informed’, and if the message is not accessed after one month the contact is classified as ‘unable to trace’. Data protection issues are important in setting up such a system and strict protocols and guidelines are followed. Health promotion and partner notification via the Internet for other ‘hard-to-reach’ sexual networks, such as people in relationships who take part in group sex (‘swingers’) are also being investigated.
Future surveillance should continue to include information on sexual networks and consideration should be given to identifying and responding to clusters in both MSM and heterosexual networks. The introduction of enhanced surveillance has provided more timely information than was possible using routine GU medicine clinic statistical returns (KC60 data). Routine STI surveillance in the UK is inadequate both in terms of reporting delay and the absence of demographic and behavioural details, including sexual contact networks. 20 Surveillance systems that collect disaggregated, anonymized, individual patient data have now been implemented in England. 21 Following a review of sexual health services, a similar system is currently being implemented in GU medicine clinics across Wales and has begun to generate timely, person- and area-based surveillance of sentinel STIs. 22
Footnotes
ACKNOWLEDGEMENTS
The authors would like to thank the management of the sauna in which the on-site testing and behavioural survey was carried out. The investigation was supported by the former Bro Taf Health Authority and Cardiff and Vale NHS Trust. Ian Simms and Kevin Fenton of the Health Protection Agency provided advice on setting up enhanced surveillance for syphilis.