
Abstract
This is a cross-sectional study of 399 subjects conducted to explore the association between drug use and risk behaviour for HIV and sexually transmitted infections (STIs) among female sex workers (FSWs), and also to study the prevalence of HIV/STIs among drug-using FSWs (DUFSWs) and non-DUFSWs in Yunnan province of China. Demographic information, mobility, sexual and drug-using behaviours were collected and subjects were tested for HIV/STIs. Mean age was 27 years (SD = ±7.8) and 94 (23.6%) tested positive for recent opiate use. Compared with non-DUFSWs, DUFSWs had a significantly higher prevalence of HIV (38% versus 4%, P ≤ 0.001), herpes simplex virus type 2 (HSV-2; 92% versus 60%, P ≤ 0.001) and STIs (95.7% versus 69.2%, P ≤ 0.001). DUFSWs had a significantly longer duration of commercial sex work compared with non-DUFSWs (median 5 versus 1 years, P ≤ 0.001), and had at least two clients in the last working day. DUFSWs were also more likely to work in low-end commercial sex venues and frequented a greater number of work locations than non-DUFSWs. Compared with non-DUFSWs, DUFSWs were more likely to exhibit riskier sexual behaviours and greater workplace mobility. Interventions targeting drug-related behavioural changes are needed urgently in this population in order to reduce rates of HIV and STIs.
Keywords
INTRODUCTION
HIV and sexually transmitted infections (STIs) among female sex workers (FSWs), particularly among drug users (DUs), is a significant public health problem in many Asian countries, including China. 1,2 For instance, provincial HIV prevalence rate estimates among drug-using FSWs (DUFSWs) in China range from 0.5% to as high as 81.2%, with our study setting, Yunnan province, reporting a prevalence rate of more than 10%. 3–5 One major reason fuelling such high rates is the fact that more than half of female illicit DUs continue to be involved in commercial sex work, 6 predisposing their clients and themselves to the risk of heterosexual transmission of HIV/STIs, and serving as an important conduit for the introduction of infection into the heterosexual non-drug-using population.
Drug use not only makes FSWs a critical bridging population for HIV/STI transmission, but also forces them into extensive high-risk sexual behaviours. 7 Several studies found that frequency and intensity of drug use and severity of drug dependence were associated with engagement in commercial sex, which owed chiefly to addiction-related financial pressure. 8,9 Under economic pressure, DUFSWs may engage in an increased number of sex trade transactions, and work at multiple locations in order to increase earnings. 10–12 Considering this, mobility (mobility means moving or switching one venue to another) seems to be an important factor in facilitation of the spread of HIV and STIs. 13 Few studies have investigated the relationship between illicit drug use and mobility among FSWs. Therefore, we hypothesized that DUFSWs could be at higher risk of HIV/STIs due to greater mobility and more high-risk sexual behaviours than non-DUFSWs.
The primary objective of this study was to explore the association between drug use and risk behaviours for HIV/STIs among FSWs, and also to estimate the prevalence of HIV/STIs among DUFSWs and non-DUFSWs in Yunnan province, China.
METHODS
Study site and participants
This study was conducted in the city of Kaiyuan in Yunnan Province, China. Kaiyuan has a population of 260,000 and is located in south-western China. The city is a major trade route to neighbouring south-eastern Asian countries of the opium-producing Golden Triangle region. 14,15 Due to its geographical location, heroin use is prevalent in Yunnan. Serological surveys conducted in Kaiyuan in 2003 found HIV prevalence among FSWs and DUs to be as high as 7.1% and 58.9%, respectively. 15,16
From 1 September to 31 October 2007, a convenience sample of 404 FSWs was recruited from all commercial sex venues in Kaiyuan. Peer outreach workers (former FSW volunteers and community liaison officers) working for the Kaiyuan Center for Disease Control and Prevention (CDC) were engaged to approach the managers of commercial sex venues in person and ask them if they would like to attend our meetings. After attending the meeting, the managers were at liberty to explain to their FSWs if the latter would like to undergo HIV/STI testing or not. For each FSW who volunteered for the test, the respective manager was paid 5 RMB, while the FSW was paid 20 RMB. Subsequently, five FSWs opted out of the study, citing the questionnaire as being too long, giving a participation rate of 98.8%. The study was approved by the Institutional Review Board of the Chinese CDC.
Inclusion criteria for participation in this study were: at least 16 years old (the legal age for employment in China) and willing and able to provide informed consent and history of commercial sex work within last three months. Participants who reported illegal use of opium-based drugs such as morphine, heroin, opium, and codeine in the last six months and/or received positive morphine urine test results were classified as DUs; otherwise participants were considered to be non-DUs.
Figure 1 shows the profile of the study participants.
Study profile of participants FSW = female sex workers; DU = drug users; HSV-2 = herpes simplex virus type 2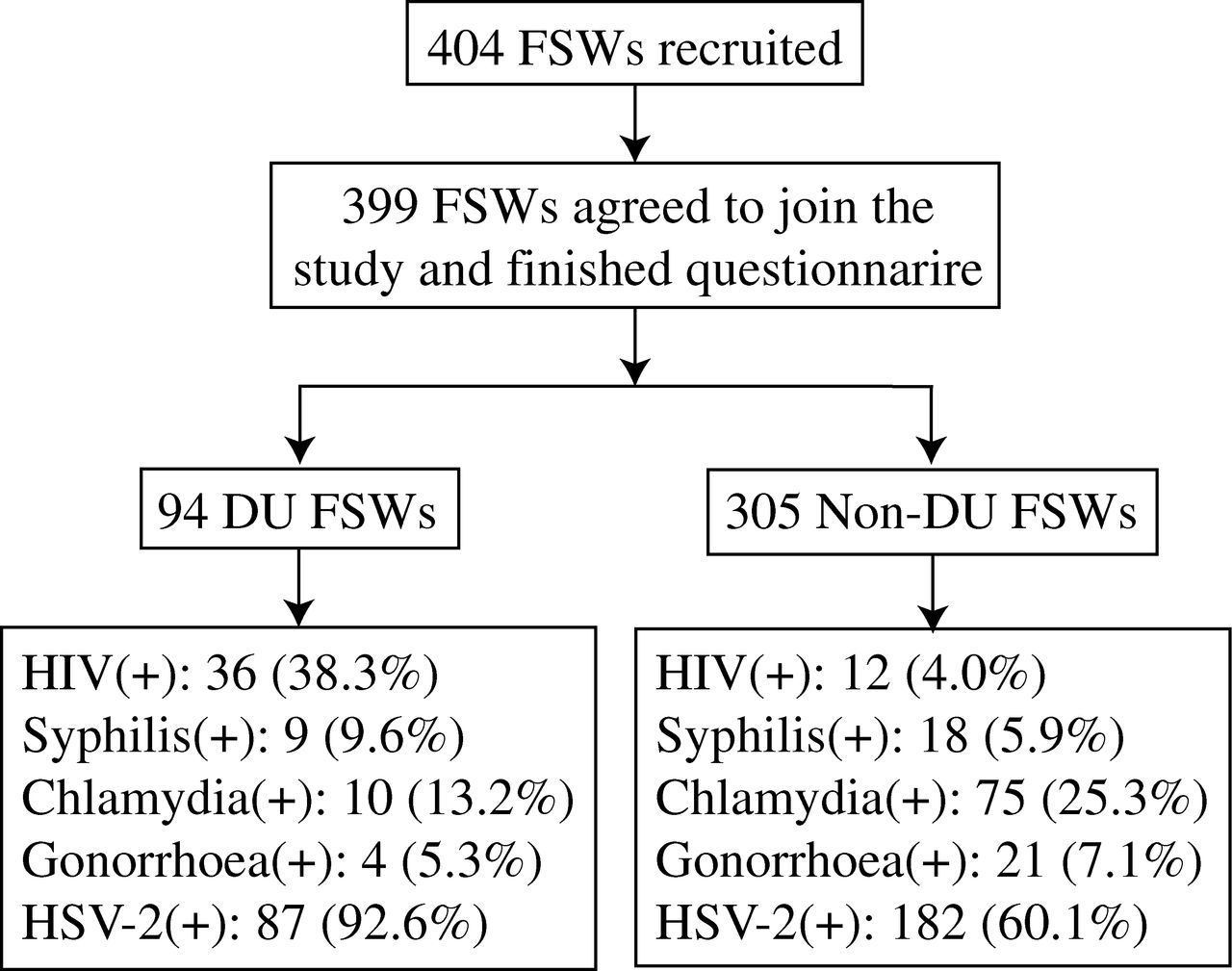
Procedures and data collection
All subjects were informed that the study was voluntary and that there would be no negative consequences for non-responders. After allocating each participant with a unique identification (ID) number and obtaining informed consent, a face-to-face verbal interview was conducted in a private (confidential) room with a trained staff member, who also administered a standardized, anonymised questionnaire regarding demographic characteristics (age, ethnicity, marital status, residence and educational level), mobility, sexual behaviours and drug use. Multiple variables, including self-reported residence re-location, workplace changes and physical moves between Kaiyuan and other cities were used to measure mobility. Commercial sex venues were grouped according to prevailing average rates/charges per client visit in Kaiyuan as follows: low range venues (<50 RMB per client) included sauna, residential sublets, inns and the street; mid-range venues (50–100 RMB per client) included hair salons; high range venues (>100 RMB per client visit) included hotels, nightclubs and karaoke halls. These rates were obtained from the peer outreach workers, some of whom were still engaged in commercial sex work during the period of the study.
After each interview, participants were asked to provide urine and blood samples as well as cervical swabs for laboratory testing. FSWs who did not complete the survey were excluded from the study and thus did not provide biological samples and were not paid.
When the results were ready, the peer outreach workers informed the FSWs (through their bosses) to come back to Kaiyuan CDC for a face-to-face notification of the test results. Those with a positive test result were given an introductory referral letter to take to Kaiyuan People's Hospital or the Kaiyuan Dermatology Hospital for treatment at a 50% discounted charge. The letter did not have a name, but had the unique ID number the subject was allocated at the beginning of the study. The two hospitals were cooperating partners in this study, and Kaiyuan People's Hospital is the only designated place for HIV treatment in Kaiyuan city, while Kaiyuan Dermatology Hospital is the largest hospital for treatment of STIs in the city.
Laboratory testing
HIV antibodies were initially detected in blood samples by an enzyme-linked immunosorbent assay (ELISA; Beijing Wan Tai Biological Pharmacy Enterprise Co, Beijing, China). ELISA-positive samples were tested twice, and positivity was confirmed by a HIV-1/2 Western blot assay (HIV Blot 2.2 WB, Genelabs Diagnostics, Singapore). Each plasma specimen was also tested for antibodies to herpes simplex virus type 2 (HSV-2) by ELISA (HerpeSelect-2 ELISA IgG, Co, Focus Diagnostics, Cypress, CA, USA) and Treponema pallidum by rapid plasma reagin (RPR, RPR Diagnosis Kit Co, Xinjiang Xindi, China). Plasma specimens positive for RPR were confirmed by the T. pallidum particle agglutination assay (TPPA, SERODIA, Fujirebio Co, Tokyo, Japan). Participants whose specimens tested positive for both TPPA and RPR were considered infected with syphilis.
Cervical swab specimens were tested for nucleic acids of Neisseria gonorrhoeae and Chlamydia trachomatis by polymerase chain reaction (PCR; AMPLICOR, Roche Molecular Systems, Branchburg, NJ, USA). A specimen was considered N. gonorrhoeae-negative if the optical density (OD) was <0.2 or -positive if the OD was ≥2.5. For C. trachomatis testing, OD < 0.2 was considered negative, and OD ≥ 0.8 was considered positive. If 0.2 ≤ OD < 2.5 for N. gonorrhoeae or 0.2 ≤ OD < 0.8 for C. trachomatis, the specimens were re-tested in duplicate tubes. For the N. gonorrhoeae test, if at least two of the three tubes had OD ≥ 2.0, the specimen was considered positive. For the C. trachomatis test, at least two of the three tubes had to have OD ≥ 0.2 for the specimen to be considered positive. Urine was collected for opiate screening using the MOP One Step Opiate Test (ACON Laboratories Inc, San Diego, CA, USA), a chromatographic immunoassay that detects opiates in urine at a cut-off concentration of 300 ng/mL. In this test, a negative result is indicated by two lines; a positive result by one red line; and an invalid result by non-appearance of the control line. Furthermore, all urine specimens were screened by the morphine-gold-conjugate test strip (ACON MOP, Acon Biotech, Hangzhou, China) method.
Statistical analyses
Descriptive statistics were used to summarize data. Chi-square tests and Mann-Whitney tests were used to analyse differences between DUFSWs and non-DUFSWs for categorical and continuous covariates, respectively. Logistic regression was used to test predictors of risk for HIV infection and drug use. Log likelihood ratio test was used to find variables retained in the multivariable model. All probability values were reported as two-sided and P < 0.05 was considered statistically significant. Data analysis was performed using SPSS version 12.0 (SPSS, Chicago, IL, USA) software.
RESULTS
Demographics of the study population
Demographic characteristics, sexual behaviours and prevalence of HIV/STIs among FSWs
FSW = female sex worker; DUFSW = drug-using FSW; STI = sexually transmitted infection; HSV-2 = herpes simplex virus type 2
*P value was calculated between DUFSW and non-DUFSW
†Others for martial status includes single, divorced or widowed; others for current residence includes commercial sex venue and family home
‡A total of 397 FSW provided blood specimens (the 2 participants who refused to provide blood specimens were non-DUFSW) and were tested for HIV, syphilis and HSV-2; 373 FSW (70 DUFSW and 303 of non-DUFSW) provided vaginal swab specimens and cervical swab specimens and were tested for gonorrhoea and chlamydia
Drug use behaviours
According to the urine screening test, 94 of the 399 participants (23.6%) were positive for opiate use, whereas only 88 (22%) subjects self-reported a history of drug use. Among FSWs who reported drug use, 86 (97.7%) used heroin, two used ketamine; 77 (87.5%) reported having injected drugs (heroin), 11 (12.5%) by inhaling. Among 77 who injected heroin, 37 FSWs injected with diazepam, two with triazolam and one with promethazine. Injection drug use (IDU) ranged from 1 to 16 years (mean = 6.9 ± 4.2 years). Of 77 self-reported IDU FSWs, 55 (71.4%) reported IDU within the last three months and of those 55 subjects, 11 (20%) reported syringe sharing.
Sexual behaviours
Mobility of DUFSWs and non-DUFSWs
FSW = female sex worker; DUFSW = drug-using FSW
*The venues were the places where FSWs had stayed in the last year
† P value was calculated between DUFSWs and non-DUFSWs
HIV/STIs
Of the 399 FSWs, 397 provided blood specimens, and 373 provided vaginal and cervical swab specimens. HIV prevalence among tested FSWs was 12.1%. The HIV prevalence was 38.3% (36/94) among DUFSWs and 4% (12/305) among non-DUFSWs.
Of 397 STI-tested subjects, 301 (75.4%) had at least one type of STI (HSV-2, C. trachomatis, N. gonorrhoeae or syphilis). HSV-2 was the most prevalent STI (67.4%), followed by C. trachomatis (22.8%), syphilis (6.8%) and N. gonorrhoeae (6.7%). STI prevalence was 95.7% (90/94) among DUFSWs and 69.2% (211/305) among non-DUFSWs. Compared with non-DUFSWs, DUFSWs had a significantly higher prevalence of HIV (38.3%, P ≤ 0.001) and HSV-2 (92.6%, P ≤ 0.001), but a significantly lower prevalence of C. trachomatis infection (14.3%, P = 0.025) (Table 1).
Mobility
Mobility among FSWs was high, as evident in the number of residence and workplace relocation along with movement between Kaiyuan and other cities. Among all subjects, 59% had changed residences at least once in the last three years, and 25% had moved at least twice. DUFSWs were less mobile in their residential relocation as compared with their non-DU counterparts (45.7% versus 63.3%; P = 0.004). DUFSWs had cumulatively worked in more commercial sex venues than non-DUFSWs (59.6% versus 35.1%; P ≤ 0.001) (Table 2). In the last year, DUFSWs were more likely to switch between work places of differing price range than non-DUFSWs (20.2% versus 7.9%; P = 0.001). Among DUFSWs, there were 56.8%, 19.3%, 50.0% and 17.0% who had worked in karaoke hall/nightclub, hotel, hair salon and temporary sublet/inn/street, respectively; whereas 62.7%, 8.0%, 26.4% and 10.6% of non-DUFSWs had worked in the same respective places. The main reasons cited in the questionnaire for DUFSWs’ versus non-DU FSWs’ work relocations were as follows: desire to earn more money (31.0% versus 34.4%); bad business (29.8% versus 19.3%); dislike of current work venue (8.5% versus 6.2%); worrying about personal security (8.5% versus 0.7%); dislike of boss (4.3% versus 2.3%) and dismissed by boss (1.1% versus 0.3%). Upon comparison of the cited reasons, the DUFSWs had significantly more ‘bad business’ (P = 0.032) and were significantly more worried about personal security (P = 0.010) than the non-DUFSWs.
In terms of duration of commercial sex work, more DUFSWs had worked in Kaiyuan for longer than one year as compared with their non-DU counterparts (68.0% versus 44.9%; P ≤ 0.001).
Logistic regression analyses for HIV infection and drug use
Univariate and multivariate logistic regression analysis of predictors of HIV infection among FSWs
Multivariate model chi-squared = 86.5
OR = odds ratio; AOR = adjusted OR; CI = confidence interval; FSW = female sex worker; HSV-2 = herpes simplex virus type 2
Controlling for age as the main potential confounder of the association between drug use and risk behaviour, drug use was significantly associated with the number of work locations in the last year (OR = 2.3; 95% CI: 1.3–4.1; P = 0.003) and duration of commercial sex work (OR = 6.2; 95% CI: 3.5–11.3; P ≤ 0.001).
DISCUSSION
This is one of the few studies focusing on drug use and its related risk behaviours for HIV/STIs among FSWs, especially mobility behaviours. Higher prevalences of HIV and STIs were observed in DUFSWs (38.3%, 95.7%) than in non-DUFSWs (4%, 69.2%). Drug use was significantly associated with duration of commercial sex work and number of work locations in the last year.
Compared with non-DUFSWs, DUFSWs had a higher rate of HIV/STIs, more clients per day and more work relocations in the last year, rendering the latter as an important cohort in the spread of HIV/STIs across different subpopulations. DUFSWs, especially IDU FSWs were at very high risk of HIV/STI transmission, both due to IDU and commercial sex behaviours. They might bridge HIV/STI transmissions from injecting DUs to clients of FSWs. 12,17 And HIV/STIs could easily be transmitted to the clients of FSWs and other non-regular sexual partners. Potential bridging of HIV/STI transmissions from the higher prevalence DUFSW population to other non-DU populations is expected to be highly efficient.
Among DUFSWs, drug use was significantly correlated with the duration of commercial sex work (r = 0.461, P ≤ 0.001). The longer they used drugs, the longer sex work experience they had, and this predisposed the FSWs to high-risk sexual behaviours, more chances of contracting HIV/STIs and transmitting them to others. These results are in agreement with reports from previous studies. 18
With the exception of duration of sex work, the number of work locations in the last year was also associated with drug use among FSWs. DUFSWs were more likely to switch between different work places compared with non-DUFSW (31.0% and 29.8% of DUFSWs reported earning more money and bad business in the original work venues as the reasons for their work relocations, respectively). Studies conducted in the UK 19 and in Mexico-USA border cities 20 found that, compared with other FSWs, DUFSWs earned less money for sex work and took on more clients per day to support their drug habits. Thus, switching work location was possibly one of the best ways to generate more money from clients. 21 Additionally, personal security was also an important reason for DUFSWs to switch between work venues. In China, commercial sex and drug use are illegal. If a person is found to sell sex by police, they get punished. Also, an individual who is found to be addicted to illegal drugs are sent to compulsory treatment for drug addicts. In order to evade all of these, DUFSWs are usually much more careful than non-DUFSWs. Based on the foregoing, DUFSWs could be expected to have greater mobility than non-DUFSWs.
These results should be interpreted with caution due to some limitations of our study. Firstly, the method of sampling we used has inherent selection bias; hence, it is difficult to draw a sample that is representative enough to generalize these results with absolute confidence. Secondly, low monetary compensation rates might have affected participation rates in our study, thereby impacting negatively on sample size. This was especially so for non-DUFSWs, who might have been under-represented due to the fact that they have relatively less financial pressures compared with DUFSWs. As a result, FSWs from DU populations might have been over-represented in our sample, possibly leading to an overall overestimation of HIV and STI prevalence rates among the population of FSWs in Kaiyuan. Thirdly, we performed urine screening tests for opiates only; hence, it is possible that we could have missed other illicit drug use such as amphetamine and methamphetamine. Fourthly, our study was also subject to social desirability bias and recall bias, which might have led to under-reporting of risk behaviours.
We conclude that there is need to arrest the rising prevalence of HIV among FSWs in Kaiyuan city, which stands at an alarming rate of 12% compared with its provincial estimate of 5.2% and the national estimate of 1.0% in this population. 22,23 In this study, we found that DUFSWs were more likely to work in low-end commercial sex venues and frequented a greater number of work locations than non-DUFSWs; hence, because such riskier sexual behaviours are precipitated by drug use, our findings underscore the need for more targeted interventions among FSWs in regions with extensive drug use. Future studies should focus on exploring further the socio-cultural dynamics that are fuelling the HIV/STI epidemic in FSWs as well as other subpopulations in China.