
Abstract
To determine factors that influence excision treatment outcome and recurrence of cervical squamous intraepithelial lesions (SIL) in women living with HIV infection, we analysed 1848 women who underwent excision treatment of cervical SIL at Tygerberg Hospital, Cape Town, South Africa. We compared treatment failure defined as presence of cervical intraepithelial neoplasia (CIN) I (presence of CIN I or higher at first follow-up after excision treatment) and post-excision recurrence of lesions (at one year or later) between women of HIV-positive, -negative or unknown status and examined factors associated with excision treatment outcome and recurrence. HIV-infected women experienced higher treatment failure than uninfected women (53.8% versus 26.9%, P< 0.001). At treatment failure, more HIV-infected women had low-grade squamous intraepithelial lesion (LSIL) compared with uninfected women (64.9% versus 37.3%, P < 0.001). Treatment failure did not differ with the type of excision used in HIV-infected women. HIV-infected women were more likely to experience recurrence of lesions after excision treatment than uninfected women (hazard ratio 1.95, 95% confidence interval [CI] 1.59-2.39; P < 0.001). Antiretroviral therapy (ART) initiated before excision biopsy had a strong protective effect against recurrence (hazard ratio 0.70, 95% CI 0.55-0.89; P = 0.006). Our data suggest that women with cervical SIL initiated on ART earlier may be expected to have better long-term excision treatment outcome. Close follow-up should be maintained after cervical excision treatment, especially in a setting of high HIV prevalence.
Keywords
Introduction
There is evidence for an altered course of human papillomavirus (HPV) infection and development of cervical cancer in HIV-infected compared with HIV-uninfected women. HIV-infected women are five times more likely to have cervical squamous intraepithelial lesions (SIL) and 10 times more likely to develop cancer.1-10
Previous studies describing excision treatment outcome of SIL have involved small cohorts of HIV-positive women in low HIV prevalence settings and they found treatment failure to be very common at 36.2% to 73%.11-13 Reports were conflicting, with post-excision lesions mostly low-grade 13 or high-grade. 12 Treatment success was associated with higher CD4 count11,12,14 but not with antiretroviral therapy (ART). 12 An improved outcome with conization (cold-knife cone, CKC) over loop excision (LEEP or LLETZ) was also observed for HIV-infected women. 12
In this study, we investigate the factors that influence outcome of excision treatment and recurrence of cervical SIL in a large cohort in a setting of high HIV/HPV prevalence.
Materials and methods
Study population
This retrospective cohort analysis used electronic records of 1848 women that underwent excision treatment of SIL of the cervix at Tygerberg Hospital, Parow, Western Cape region of South Africa during the period July 2004 to July 2009. Only women that had >24 weeks follow-up available were included. Women were assigned to one of three groups: HIV-infected, HIV-uninfected or HIV status unknown. The choice of HIV group was made according to the status as known at excision biopsy (EB), as this was the most common point at which a patient's status was identified.
Regulatory approvals
The study was approved by the Stellenbosch University Human Research Ethics Committee (ref no N11/01/007).
Operational definitions, explanatory and outcome variables
Histopathology and cytology data as well as information regarding use of ART were extracted and anonymously linked to a study-specific identifier. ART exposure was defined as follows: ‘ART started before EB’ and ‘no ART indicate the start time or absence of ART, respectively. For the analysis of excision treatment failure, ‘after EB’ means that ART was started during the first 365 days after EB; for the analysis of recurrence, it indicates that ART was started after EB but before endpoint of survival analysis. Baseline CD4 count was stratified in three groups according to the current South African guidelines for initiation of antiretroviral therapy: <200 cells/μL, 200-350 or >350 cells/μL.
Squamous abnormalities were classified as LSIL, high-grade SIL (HSIL) or cancer according to the 2001 Bethesda Classification System. 15 Cytology was performed with routine Papanicolaou (Pap) smear. The quality of cytology was assessed by determining the percentage of smears with endocervical cells (EC) present. Pathology was considered to be more specific and the result used if a smear performed on the same day was of lesser severity.
EB refers to the surgical removal with the loop electrosurgical excision (LLETZ or LEEP) or the CKC method. Excision treatment failure is the presence of at least CIN I at first follow-up visit.
Post-excision recurrence (at one year or later) refers to the proportion of the population with disease after EB at a given time. The statistical method for this analysis is described below.
Statistical analysis
Mean or median and the interquartile range were calculated as a measure of spread of the baseline characteristics. The f-test was used to compare statistical significance of baseline continuous variables such as mean ages of women by HIV status. Dichotomous baseline variables were evaluated using proportions and compared by performing two-tailed chi-squared test.
For the analysis of EB treatment failure, 1620 women out of the total 1846 in the cohort were selected as women who had the first post-excision follow-up evaluation within 365 days. Logistic regression was used to evaluate the association of factors such as HIV status with excision treatment outcome. Of the 1620 women analysed, the 653 HIV-infected women were analysed separately as well, using univariate and multivariate logistic regression to evaluate the association of each risk factor separately with treatment failure. In the multivariate analysis the selected covariates were included because of clinical relevance. Subsequent excision and subsequent hysterectomy were not included in multivariate analyses, since although there was a strong association, the subsequent procedure was performed as a result of excision treatment failure and could not be considered a cause thereof.
Survival analysis of recurrence-free time in the post-excision period used the Kaplan-Meier method and log-rank test to compare the HIV status groups. All 1846 women in the cohort were included in the recurrence analysis. For the analysis the time 0 was taken as the date that the first EB was performed. The endpoint for recurrence-free survival was taken as the first date that the patient had CIN I or higher (event), or if there was no lesion after excision, the date of last follow-up evaluation (Pap or histopathology) during the post-excision period was used (censored). Cox regression analysis was applied to investigate the influence of covariate factors such as excision type and completeness of excision. The analysis was also done separately for the 778 HIV-infected women to further include covariates CD4 count and ART.
Results
Baseline demographics
Table 1 provides demographics data by HIV status. Of note, the quality of Pap smears performed on the HIV-infected group was found to be marginally inferior (with the percentage of smears with no EC present higher at 19.1%), compared with 15.6% in HIV-uninfected (P = 0.006) and 18.2% in the HIV-unknown status groups (P = 0.05).
Demographic and clinical characteristics
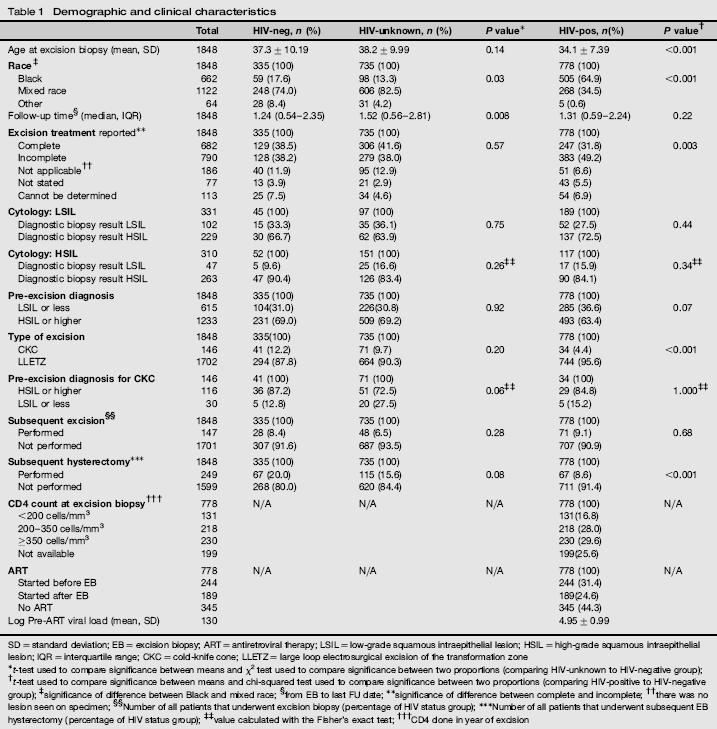
SD = standard deviation; EB = excision biopsy; ART = antiretroviral therapy; LSIL = low-grade squamous intraepithelial lesion; HSIL = high-grade squamous intraepithelial lesion; IQR = interquartile range; CKC = cold-knife cone; LLETZ = large loop electrosurgical excision of the transformation zone
t-test used to compare significance between means and χ2 test used to compare significance between two proportions (comparing HIV-unknown to HIV-negative group);
t-test used to compare significance between means and chi-squared test used to compare significance between two proportions (comparing HIV-positive to HIV-negative group);
significance of difference between Black and mixed race;
from EB to last FU date;
significance of difference between complete and incomplete; there was no lesion seen on specimen;
there was no lesion seen on specimen;
Number of all patients that underwent excision biopsy (percentage of HIV status group);
Number of all patients that underwent subsequent EB hysterectomy (percentage of HIV status group);
value calculated with the Fisher's exact test;
CD4 done in year of excision
Excision treatment failure
HIV-infected women experienced markedly higher excision treatment failure than HIV-uninfected women at first follow-up after EB treatment. Overall, treatment excision failed in 53.8% of HIV-infected women (P < 0.001) and 23.8% of women of unknown HIV status (P = 0.31) compared with 26.9% of HIV-uninfected women. In cases where excision was reported complete, treatment failure occurred in 41.1% of HIV-infected women (P < 0.001) and 11.7% of women of unknown HIV status (P = 0.38), respectively, compared with 14.9% of HIV-uninfected women. Treatment failure for incomplete excisions was 65.9% for HIV-infected women (P < 0.001) and 34.5% for women that were of unknown HIV status (P = 0.68) compared with 36.7% in HIV-uninfected women.
The results of univariate and multivariate logistic regression of excision treatment outcome in HIV-infected women are listed in Table 2(a) (all women) and 2b (HIV-infected women).
Factors influencing excision treatment failure

EB = excision biopsy; LSIL = low-grade squamous intraepithelial lesion; HSIL = high-grade squamous intraepithelial lesion; CKC = cold-knife cone; LLETZ = loop electrosurgical excision
Not applicable: no lesion;
after 1 year
At treatment failure the lesion detected was most likely to be LSIL in HIV-infected compared with HIV-uninfected women. Of HIV-infected women, 62.7% had LSIL, compared with 33.0% of HIV-uninfected women (P < 0.001).
Post-excision recurrence
More HIV-infected women experienced recurrence of lesions after excision treatment than HIV non-infected women or women of unknown status (Figure 1).
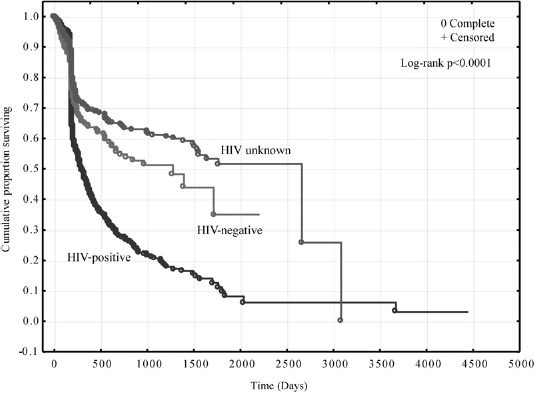
Squamous intraepithelial lesions recurrence-free survival after excision biopsy
The results of univariate and multivariate survival analysis of recurrence of lesions are listed in Table 3(a), and for HIV-infected women alone, in Table 3(b).
Factors associated with recurrence of squamous intraepithelial lesions

EB = excision biopsy; LSIL = low-grade squamous intraepithelial lesion; HSIL = high-grade squamous intraepithelial lesion; CKC = cold-knife cone; LLETZ = loop electrosurgical excision
Not applicable: no lesion;
after one-year follow up
Discussion
We found that HIV-infected women experienced much higher excision treatment failure than HIV-uninfected women, but that failure occurred mostly as low-grade lesions. Factors that improved outcome were higher CD4 count and complete excision. Recurrence was much more common in HIV-infected women than uninfected women. Importantly, initiating ART before excision treatment reduced risk for recurrence.
Treatment failure in HIV-infected women was previously reported to be more LSIL, 13 but in contrast Reimers 12 , who reported 55% treatment failure in HIV-positive women (similar to our 53.8%) found most (>70%) treatment failure lesions to be HSIL. Like Reimers, we set the minimum lesion for treatment failure conservatively at CIN I, but found 62.7% of lesions at treatment failure to be LSIL in the HIV-infected women.
Others have previously already reported better excision treatment outcome with higher CD4 counts,11,12,14 which we could confirm. We found no association of CD4 count with recurrence, however ART that was started before excision treatment did not significantly reduce risk for excision treatment failure, but there was a strong association of ART with reduced risk for recurrence. We had few women who had been treated with ART for longer periods and presented with indication for excision, and the question is if the ART had protected women from progression of low-grade disease. 16
The strength of this study lies in its large sample size and the use of a combination of cytology and pathology results in determining and comparing outcome of excision treatment of cervical SIL. Set in high HPV/HIV prevalence area, it describes the clinical scenario physicians and their patients are faced with in limited-resource countries.
Our study has a few limitations. First, as for all observational data, our study may be subject to unknown confounding factors that we are not aware of and therefore were not controlled for in our multivariate models. Furthermore, the quality of cytology was inferior for the HIV group as measured by the percentage smears without EC present, but the result would rather have been attenuation of our differences reported. Cervical abnormalities may occur in the region of the endoectocervical junction.
Judging completeness of a Pap smear, the presence of endocervical cells on cytological reporting is considered important. The presence of these cells is routinely used to compare quality of smears between groups of patients. If more patients in one group have incomplete smears (endocervical cells not seen), such as with the HIV-infected group in this study, it means that cervical lesions could have been missed more often in the HIV-infected group. In spite of the HIV group having more smears with no endocervical cells present, there is the difference in outcomes described. Without the possible attenuation of effect, the results could have been more pronounced.
For completeness of excision, we set strict criteria at LSIL present at any margin to agree with previous reports. 12 Completeness overall was low, and also significantly lower in HIV-infected women. However, comparing only the excisions reported as either complete or incomplete, treatment failure occurred more in HIV-infected women. Incomplete excision in HIV-infected women may be due to extensive HPV infection caused by their immunocompromised state, and may explain the higher excision treatment failure.
Also, our study may be subject to a selection bias toward HIV-infected women entering care earlier. For HIV-infected women, local guidelines request referral for colposcopy evaluation after their first LSIL. In addition, Pap screening is available free to all women over the age of 30 years, but HIV-infected women qualify for this benefit regardless of age. The younger age at which HIV-infected women underwent first excision treatment reflects referral policy but does not necessarily implicate faster progression of low-grade lesions.
We included women of unknown HIV status in our analysis. The clinical significance of including the HIV unknown group is high. As can be seen in the total patient numbers, this group is larger than the HIV-negative group. The reason is that HIV testing for the largest part of the study period was not routinely done for women with cervical dysplasia. Importantly, the study did not find increased risk for recurrence of SIL post-excision in the HIV-unknown status group compared with the HIV-uninfected group.
In conclusion, our data suggest that careful follow-up should be maintained after cervical excision treatment, especially in countries with high HIV/HPV prevalence. Women on ART may be expected to have overall better excision treatment outcome and this supports earlier initiation of ART in vulnerable communities than current guidelines stipulate. The poorer outcome in HIV-uninfected patients than previously observed implicates incident HIV infection and review of HIV status in areas of high HIV/HPV prevalence should occur more regularly.
Footnotes
Acknowledgements
MZ, M LG and MvS are supported in The ANOVA Health Institute's ShareCare programme by the US President's Emergency Plan for AIDS Relief (PEPFAR) program and the US Agency for International Development, (USAID) under Cooperative Agreement No. 674-A-00-08-00009-00. J N is supported by The United States National Institutes for Allergy and Infectious Disease (NIAID-NIH), Division of AIDS (DAIDS): K23 AI 068582-01; The US PEPFAR Grant Award, T84HA21652-01-00 for Medical Education Partnership Initiative (MEPI); The European Developing Countries Clinical Trial Partnership (EDCTP) Senior Fellowship Award: TA-08-40200-021 and the Wellcome Trust Southern Africa Consortium for Research Excellence (SACORE): WT087537MA.