
Abstract
Care pathways, also known as clinical pathways, critical pathways or integrated care pathways, are used all over the world. Although they are used internationally, there are still a large number of misunderstandings. The goal of this paper is to provide an overview on the history of pathways and how pathways are actually perceived and defined. Pathways are more than just a document in the patient record. They are a concept for making patient-focused care operational and supporting the modelling of patient groups with different levels of predictability. Pathways are a method within the field of continuous quality improvement and are used in daily practice as a product in the patient record. This paper explains these different issues and provides an extensive list of references that should support pathway facilitators, clinicians, managers and policy-makers in their search for excellence.
The international phenomena of safety, quality and efficiency
Patient safety, quality of care and efficiency of health-care procedures are international phenomena. In 1991, Brennan et al. 1,2 concluded that a substantial amount of injury to patients occurred due to health-care management and that many injuries resulted from substandard care processes. One of the most cited reports on this topic was published in 1999 by Kohn et al. 3 of the Institute of Medicine (IOM): ‘To err is human’. Since then, other authors from all over the world have also published similar results on adverse events. 4–8 The first and fundamental ethical principle in health care – do no harm – is now being taken seriously by a wide constituency. 9 Five years after the IOM report, in 2004, Altman et al. 10 concluded that many promising efforts had been launched; however, the task is far from complete. 11
Although adverse events are not uncommon in hospitalized patients, they are by no means inevitable. 12 Even if a direct relationship is difficult to establish between variations and errors, reducing variations by standardizing clinical processes is an effective tool to minimize the probability of medical errors. 3,11 Improvements in health care require the active participation of not only physicians, but also all health-care workers. Recently, Batalden and Davidoff stated that: ‘Everyone in health care really has two jobs when they come to work every day: to do their work and to improve it!’. 11,13
Porter and Olmsted Teisberg 14,15 stated that health care should change and that the purpose of health-care systems is not to minimize costs, but to deliver value for patients, which in the long run results in better health per dollar spent. Three principles should guide this change: (i) delivering value to patients should be a goal; (ii) medical practice should be organized around medical conditions and care cycles; and (iii) results – risk-adjusted outcomes and costs – must be measured. With respect to this change, the role of the multidisciplinary team is to focus on clinical process innovation (CPI). 16–18 CPIs are central to the ability of organizations to negotiate the challenges of cost containment and quality improvement; yet, many CPIs have not met expectations to improve these primary processes. 17 Well-organized care processes, medical conditions or care cycles lead to appropriate outcomes if they include a structured context and a well-functioning multidisciplinary team. 19
The origin and definition of pathways
Health care continues to change towards more patient-focused care. The organization of the care process related to quality, efficiency and accessibility is one of the main areas of interest in the next few years for clinicians, health-care managers and policy-makers. The main method to (re)organize a care process is the development and implementation of a care pathway. 11,18,20–33 Care pathways, also known as clinical pathways, integrated care pathways or critical pathways, are used worldwide for a variety of patient groups. 18,20–23,27,30,31,34–38 They originate from industrial processes and were introduced in health care in the early 1980s in the USA. 23,37,39–43 The development, implementation and evaluation of care pathways represent one of the structured care methodologies next to, for example, guidelines, protocols and case management. 22,35–37,44–47 Nowadays, care pathways are being implemented as a method for monitoring processes and processing time, in a wide range of health-care systems, primarily to improve the efficiency of hospital care while maintaining or improving quality. 34–37,40,48–53 The first systematic use of clinical pathways took place between 1985 and 1987 at the New England Medical Center in Boston (USA) in response to the introduction of Diagnosis-Related Groups (DRGs) in 1983. 11,40,41 Typically, a reference length of stay and a budget are assigned to each DRG. In the late 1990s, more than 80% of US hospitals used at least some pathways. 54
In the UK, pathways were introduced in the early 1990s. 41,55 Clinical pathways, or integrated care pathways as they are called in the UK, are primarily considered to be the tools for designing care processes, implementing clinical governance, streamlining delivered care, improving the quality of clinical care and ensuring that clinical care is based on the latest research. 56–59 From the late 1990s to the beginning of the 21st century, pathways were disseminated all over the world. 23,37,41 Nowadays, pathways are used worldwide as one of the tools to structure or design care processes and improve them within the patient-centred care concept. 11,23,37,41,45,52,53,60 In most countries, the prevalence of pathways is still rather meagre, especially when one considers the idea that the care of 60–80% of patient groups in general hospitals should be suitable for pathway use. 11,23 When developing the pathway for these patient groups, one needs to take into account the evidence-based key interventions, the interdisciplinary teamwork, the patient involvement and the available resources. 11,18,20 Therefore, it is clear that introducing pathways in an organization and developing, implementing and evaluating individual pathways is a complex intervention.
In response to this complex challenge, the European Pathway Association (E-P-A) 23,33,42 adapted the definition as suggested in Vanhaecht et al. 20 and nowadays define a care pathway as: ‘A complex intervention for the mutual decision making and organization of predictable care for a well-defined group of patients during a well-defined period. Defining characteristics of pathways include: an explicit statement of the goals and key elements of care based on evidence, best practice and patient expectations; the facilitations of the communication and coordination of roles, and sequencing the activities of the multidisciplinary care team, patients and their relatives; the documentation, monitoring, and evaluation of variances and outcomes; and the identification of relevant resources’.
A care pathway is not defined as a document or a tool but as a ‘complex intervention’. 18,20,28,32,61–64 The Medical Research Council states that complex interventions in health care, whether therapeutic or preventive, comprise a number of separate elements that seem to be essential to the proper functioning of the intervention, although the ‘active component’ of the intervention that is effective is difficult to specify. 62 If we were to consider a randomized controlled trial of a drug versus a placebo as being at one end of the spectrum, then a comparison of a stroke unit to traditional care could be considered as being at the most complex other end of the spectrum. The greater the difficulty in defining precisely what exactly the ‘active component’ of an intervention is, and how they relate to each other, the greater the likelihood that you are dealing with a complex intervention. 62–64 Pathways are more similar to the complexity of stroke units than to the simplicity of giving a single drug. When developing and implementing a care pathway, active ingredients of the complex intervention include the multidisciplinary teamwork, understanding the practical organization of care and the integration of a set of evidence-based key interventions and outcomes.
Because of this complexity it becomes clear that pathways are more than just a piece of paper or a file in the patient record. 18,20,24 Care pathways are a concept to introduce patient-focused care. Different models of pathways exist, and they are a methodology to support the quality and efficiency improvement process and are made operational on different aggregation levels. 18
Pathways are more than just a document in the patient record; they are a concept, model, process and product
The concept of introducing patient-focused care
The goal of care pathways is to introduce and make the patient-focused care concept operational. Although ‘patient-focused care’ can be found in nearly every mission statement of a hospital, rehabilitation centre or primary care organization, it is not always put into practice. The patient-focused concept requires real patient-focused care, which means a disease-specific orientation and involving patients as real partners. 33 Nowadays, more and more hospitals are changing towards service line organizations, where the patient group is a key unit of organization. The Institute of Medicine stated in their publication, ‘Crossing the Quality Chasm’ (2001), 19 as one of the first steps to enhance the quality and safety of healthcare organizations: ‘Organize and coordinate care around patient needs. The primary purpose of identifying priority conditions is to facilitate the organization of care around the patient's perspective and needs rather than, as in the current system, around types of professionals and organizations’. 19,33 In the British Medical Journal, Degeling describes the relation between medicine, management and modernization as ‘a dance macabre’. He argues that pathways can help in the integration of different professional groups because in this model the patient group is the central focus. 47 Next to this disease-specific orientation, seeing patients as real partners will become even more important. ‘Every patient is unique, so deal with their needs as they come up and move them onto the next step’. This is one of the traditional rules to providing access to health care, as described by Rogers et al. 65 The new rule will be that every patient is unique, but they have enough in common to ensure that care pathways are a useful norm, and patients and clinicians are able to make choices that differ from these pathways as needed. 33,65 To protect pathways against this fear and to build patient-centred pathways, we need to involve patients as real partners in the development process. Wensing and Elwyn 66 provide an interesting overview of different methods to incorporate patients' views into health care. Although patient satisfaction questionnaires are one of the most widely used tools, more in-depth methods could be employed for pathway projects. Open interviews with patients and relatives or performing walkthroughs together with a patient or by a clinician acting as a mystery patient will provide useful information for the pathway development team. 33
Different models of care pathways exist
Care pathways are a model to standardize and follow up patient-focused care. They combine a variety of methods from quality improvement and operational research used in industry and health care. When using or translating these methods, two issues are important: the level of predictability of the care process and the level of agreement between the members of the multidisciplinary team. 18,35 Based on these two issues, three different coordination mechanisms can be described: chain models, hub models and web models (see Figure 1). 18
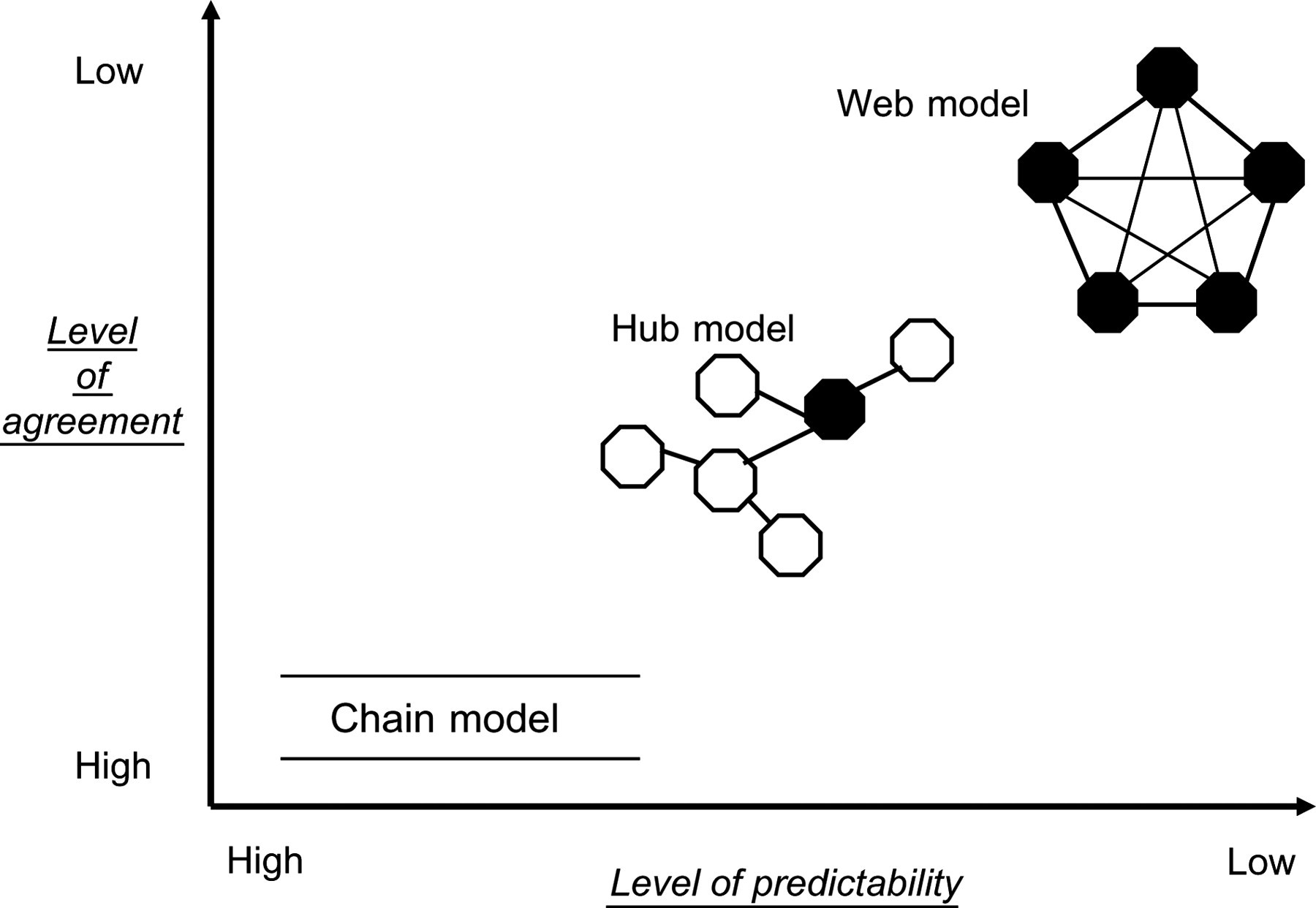
Chain models are used for high predictable care processes with a high level of agreement between the team members. We find this mechanism for example in elective surgery or chemotherapy processes. For these processes, pathways can be used as time–task matrixes, also called Gantt charts. 39 The sequence of the timing will mostly be day-by-day. For some more critical care processes, half days or hour-by-hour timings will be used to describe the timing of the process. Hub models are used for less predictable processes like internal medicine, rehabilitation, psychiatry and also within palliative care processes. In these models a key person or case manager will lead the organization of the care process and can use chain models for the high predictable subprocesses. Web models are used for unpredictable care or care processes where it is necessary to have daily team meetings to be able to organize and structure the process. 18 In web models the ‘time’–task matrix can be changed into a ‘goal’–task matrix. If the time sequence is kept, the day sequence can be changed in weeks. Examples are complex diagnostic admissions or pathways for patient groups with several important comorbidities.
One of the goals of each of these models is to enhance the interdisciplinary teamwork. 18 The importance of appropriate teamwork should not be underestimated. Gittel et al. 67 analysed the relation between good teamwork and patient outcomes and found positive results. Vanhaecht et al. 20,26 found similar results in 2007. As already described in a previous section (see pathways as a process), the team needs to develop the pathway taking into account the content and organization. Care pathways are – as stated in the definition – interdisciplinary. Different professional groups (doctors, nurses, allied health professionals, etc.) need to interact and decide how they will organize the care process and who is responsible and will take the lead in which part. How this challenge is managed will also depend on the level of agreement and predictability as described above (see Figure 1).
Chilingerian and Clavin 68 describe the concept of temporary teams, where for every patient a temporary team is formed, under the supervision of a clinical lead (medical doctor) and in which the team members are detached from their own professional group or service. When structures are built around these temporary teams and specific resources are invested, the temporary teams may become focused teams (stroke team, total knee team, palliative care team). 69 The interdisciplinary pathway team needs to focus on common goals, describe the different roles of the team members, and the communication, coordination mechanisms and processes that will be used. 70 Nelson and Batalden 71 discuss clinical microsystems. A clinical microsystem is a small, interdependent group of people who work together regularly to provide care for specific groups of patients. This small group is often embedded in a larger organization. Formed around a common purpose or need, these groups may comprise discrete units of care, such as a neonatal intensive care unit or a spine centre. A general clinical microsystem includes, in addition to doctors and nurses, other clinicians, some administrative support and a small population of patients, with information and information technology as critical ‘participants’. 71 Within a care pathway, different clinical microsystems can be defined. The number of people within each microsystem or the number of microsystems within each organization or pathway will differ from organization to organization and model to model (see Figure 1). 18
The quality and efficiency improvement process
Care pathways are also a process on their own to develop and implement well-organized care and to improve quality and efficiency. 18,20,21,24 In literature, different methodologies are described but basic principles are found in all appropriate methodologies. 11,23,33,35,41,43,72,73 Active ingredients of the complex care pathway intervention are the feedback on the actual organization of the care process, the availability of evidence-based key interventions and outcome indicators, and the continuous quality and efficiency improvement process that takes place within the multidisciplinary team. Recent multicentre research describes that during the pathway development, even before the implementation of the pathway, the organization of the care process can be improved. 20,26 Over time the team will improve the quality and efficiency of the care process by analysing the actual organization and performance of the care process. Based on the bottlenecks, the team will improve the process by using the plan–do–study–act cycle for continuous improvement with respect to patient characteristics and expectations. 20,74 The changes in the organization of the care process are standardized by implementing the pathway product (see Figure 2). 20
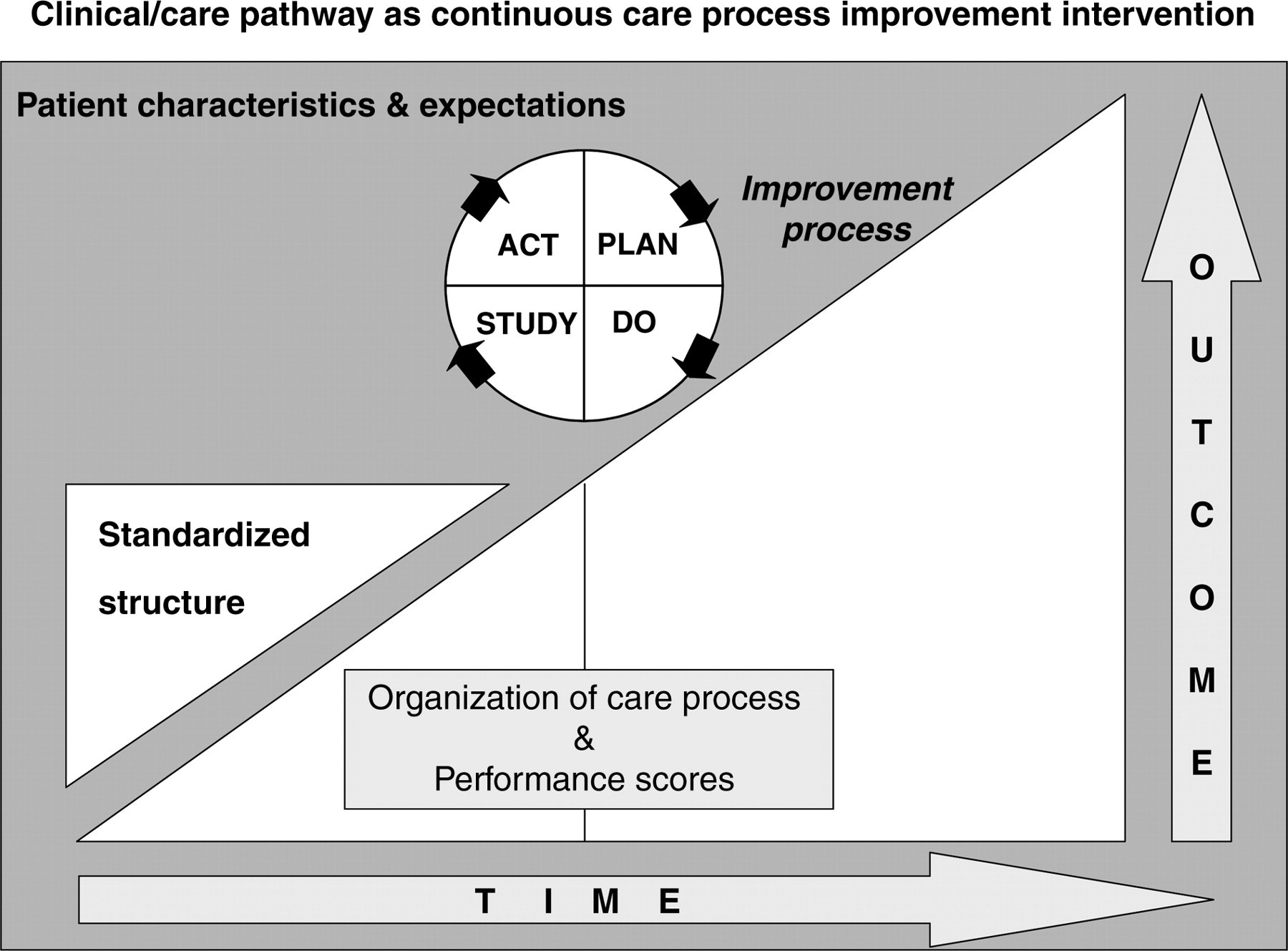
Pathway continuous quality and improvement process 20
To improve the organization, the involvement of the multidisciplinary team will be necessary. Enhancing teamwork is seen as one of the main processes that lead to the improvement of care pathway outcomes. The development of a pathway asks for real teamwork. 33 ‘Pathways make teams work’ is one of the quotes often used during pathway conferences and even in literature. The impact of care pathways on the multidisciplinary teamwork is described in vast amounts of literature but mostly only in words. There is a lack of hard proof on this management issue and it is time to find out what the impact of pathways on teamwork really is. Recently, David Bates et al. 75 published a list of global priorities in patient safety research. When they consider only the developed countries, the most important area for research is the lack of coordination and communication, followed by latent organizational failures and poor safety culture and blame-oriented processes. 75 A study on the impact of clinical pathways on the organization of care processes 26 revealed that teams who have a pathway to support the care process have significant higher scores on the coordination of the care process than teams not using pathways (odds ratio 8.92, confidence interval [CI] 1.52–95.38). 20,26 Also on the follow-up of the care process, a significant odds ratio of 5.56 (CI 1.80–20.36) was found. 20,25,26 In the overall organization of the care process, measured with the Care Process Self-Evaluation Tool, 25 an odds ratio of 4.26 (CI: 1.40–13.61) in the benefit of pathways was found. 20,26 A multicentre study on joint arthroplasty patients, including 39 care processes and 737 consecutive patients, revealed the statistical interaction effect between pathways and the coordination of the care process as determinants for length of stay and elapsed time to discharge. 20,76 Most of these effects are seen in observational studies. Additional research will be necessary to prove the relation between pathways and coordination. The E-P-A is actually organizing an international cluster randomized controlled trial on chronic obstructive pulmonary disease and proximal femur fracture patients to explore the impact of pathways on these two patient groups. One of the focuses in these trials is the impact of pathways on multidisciplinary teamwork. 77,78
One of the most important pitfalls in pathway development from a clinical point of view is the absence or lack of evidence-based key interventions and outcome indicators. 11,33 During the pathway development process, the team needs to review the available literature on the specific clinical topic. Although this can be a very time-consuming process, it is one of the most important challenges for the future. 33 Pathways are used to standardize outcome-oriented care, but the content of the pathways is not always clear and is frequently described vaguely in pathway literature. Pathway appraisal instruments describe the development of the pathway, the organization of the care process or the pathway document, but they rarely evaluate the content of the path. 24 This problem does not only occur in the field of care pathways, but also within the area of clinical guidelines, where the AGREE instrument also does not evaluate the content of the guideline. 24,79
One of the possible reasons why some pathways do not lead to an improvement in quality and/or efficiency is the quality of the content. Therefore references to the literature and guidelines should be used in pathways. Websites like
Evidence-based indicators need to be used in the pathways. To develop a pathway is one challenge but to keep pathways alive is a very difficult exercise. To keep pathways alive, clinicians, managers and, why not patients, should be frequently provided with hard data on outcomes. A framework for pathway indicators is the Leuven Clinical Pathway Compass in which five domains are defined: clinical indicators, process indicators, financial indicators, team indicators and service indicators.
80
Pathway facilitators could use the indicator clearing house (comparable to the guideline clearing house) (
The pathway product has four aggregation levels: the model pathway, the operational pathway, the assigned pathway and the completed pathway
Next to pathways as a concept, a model and a quality and efficiency improvement process, we have to describe pathways as a product. The pathway product is of course an important item; however, without the pathway concept, process and method, the product is nothing. This means that buying pathways without translating them and adapting them to the specific organization and team could be unsafe and ineffective. The pathway product is mostly seen as a file in the patient record. 44,83 This patient record is mostly paper-based, but examples can be found of electronic supported pathways. 42,84 Five types or four levels of aggregation of pathway products can be described: the model pathway, the operational pathway, the assigned pathway, the completed pathway and the patient version of the pathway, which is a combination of the operational–assigned–completed pathway in patient language (see Figure 3). 18
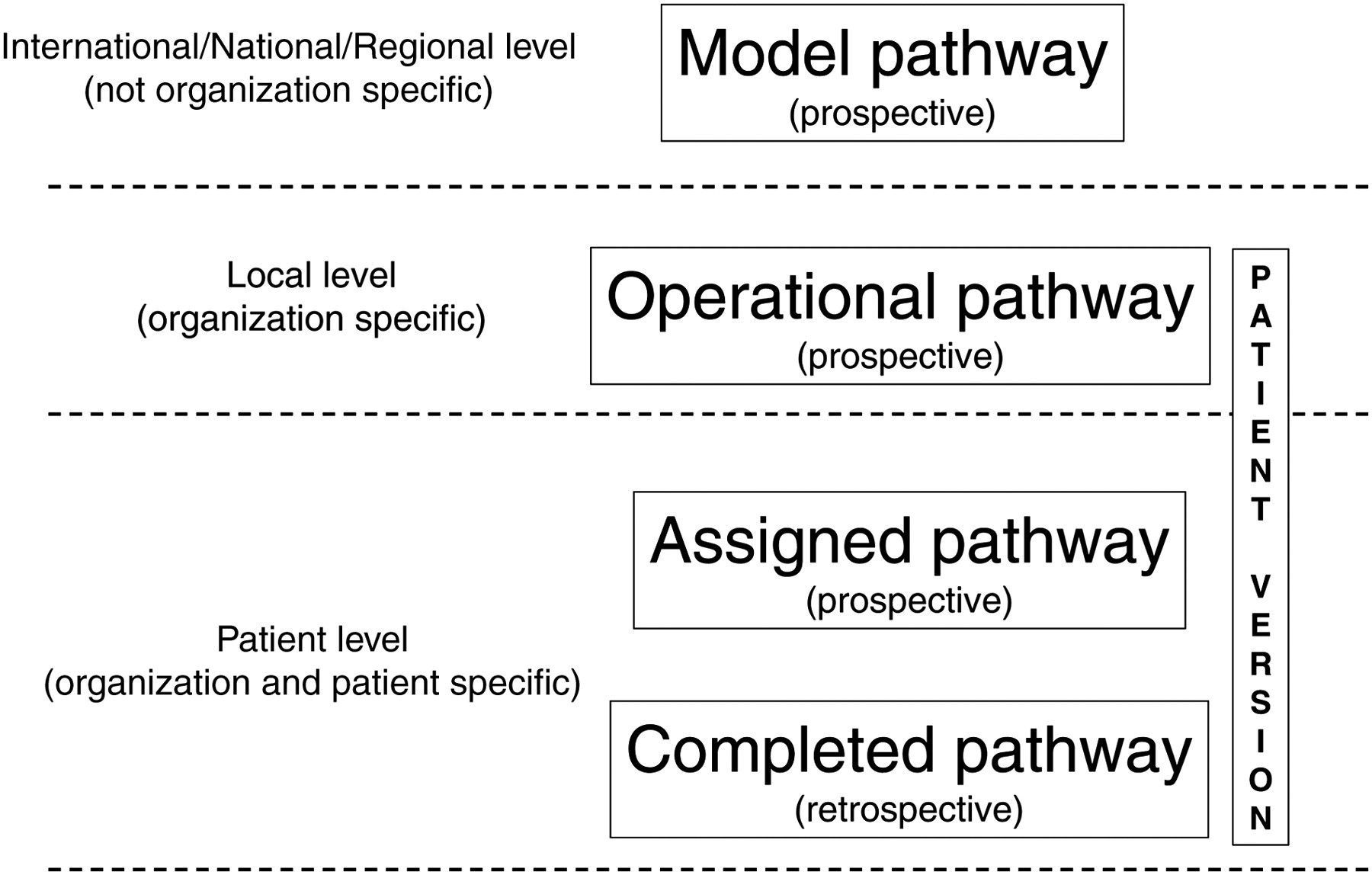
The model pathway is the most aggregated level. This pathway is based on the available international and national evidence. It is not organization specific and lots of guidelines that also describe the organization of the content could be called model pathways. The operational pathway is the pathway that is developed by a specific organization taking into account the information from the model pathway and the characteristics from the specific organization (available competences, resources). This pathway is organization specific because of the differences between different organizations. The assigned pathway is the pathway that is used for a specific patient and is the pathway that is based on the operational pathway and adapted to the needs of a specific individual patient. The completed pathway is the path that can be reviewed ex post facto, after the discharge of the patient. The difference between the completed pathway and the operational pathway provides information about the variances and the level of compliance to the key interventions in the path. 21 Based on this information, the pathway can be revised and further improved. A last type of pathway is the patient version of the pathway to inform and involve the patient and family about the process of care. Most of the time the patient version is based on the model and operational pathway and can also be used as a communication instrument between the patient – family – and the multidisciplinary team. 11,18,20
Are we there yet?
Pathways are complex interventions that are more than just a piece of paper. They are developed by a multidisciplinary team of clinicians and managers and need to be based on the latest evidence from literature, operational research and patient involvement methodologies. Pathways are not something that can be developed overnight. Pathways need to be developed and implemented with patient-focused care paradigm as the main driver. Different models of pathways can be implemented based on the level of predictability of the care process and level of agreement within the team. Evidence-based key interventions and outcome indicators are and will remain an important and difficult issue in health-care management. Discussions about the importance of clinical activities or the issue that supporting care is more important will remain a main issue. All interventions in the pathway need to be discussed among the different team members so that they can lead to shared goals, clear roles, and understandable communication and coordination procedures. Only in this way can the team become a high performing team. Next to the relation between the professional team and the individual patient, special attention also needs to be given to the patient's family. A patient and family version of the pathway, based on the model and operational pathway, should be an important by-product for care pathways.
We hope that the above-described history and concept of care pathways as complex interventions will prove informative. However, it is not possible to learn what pathways are by just reading this article; it is necessary to start projects. When planning, performing and evaluating projects, it is important to keep in mind the basic principles that were discussed in this article.