
Abstract
Summary
George James Guthrie (1785–1856) was a British military surgeon who came to prominence during the Napoleonic Wars (1803–15). He wrote several books on military surgery and was President of the Royal College of Surgeons of England three times. However, his most innovative and important achievement has largely gone unrecognised by modern historians. In 1814, at the battle of Toulouse in the Peninsular Campaign, he performed a landmark early trial of the treatment of musket wounds to the thigh. Here we not only discuss this clinical trial and place it in its social context, but also present the pathological skeletal specimens of two wounded British soldiers who took part in it.
Introduction
Past biographies of George James Guthrie have aimed to show the important role this surgeon had in Georgian Britain. Using information from his own books and articles and from his obituary, modern readers are now more aware of his exploits in Canada, the Napoleonic Wars, at the Royal College of Surgeons and in London hospitals.1–4 However, arguably his most important achievement has not been discussed at all – his clinical trial of the treatment of musket wounds to the lower limbs in 1814.
Guthrie was by no means the first British doctor to conduct a clinical trial. James Lind's (1716–94) controlled trial of the treatment of scurvy in 1747 5 and Edward Jenner's (1749–1823) trial of vaccination with cowpox to prevent smallpox in the 1790s 6 are notable examples that predate Guthrie. However, such trials were still rare in medicine during the early 1800s; they were very rare in the field of surgery and particularly rare in the pressured environment of the battlefield. It was at the Battle of Toulouse that Guthrie attempted to determine the optimal surgical technique for treating gunshot wounds to the thigh. This study had a major impact upon the approach to projectile wounds taken by military surgeons during the 19th century.
The Battle of Toulouse (1814)
The Sixth Division next came up,
within the range of shot;
And shot and shells mow'd down our ranks,
they play'd so dreadful hot;
But still we march'd undauntedly,
although our men did fall;
Resolv'd when we came up to them
to pay them once for all. 7
This verse of a song written by a British soldier at the Battle of Toulouse vividly highlights the wounds sustained by those young men who took part. The battle took place on 10 April 1814 (Figure 1). 8 The French army was under the leadership of Marshal Soult (1769–1851), and had been pursued across Spain and southern France by combined British, Spanish and Portuguese forces under General Wellington (1769–1852) until besieged in Toulouse. Toulouse was an important supply centre for the French army and an obvious target for the British army who were hungry and exhausted. It was the last major battle of the Peninsular War and, with hindsight, is known to have been unnecessary as Napoleon had already abdicated four days previously. 9 Guthrie was the chief British military surgeon at the battle. It was only here, once he had gained years of experience in the campaign, that Guthrie felt able to undertake his trial.
Georgian illustration of the Battle of Toulouse by JC Stadler, 1818 (reproduced courtesy of the Council of the National Army Museum, London)
Investigating the clinical trial
This investigation was triggered by our identification of the skeletal remains of two British soldiers injured in the battle and curated in the Imperial College London Pathology Museum at Charing Cross Hospital. The specimens were a right femur from one individual (code W.0238), and the left femur and tibia from another individual (code W.0624). The museum cards for both cases were written in the 1800s (the style of card was changed in 1900). On one card it was stated that Guthrie donated the specimen to the pathology museum at the Westminster Hospital. With the closure of the Westminster Hospital the specimens were moved to the Charing Cross Hospital Pathology Museum, which is now part of the Imperial College London.
Textual sources for this study concentrate on Georgian medical texts and military accounts of the Napoleonic Wars. The works of military surgeons active during the Peninsular Wars, in particular at the Battle of Toulouse itself, were consulted. The aim of studying these textual sources was to allow the construction of the probable care received by each soldier and to investigate the effects of Guthrie's clinical trial on open femur fractures that took place on the wounded British soldiers after the battle.
Despite the large numbers of dead and wounded in the Napoleonic Wars, surprisingly little palaeopathology has been published from this conflict. A brief paper has noted the existence of wounds in a Peninsular War military hospital cemetery at Tolosa in Spain but it goes into very little detail. 10 A mass grave dating from the Napoleonic period (1812) has been noted at Vilnius in Lithuania11,12 but papers discussing wounds have not appeared. A good series of pathological specimens from the Battle of Waterloo (1815) has been described as part of a larger work on weapon injuries from the first half of the 19th century. 13
Guthrie's description of his trial
Typical battlefield treatment for compound fractures of the lower limb was recorded in the written works of British surgeons who worked in field hospitals in the Napoleonic Wars.14,15 Charles Bell (1774–1842) painted the wounds of many of Wellington's soldiers and this also helps us to understand the injuries from a modern perspective. 16 There were apparently 1359 British sick and wounded at the battle and medical staff at the battle was comprised of two deputy inspectors-general, 10 staff surgeons, six apothecaries and 51 assistant surgeons. 17 In the period 10 April to 28 June 1814, records show that 1242 soldiers were treated in the General Hospital at Toulouse. Of these 146 died, 306 were discharged to duty and 790 transferred to Bordeaux. 18 George Guthrie was the chief British surgeon at the battle and wrote several books on the management of such wounds; his work On Gun-shot Wounds of the Extremities Requiring Different Operations of Amputation, with their After-Treatment was published just one year after this battle. 19 In contrast to injuries elsewhere, he recommended that all compound fractures of the thigh were amputated early without attempting to preserve the injured limb. However, at that time he did not give the details of exactly how he came to this conclusion. It was only in a later work, Commentaries on the Surgery of the War in Portugal, Spain and France and the Netherlands, that he described the trial that enabled him to reach this conclusion. 20
Guthrie's inclusion criteria for the trial were projectile wounds to the thigh with femoral fracture but limited soft tissue loss, which he termed the best cases available. He removed the musket balls surgically, cleaned the wound and splinted the leg with traction. There was no randomisation nor was there a control group as we might expect in modern trials. Nevertheless, for his day this was an innovative approach to take in the challenging situation of the military campaign. Guthrie wrote:
An arm or a leg, as a general rule, is not to be amputated in the first instance for a compound or gun-shot fracture. An effort should always be made to save it; and, under reasonable circumstances with regards to the extent of the injury, the comfort, climate and ordinary good health of the sufferer, the object will usually be obtained, under good surgical treatment.
It is not so with the thigh. After the battle of Toulouse, 43 of the best of the fractures of the thigh were attempted to be saved under my direction. Of this number, 13 died, 12 were amputated at a secondary period, of whom seven died; and 18 retained their limbs. Of these 18, the state three months after the battle was: five only could be considered well, or using their limbs; two more thought their limbs were more valuable, although not very serviceable, than a wooden leg; and the remaining 11 wished they had suffered amputation at first. 21
Guthrie set up his trial to determine whether he could preserve the limbs. Men treated with limb conserving surgery had a very poor outcome. In his group 47% (20 of 43) died. Only 12% (five of 43) were left with a useful limb and were satisfied with their outcome. Since he found that the results of early amputation were much better than this, the recommendation that all such injuries underwent early amputation became widespread practice in the British army. 22
Guthrie also noticed something shared by all those who survived to have a useful leg. It seems that the location of the original injury was a major determinant of the outcome in his trial: ‘In the five successful cases, the injury was in all at or below the middle third of the thigh. In the 13 others who retained their limbs, the injury was not above the middle third’. 23 The closer the injury was to the knee, the more likely the soldier was to survive. Injuries up near the groin had less chance of survival.
Amputated limbs from the trial
The two cases from the battle are considered with regard to the likely cause of the injury, the weapons that may have been used and the long-term physical disability.
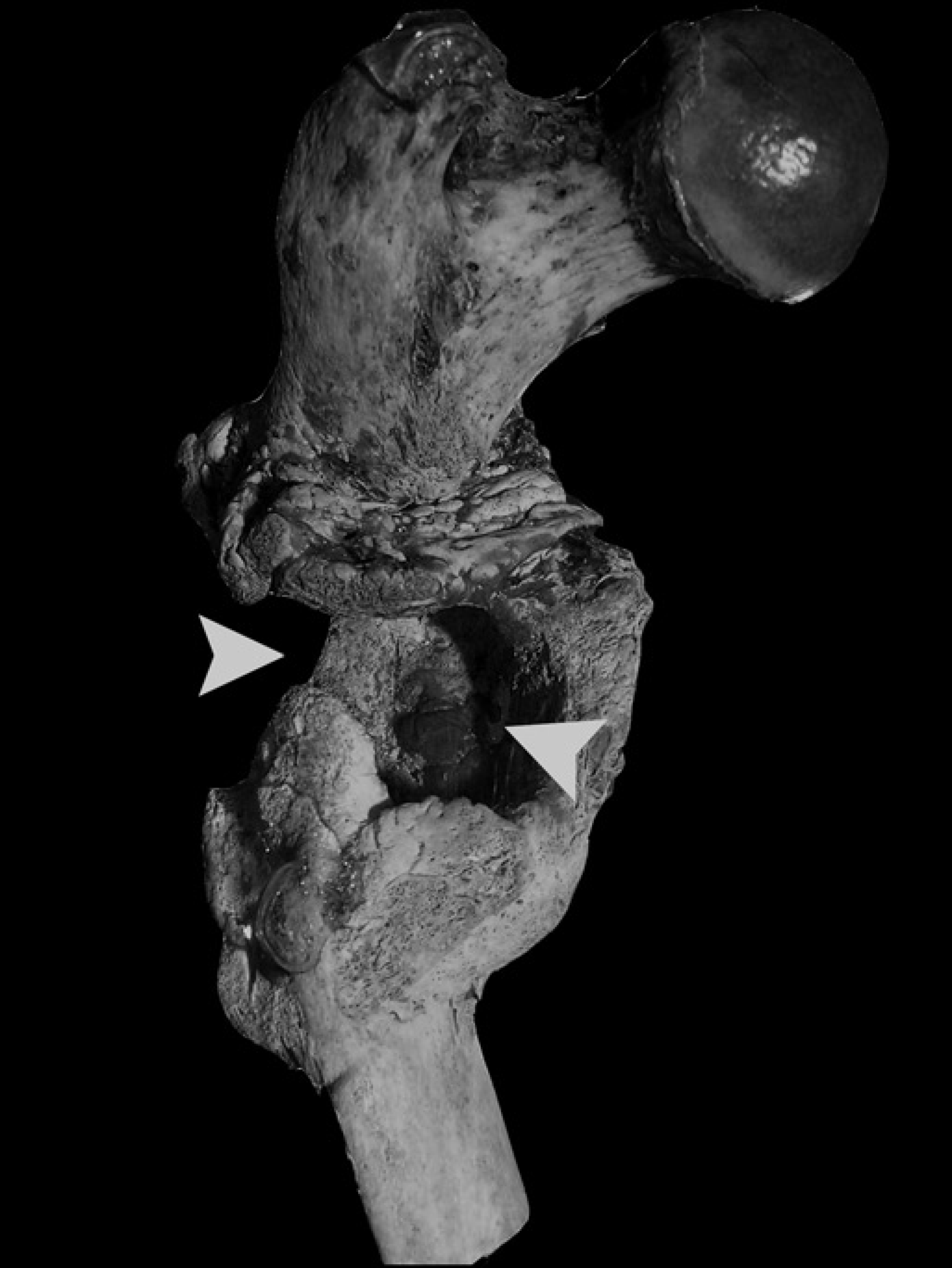
In both specimens there is evidence for a penetrating injury to the thigh during the battle. In the first case (code W.0238) the right femur was fractured and a section is absent (Figures 2 and 3) and in the second case (code W.0624) the medial aspect of the distal left femoral cortex is absent (Figure 4). Evidence for infection is found in the widespread pitting, new bone formation on the bone surface (involucrum) and holes in the bone through which pus would have drained (cloacae). The second case also had septic arthritis of the knee, since the joint was fused solid.
Posterior view of proximal femur of case 1. Left arrow shows area where a section of the femoral shaft has been destroyed, either by the projectile or by the subsequent infection. Right arrow demonstrates the location of an infected cavity bounded anteromedially by callus
Lateral view of case 1. Arrow shows rounded-off stump of distal femoral shaft. Note also malalignment of proximal and distal femoral fragments
Anteromedial view of case 2. Note the knee fused in flexion and the defect in the distal femoral shaft (arrow)


The projectiles that caused these injuries could have originated from a variety of different weapons. Records from the Napoleonic Wars describe the use of small arms, such as muskets, and artillery with a variety of projectiles. French muskets of the time were the 1777 model and fired a lead ball of .70 calibre. Cannons fired round shot, grape shot, chain shot, bar shot and spherical case shot. 24 The destruction caused by the projectiles appears too limited to be round shot, chain shot or bar shot from a canon. These tended to remove the entire limb from the site of impact distally. The injuries could have been caused by one single musket shot or by a projectile from a grape shot. However, the overwhelming popularity of the musket increases the probability of the wounds being caused by a musket ball.
The question arises as to whether these two cases were early amputations or members of the limb conservation group in his trial. Analysis of the bones shows that there has been considerable healing in both cases, with callus bridging the defect in the first case and fusion of the knee in the second. This suggests that both these soldiers survived the immediate aftermath of the battle without undergoing a primary amputation. The degree of healing implies the limbs were probably removed some months or perhaps years later. It is likely, therefore, that the two soldiers were part of Guthrie's trial on the limb conserving management of open femur fractures. 25
Consequences of the trial
So what did Guthrie himself think of the results of his trial and how did it affect his writings? He seems to have believed that it demonstrated clearly the best way to manage musket wounds to the thigh. One consequence of the evidence he found was that he felt able to recommend the early amputation of such injuries. At that time a surgeon may have been reluctant to amputate the entire leg before evidence of gangrene became apparent, hoping the patient might improve on his own. However, Guthrie showed that to wait was futile and actually increased the risk:
Every broken thigh or leg was in a straight position, and the success was greater than on any previous occasion. Nevertheless, with all these advantages, there can be little doubt that if amputation had been performed in the first instance, on the 36 of the 43 who died or only partially recovered, some 20 would have survived, able, for the most part, to support themselves with a moderate pension. 26
His ideas do appear to have been wholeheartedly adopted by other authors on military medicine writing in the first half of the 19th century. 27
While some of the disabled veterans from the Peninsular Wars were treated in the Royal Hospital at Chelsea, others would have received care at nearby London hospitals established for the use of the general public. Sir George Guthrie left the army after the Battle of Waterloo (1815) and took up a post as surgeon at the Westminster Hospital. 28 He also co-founded the Westminster Medical School. 29 It is likely these specimens in its pathology collection would have been used by him to teach the students. We may never know whether the specimens described in this paper were obtained by him by amputation during life or post mortem. We are also ignorant as to whether the procedures took place in France or London, although the degree of bone healing certainly suggests the latter. However, the connection with Guthrie explains how the specimens came to be donated to the Westminster Hospital pathology collection, later to be inherited by the Imperial College London Pathology Museum.
Guthrie was certainly not the perfect clinician, as demonstrated by the quite blatant criticism to be found in his obituary in the Association Medical Journal. 30 However, his clinical trial from the Battle of Toulouse was well ahead of its time, being groundbreaking due to its military context. It is perhaps for this trial, most of all, that he should be remembered.
Footnotes
Acknowledgements
We are grateful for the assistance of Dr Vin Chauhan, curator of the Imperial College London Pathology Museum at Charing Cross Hospital.