
Abstract
Dramatic improvement in the survival of the HIV population has occurred with the ascendance of highly active antiretroviral therapy (HAART). In the foreseeable future, HIV-infected women who acquired disease during the peak years of the epidemic are expected to survive to experience menopause and even years beyond. The HIV epidemic may be viewed as ‘mature’, as its earlier victims become part of the geriatric population. Research about the process of menopause in HIV-infected women and, conversely, about HIV infection in women undergoing menopause is currently limited. Existing research suggests that the process of menopause is affected by HIV infection, inasmuch as infected women appear to experience menopause at an earlier age, with greater symptomatology, and with different reproductive hormone profiles compared with HIV-uninfected women. HIV infection also appears to affect bone mineral density, cardiovascular disease and cognition, with some age-related interactions. Lifestyle and demographic factors have pervasive importance for both HIV infection and the menopause in women. This article reviews the current state of knowledge about the menopausal process in HIV-infected women, and the common conditions in postmenopausal women that are likely to be affected by HIV infection. Clinicians should appreciate the potential role of HIV infection in caring for menopause-aged women.
Introduction
Combination antiretroviral therapy has led to decreased AIDS mortality. 1,2 For women infected with HIV, this means that many may live to experience menopause. Menopause represents a complex transition in a woman's life, involving ovarian, hormonal, metabolic and social changes. 3 At times, symptoms associated with menopausal changes drive women to seek out medical care. 4 A sound understanding of the menopausal transition is crucial in developing plans for clinical management. Menopause in HIV-infected women may present unique challenges. 5 Although incident HIV infection rates are declining, women represent an increasing proportion of such cases. 6
Herein, we discuss the following topics as they relate to the special case of HIV-infected women: age at menopause, menopausal symptoms, reproductive hormones, bone mineral density (BMD), cardiovascular disease (CVD) and cognition. Avenues for future research are also discussed.
Age at menopause
Earlier age of menopause onset has been associated with increased risk for medical illnesses and increased mortality. 7–12 Self-knowledge of menopausal status allows a woman to anticipate her needs for contraception use and disease prevention measures. 13
Several investigators studying the effect of HIV on age at menopause have found significant reductions in the median age of menopause in their study populations. 13–16 Schoenbaum et al. 14 conducted a prospective study of 571 women, the Ms. Study, in which they found that HIV infection was independently associated with earlier onset of menopause. Moreover, within HIV-infected women, greater immunosuppression, low physical activity level and recent drug use were each independently related to a higher probability of menopause onset. In a sample of 96 HIV-infected Brazilian women, Ferreira et al. 15 found a median age at menopause of 47.5 years. In contrast, in the Study of Women's Health Across the Nation (SWAN), Gold et al. 17 found a median age at menopause of 51.4 years in a large, multiethnic, population-based sample.
Other investigators have found no significant distinction in the age at which HIV-infected women reach menopause. 18 Cetjin et al., in a nested cohort study of 1431 women, found a greater risk of prolonged amenorrhoea in HIV-infected women compared with uninfected reproductive-aged women. However, when levels of follicle-stimulating hormone (FSH) >25 mIU/mL were used to define menopause, an independent effect of HIV infection on age at menopause was no longer statistically significant. 13 Fantry et al. 18 surveyed 120 HIV-infected, largely African-American women and found a median age of menopause being 50 years. After comparison with other studies of HIV-uninfected women, they concluded that the age at menopause appeared similar between HIV-infected and uninfected women.
A variety of additional factors have been associated with earlier menopause, including current smoking, drug use, African-American ethnicity and lower education level, all of which are common among the HIV-infected population. 14,17,19,20
Taken together, these data suggest that there may be an independent effect of HIV infection in causing earlier menopause. It remains difficult to disentangle independent effects of HIV from lifestyle and demographic factors that influence the onset of menopause.
Menopausal symptoms
Symptoms characteristic of the menopausal transition include breast tenderness, vasomotor symptoms, insomnia, migraines, premenstrual dysphoria, genital atrophy and sexual dysfunction. 3
Some investigators have found no difference in menopausal symptomatology between HIV-infected and uninfected women. 21 Analysis of symptom attribution by 278 women from the Ms. Study showed no difference in prevalence of hot flashes or vaginal dryness between HIV-infected and uninfected women. 21
Other studies have found increased menopausal symptom prevalence in HIV-infected women. One study of Brazilian women of low socioeconomic status found increased prevalence of vasomotor, psychological, genitourinary and sleep-related symptoms among HIV-infected participants. 15 HIV-infected women were 65% more likely to report menopause symptoms than uninfected women. 15
African-American women report more vasomotor symptoms than women of other ethnic groups. 22 In comparison with HIV-uninfected, African-American women, Fantry et al. 18 found a higher prevalence of hot flashes and vaginal dryness among HIV-infected, African-American women.
Miller et al. 5 found that HIV-infected women were more likely to report menopause symptoms than uninfected women. Within HIV-infected women not using highly active antiretroviral therapy (HAART), lower symptomatology was associated with greater immunosuppression. 5 Similarly, in a small sample of 52 HIV-infected women, Clark et al. 16 found that higher CD4 counts were associated with greater prevalence of hot flushes. Other studies have demonstrated no association between CD4 counts and menopausal symptoms. 15,18
Studies addressing the suspected increase in prevalence of menopausal symptoms among HIV-infected women highlight the roles that age, socioeconomic status, ethnicity, drug use and overall well-being play in the presentation and attribution of menopausal symptoms. Johnson et al. 21 observed that women aged 45 years or older were more likely to attribute hot flashes and vaginal dryness to menopause than women less than 45 years old. They also observed that women who had at least graduated high school more commonly attributed vaginal dryness to menopause. 21 These effects associated with age and education were found to be important in perimenopausal but not postmenopausal women. 21
Ferreira et al. 15 found significantly greater vasomotor, psychological and genitourinary symptoms in women with a fair or poor self-perception of health status as opposed to good or excellent. Additional factors associated with menopause symptoms were age between 45 and 54 years and receipt of public benefits. 15
Miller et al. 5 did not find any association between recent drug use and menopausal symptoms, but they did find a linear increase in the odds of having menopausal symptoms with the number of negative life events and with depressive symptoms. In addition, mean number of menopause symptoms reported was higher for Hispanic women than for African-American or white women. 5
HIV-infected women may be more inclined to attribute their symptoms to health problems other than menopause. In the Ms. Study, HIV-infected women were more likely to be unsure of the cause of menopause symptoms, a factor that may lead to systematic under-reporting of menopausal symptoms by HIV-infected women. 21
Given the multifactorial nature of menopausal symptoms and the likelihood that HIV-infected women may attribute their symptomology to negative life-events or other illnesses, caretakers of these women should be proactive in their investigation of menopausal symptoms and offering of treatment, if necessary.
Reproductive hormones
The World Health Organization defines natural menopause as 12 months of amenorrhoea without any pathological or physiological cause, determined retrospectively. 23 In addition to the cessation of menses, however, are hormonal changes that have systemic effects. 23
The Stages of Reproductive Aging Workshop (STRAW) convened in 2001 offers a useful staging system for menopause. 24 Included in the staging system are some of the hormonal signs of reproductive change (Figure 1). 24
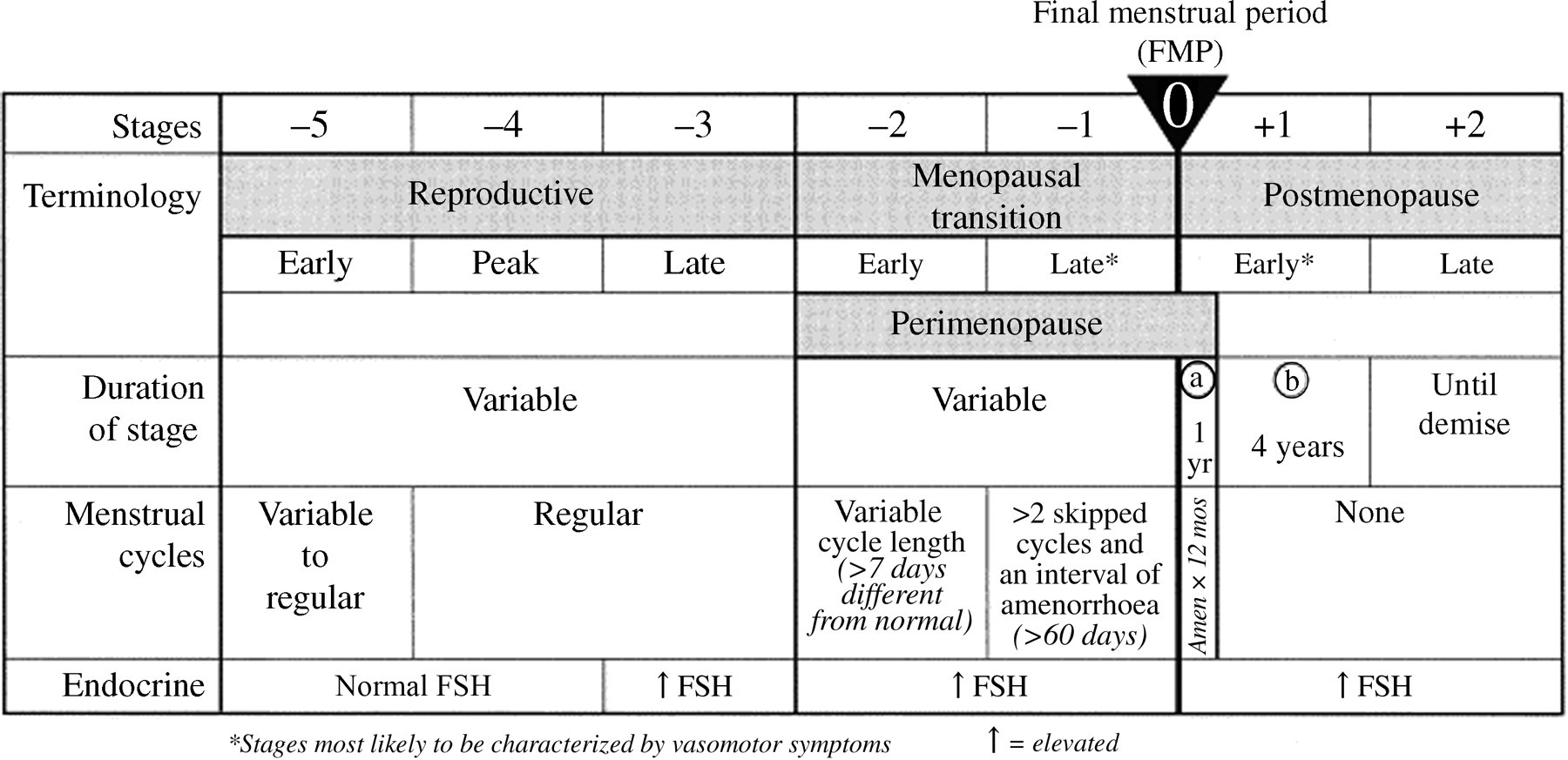
The Stages of Reproductive Aging Workshop staging system for reproductive ageing. Reprinted from Soules et al. 24 with permission from Elsevier Limited
Elevated FSH is an early and readily measurable sign of reproductive ageing. 24 This rise in FSH is caused by reduced production of inhibin B, which itself results from the dwindling of ovarian follicles. 24,25 Other predictable reproductive hormone changes that occur during the menopausal transition include increased luteinizing hormone (LH) and decreased estradiol and progesterone. 24
Santoro et al. 26 conducted a pilot study of 82 HIV-infected women and 15 HIV-uninfected women and found thyroid-stimulating hormone (TSH), prolactin and estradiol levels to be unaffected by HIV serostatus. In postmenopausal, HIV-infected women, FSH was reduced compared with uninfected women. 26 Blood was drawn from the 15 HIV-uninfected, control women between cycle days 3 and 5, representing peak FSH for normal, mid-reproductive-aged women. 26 Santoro et al. 26 also found that use of HAART was associated with higher FSH but not with changes in estradiol or prolactin. Drug use was independently associated with significantly higher prolactin and with decreased FSH. 26
In a larger sample of HIV-infected, substance-using women, Santoro et al. 27 found HIV infection to be associated with higher levels of estradiol and inhibin B. There was significant interaction between HIV infection and menopausal status. After multivariable analyses, FSH was increased in HIV-infected women during the late menopausal transition and postmenopause only, while LH was increased in HIV-infected women during premenopause only. 27 Among HIV-infected women, HAART use was associated with increased estradiol during the early menopause transition, and higher prolactin levels were seen with lower CD4 count. 27 Increased prolactin and decreased estradiol and inhibin B were observed with use of opiate drugs. 27 FSH was reduced with opiate use in postmenopausal women only. 27
Data on reproductive hormones in HIV-infected women remain limited. One thing that does seem clear from studies thus far is the need for caution in defining menopausal status by biomarkers such as FSH levels. Lifestyle factors, stress and drug use may all result in decreased FSH, such that menopause may fail to be correctly diagnosed or predicted. Care of HIV-infected women approaching or undergoing menopause should be guided by awareness of the difficulty of detecting traditional menopausal stages and of the potential for masking of progression through menopause.
Bone mineral density
Established risk factors for low BMD include age, ethnicity, menstrual function and body mass index (BMI). 28 In addition, several studies have consistently shown increased prevalence of low BMD among HIV-infected women nearing the age of menopause.
Dolan et al. 29 compared the BMD of 84 HIV-infected women with that of 63 HIV-uninfected women similar in age, BMI, ethnicity and age of menarche. HIV-infected women in the study had significantly less fat and greater histories of smoking, substance abuse and intravenous drug use. Reduced lumbar spine, femoral neck and total hip bone density was found in HIV-infected women compared with HIV-uninfected women. Osteopenia at either the hip or spine was present in 54% of HIV-infected women compared with 30% of uninfected controls (P = 0.004). In addition, HIV-infected women had decreased 1,25-dihyroxyvitamin D but increased urinary N-telopeptides of type 1 collagen (NTx) and serum osteoprotegerin (OPG). The investigators suggest that increased serum levels of OPG may reflect compensatory downregulation of bone resorption. Within HIV-infected women, BMD was significantly reduced among women with oligomenorrhoea or with an FSH > 15 IU/L. Dolan et al. 29 found no association between antiretroviral therapy and BMD.
Yin et al. studied 31 HIV-infected, African-American or Hispanic women older than 50 years with greater than one year of amenorrhoea. Comparison was made with 186 HIV-uninfected historical controls matched for age, ethnicity and postmenopausal status but with significantly higher mean BMI. Yin et al. found that HIV-infected women had significantly lower mean BMD at the lumbar spine and total hip. HIV-infected women also had significantly higher prevalence of osteoporosis in the lumbar spine and total hip. No association was found between BMD and duration or class of antiretroviral therapy, AIDS diagnosis, CD4 count or vitamin D deficiency. 30
In the Ms. Study (n = 495 women), the prevalence of low BMD was below national estimates for middle-aged women, likely due to the high proportion of African-American (54%) and overweight/obese (3/4 with a BMI > 25 kg/m2) participants. The study found reduced femoral neck and lumbar spine BMD in HIV-infected women vs. uninfected women. 31 Class or duration of antiretroviral use, duration of HIV infection and CD4 count were not associated with BMD. Arnsten et al. 31 also found that methadone treatment was independently associated with reduced BMD of the lumbar spine.
The pathogenesis of HIV-associated bone loss is still unclear but likely multifactorial. Chronic T-cell activation found in HIV-infected individuals promotes bone resorption via pro-inflammatory cytokines, such as tumour necrosis factor (TNF)-α, interleukin (IL)-6 and IL-1. 28,30,32 Secondary effects of HIV infection such as weight loss, hypogonadism and vitamin D deficiency likely play a role as well. 30 In the three studies just described above, no associations were found between antiretroviral medications and BMD. 29–31
Estrogen deficiency with the onset of menopause appears to exacerbate HIV-associated bone loss. Estrogen may downregulate the proinflammatory cytokines responsible for increased bone turnover while inducing OPG. 28,33 With the loss of estrogen at the menopausal transition, HIV-infected women become exposed to higher levels of bone-resorbing cytokines, leading to a more rapid, than expected, rate of bone loss postmenopause. 28,30 Given the evidence of increased susceptibility to fracture with decreasing bone density, the treatment of HIV-infected, middle-aged women should be geared towards fracture prevention. Early screening of this population may be prudent given the propensity for earlier menopause as well as perimenopausal bone loss. Treatment with the bisphosphonate alendronate was shown to be effective in treating HIV-associated bone loss without sex differences in response and may be a useful therapeutic option in HIV-infected perimenopausal women with low BMD who are at high risk for fracture. 34
Cardiovascular disease
Evidence suggests that HIV infection and antiretroviral therapy increase the risk for CVD beyond that of the traditional risk factors for the general population such as smoking, dyslipidaemia, hypertension, obesity and diabetes. 35 However, participants in most studies thus far addressing CVD and its associated metabolic derangements in HIV-infected individuals have largely consisted of men. Given the potential for interaction between HIV infection and CVD as well as between menopause and CVD, consideration of CVD risk in HIV-infected women facing menopause is warranted.
HIV infection has been associated with CVD outcomes as well as with metabolic and lipid alterations linked to CVD. 36–38 Similarly, therapy for HIV infection has been associated with both CVD outcomes and metabolic and lipid alterations linked to CVD, including metabolic syndrome and lipodystrophy. 36,39–41 Metabolic syndrome has several components: abdominal obesity, atherogenic dyslipidaemia, elevated blood pressure, insulin resistance with or without glucose intolerance, proinflammatory state and prothrombotic state. 42 Lipodystrophy syndrome has been described in HIV-infected patients as selective thinning of subcutaneous cheek and peripheral fat, often accompanied by visceral and dorsocervical fat accumulation, subcutaneous lipomata, dyslipidaemia insulin resistance, hyperglycaemia and diabetes. 41 HIV-associated lipodystrophy syndrome has been linked to protease inhibitor (PI) and nucleoside reverse transciptase inhibitor use, but has also been described in patients with no history of retroviral therapy. 41 Female sex and longer duration of HIV infection with greater immunosuppresion have been identified as risk factors for lipodystrophy. 41
Dolan et al. 43 studied CVD risk indices in 100 HIV-infected women alongside 75 healthy women similar in age and race. C-reactive protein, IL-6 and triglyceride concentrations were significantly higher in HIV-infected women while HDL and adiponectin were significantly lower. 43 Significantly more HIV-infected women than HIV-uninfected women showed either impaired glucose tolerance or fasting hyperinsulinaemia. 43 In addition, HIV-infected women had significantly higher waist-to-hip (WHR) ratio and visceral to subcutaneous fat area ratio but significantly lower total body fat, extremity fat, subcutaneous abdominal fat area and hip circumference. 43 WHR was found to be independently associated with coronary heart disease incidence in the Nurses' Health Study. 44
In the Women's Interagency HIV Study, HIV infection was independently associated with metabolic syndrome in a sample of 1725 HIV-infected and 668 HIV-uninfected women. 45 Higher mean triglyceride and lower mean HDL cholesterol levels were found in HIV-infected women compared with uninfected women. 45
Triant et al. 46 examined the incidence of acute myocardial infarction (MI) in a large cohort of HIV-infected and HIV-uninfected patients. 46 They found in HIV-infected patients significantly higher acute MI rates and proportions of hypertension, diabetes and dyslipidaemia. When analysis was stratified by gender, increased relative risk of acute MI was higher in women than in men, which the investigators suggest might be due to altered inflammatory marker profiles, changes in body composition, relative shift from gynoid to android fat distribution or greater rates of some traditional cardiac risk factors such as diabetes in women. 46 Overall, dyslipidaemia was the risk factor most significantly associated with acute MI. 46
In a cohort of Kaiser Permanente Northern California patients, increased risk of MI was observed with use of PI in HIV-infected patients compared with HIV-uninfected patients. 47 Moreover, increased relative risk of MI with HIV infection was even higher for HIV-infected women than in HIV-infected men. 47
Investigators of the SWAN study suggest an association between declining estrogen levels during the menopausal transition and alterations of the peripheral vasculature. 48 Estrogen can affect vasodilation and vasoconstriction through activating nitric oxide, decreasing endothelin levels and increasing adrenergic activity. 48 In a sample of 483 women, the menopause transition was associated with higher systolic and diastolic blood pressure, total LDL and HDL cholesterol, triglycerides, glucose, insulin, HOMA-estimated insulin resistance, free androgen index, testosterone, common carotid artery (CCA) adventitial diameter and CCA intima-media thickness levels. 48 Lower estradiol was associated with significantly larger adventitial diameters, even after adjustment for CVD risk factors. 48 Larger CCA diameter has been associated with CVD risk. 49 Separate analysis of haemostatic factors in women from the SWAN study led to the conclusion that endogenous estrogens might reduce CVD risk through suppression of fibrinolytic factors, but not by modulation of coagulation or inflammatory markers. 50 In addition, low levels of sex hormone-binding globulin and high levels of free testosterone have been associated with CVD risk in women. 51–53
Traditional CVD risk factors increase during menopause, including changes in body fat distribution, glucose intolerance, dyslipidaemia, hypertension, increased sympathetic tone, endothelial dysfunction and vascular inflammation. 10,54–56 HIV infection and antiretroviral therapy appear to compound the menopausal increase in many of these CVD risk factors and become the cause for additional and perhaps earlier concern.
Cognition
Cognitive declines associated with ageing are well-documented, but cognitive changes specifically associated with menopause are less clear. 57–64 Numerous plausible biological mechanisms for neuroprotective roles of estrogen exist. 65–67 However, evidence for benefit with hormone replacement therapy has been equivocal. 68 Alexander et al. 69 suggest that symptoms of the perimenopause such as sleep loss have the potential to affect cognition.
Ageing individuals infected with HIV may be at higher risk for developing age-related cognitive decline, mild cognitive impairment or dementia. 70 Chronic immune activation with HIV infection can lead to progressive hyperproduction of inflammatory cytokines within the nervous system and onset of HIV-associated dementia (HAD). 71 Risk factors for HAD include low CD4 count, anaemia, low BMI, age, systemic symptoms, injection drug use and female sex. 71 HAD incidence has been drastically reduced with the introduction of antiretroviral therapy. 70,71 Minor, chronic cognitive deficits that may affect a greater proportion of HIV-infected individuals require much more demanding and detailed neurological testing to detect and remain the source of much debate but little firm data. 72 Accurate cognitive testing may be especially difficult in HIV-infected individuals with low education levels.
In addition to HAART, Vance et al. 73 suggest reducing alcohol and substance use, improving nutrition, treating co-morbidities, increasing social contact, reducing depression and stress levels, engaging in cognitively stimulating activities, applying cognitive remediation therapies, and incorporating psychopharmacological interventions to improve neuroplasticity and cognitive reserve in HIV-infected individuals. Attention to psychiatric co-morbidity during menopause, including depression, is also critical. 69 Research on cognition in HIV-infected women would be strengthened by adoption of more uniform, sensitive testing.
Conclusions
Current literature on the nature of menopause in HIV-infected women leaves much room for further study. The emerging picture, however, suggests that menopause in HIV-infected women may in fact be exceptional. HIV infection might independently cause the earlier menopause, which would mean longer exposure to postmenopausal health risks. HIV-infected women also appear to complain of more menopausal symptoms. Reproductive hormones in HIV-infected women are associated with both HIV infection and drug use, leading to a need for caution in interpreting hormone levels when assessing menopausal status. In addition, HIV infection and menopause may have cumulative negative effects on BMD, CVD risk and/or outcome, and cognition. A variety of CVD outcomes have been associated with antiretroviral therapy. Nevertheless, it appears that overall CVD event outcomes are better with continuous rather than interrupted antiretroviral therapy. 74
Menopause in HIV-infected women may also be exceptional for its considerable interaction with lifestyle and demographic factors, which are overall different in HIV-infected women. HIV-infected women are more likely to smoke, use drugs, be less educated and experience greater life stress. Improved assessment of health risks as well as enhancement of directed systems of health-care delivery in this special population is needed. More and more, clinical care of HIV-infected, middle-aged women will be guided by a geriatric model and goals oriented toward the long-term. Health-care providers are needed with expertise in both ageing and HIV infection, as the effects of each may be difficult to disentangle. 75 For many topics discussed in this review, definitive research remains lacking. With further research, though, lies hope of healthier futures both during and after the menopause in HIV-infected women.
Competing interests
None declared.