
Abstract
Objective
To establish whether treatment for three years with pro-juven progesterone cream affects progression of atherosclerotic plaques or bone density in postmenopausal women.
Design
Randomized double-blind placebo-controlled trial.
Sample
One hundred and thirty-one healthy postmenopausal women aged between 50 and 75 years with at least one asymptomatic arterial plaque visible on ultrasound of the carotid or femoral bifurcation.
Methods
Women were randomly allocated to receive pro-juven progesterone cream, 20 mg twice daily, or placebo, for three years.
Main outcome measure
Rate of change of plaque thickness, intima-media thickness and bone density of lumbar spine and femoral neck.
Results
There was no difference between the groups.
Conclusion
Pro-juven progesterone cream 20 mg twice daily did not affect progression of asymptomatic atherosclerosis or deterioration in bone density over three years.
Introduction
Although conventional estrogen and progestogen hormone therapy is effective for the relief of menopausal symptoms and prevention of osteoporotic fractures, adverse effects such as vaginal bleeding and a perceived risk of breast cancer and cardiovascular disease have led to the need for alternatives. A potential alternative requested by patients is progesterone cream as it has been claimed that this will preserve bone density while being free from unwanted side-effects. 1–5
Evidence to suggest that progesterone or progestogens may conserve bone in postmenopausal women is limited. Progesterone receptors are expressed in human osteoblasts 6 and progesterone stimulates human osteoblast proliferation. 7 In rat cell culture, progesterone stimulates bone nodule formation in a dose-dependent fashion. 8 Oophorectomized rats treated with progesterone have no reduction in bone weight compared with sham-operated controls. 9
In postmenopausal women, the progestogen, gestronol, prevented bone loss over one year. 10 When 20 postmenopausal women were treated with norethisterone for two years, there was an increase in bone mineral content of 1.65% annually, which was compared with an overall loss of 5% over two years in a matched group taken from the placebo groups of earlier trials (P < 0.002). 11
There is evidence to suggest that progesterone is free from the negative cardiovascular effects of other progestogens and may even have a direct beneficial effect on the cardiovascular system and the genesis of atherosclerotic plaque. Progesterone inhibits the proliferation of vascular smooth muscle, an important constituent of plaque, 12,13 and induces relaxation of precontracted rabbit coronary arteries. 14 When oophorectomized rhesus monkeys were treated with either estrogen, progesterone or combined estrogen plus progesterone this protected against coronary vasospasm, whereas addition of medroxyprogesterone acetate had the opposite effect. 15,16 In the three-year prospective Postmenopausal Estrogen/Progestin Interventions Study, levels of high-density lipoprotein (HDL) cholesterol were significantly higher in women in whom conjugated equine estrogen was opposed by micronized oral progesterone than by medroxyprogesterone acetate. 17 In a small randomized-controlled cross-over study of hypertensive postmenopausal women and men, oral progesterone caused a dose-dependent reduction in blood pressure. 18
The use of progesterone cream for prevention of postmenopausal osteoporosis and cardiovascular disease has been questioned. 19,20 Pharmacokinetic studies indicate that progesterone creams give serum progesterone levels that are substantially lower than those found in the mid-luteal period. 21–24 In randomized-controlled trials, Wren 25 found no change in bone markers or lipids after 12 weeks and Leonetti 26 found no improvement in bone density after one year.
Methods
The aim of this study was to investigate whether progesterone cream reduces the progression of small asymptomatic atherosclerotic plaques or the deterioration of bone density, which occurs over three years in healthy postmenopausal women.
Participants
With the approval of the local ethics committee, healthy postmenopausal women aged 50–75 years were recruited from menopause clinics at the Chelsea and Westminster, and Lister Hospitals, and in response to articles in predominantly national newspapers. The articles would have interested postmenopausal women who were looking for alternatives to conventional hormone replacement therapy and such women were invited to take part in a prospective study of the effects of progesterone cream.
Subjects were screened by telephone interview, self-administered questionnaire and clinical assessment including history and examination. A pelvic ultrasound scan was performed to exclude asymptomatic ovarian or endometrial pathology and, if required, either a mammogram or cervical smear, or both, was arranged.
Menopause was diagnosed by being more than one year since the last menstrual period (if the uterus was present) or following bilateral oophorectomy. All had follicle-stimulating hormone (FSH) > 30 U/L. None of the participants had taken any other form of hormone therapy within the previous eight weeks, or had ever had a hormone implant.
Subjects had to be asymptomatic for cardiovascular disease and free from active thyroid disease or clinical suspicion of a disease likely to affect bone turnover. Concomitant use of medication likely to affect cardiovascular function or bone turnover or medication known to affect liver enzymes was not permitted. A stable dose of thyroxine was permitted.
Eligible subjects were invited for a vascular ultrasound scan to look for arterial plaque at the carotid and common femoral bifurcations on both sides. Those with at least one small plaque at one or more of these sites were offered a place in the study.
Assessments
If the screening assessment indicated eligibility for the study, a high definition ultrasound scan of the carotid and femoral arteries was performed to measure plaque thickness and intima-media thickness (IMT) using Advanced Technology Laboratories High Definition duplex 3000 system with a high-resolution broadband width linear array transducer L7-4 MHz. The coefficient of variation for the intraobserver variability was 5%.
Subjects were examined supine with a small pillow under the neck, and the head and neck was rotated 45° from the side where the scanning was being performed. Carotid and femoral artery bifurcations were visualized on both sides, initially by a transverse scan. The bifurcation was examined for plaques over a length of 4 cm (2.5 cm proximal and 1.5 cm distal to the flow divider). In the carotid, this included the distal common carotid artery, carotid bulb and proximal internal carotid artery. The femoral artery was similarly examined, such that the whole arterial wall was viewed, circumferentially, proximal and distal to the flow divider. The probe was then rotated through 90° to obtain and record, on both magneto-optical disc and video, a longitudinal image of both the anterior and posterior arterial walls.
The scan was performed first using the colour flow Doppler, which allowed any echolucent plaques to be visualized as filling defects. It was then repeated in B-mode and measurements were taken of the thickness of the intima media complex at its thickest point on the posterior wall of the common carotid and common femoral arteries, approximately 2 cm proximal to the flow divider. On optimal views, the measurements taken from longitudinal and transverse sections were identical. If a plaque was present at that spot, the IMT was measured adjacent to the plaque. IMT for a patient was taken as the mean of the maximum IMT measured across four vessels: the common carotid and common femoral arteries on both sides.
The thickness of any plaque was measured at its thickest point in both longitudinal and transverse section. Plaque was defined as a localized thickening of the intima-media complex measuring more than 1.2 mm at its thickest part. Most asymptomatic plaques were small, measuring less than 3 mm in thickness, and unlikely to be associated with cardiovascular events over the duration of the study. Occasionally plaque was of a size to cause constriction of 50% of the lumen or flow disturbances detectable with Doppler around the constriction. This is associated with increased risk of imminent stroke from embolization or occlusion and increased risk of significant plaque in the coronary arteries. Such patients were excluded from the study and referred to their general practitioner for further investigation. The approximate size, shape and location of each plaque were outlined on a diagram to facilitate return to the same spot for repeat measurements of plaque thickness at subsequent assessments.
Bone density of the left femoral neck and the lumbar spine from the first to the fourth vertebrae was measured using a Hologic QDR-1000 dual-energy X-ray absorptiometry scanner with version 5.11 software.
After an overnight fast, a sample of venous blood was taken for baseline assessment of serum progesterone, total cholesterol, HDL cholesterol and triglycerides. Samples for screening of FSH, oestradiol, full blood count, liver and thyroid function were also taken to confirm eligibility.
Subjects were randomly allocated to progesterone cream or placebo. The test drug studied was pro-juven, a 3% by weight progesterone cream delivering 20 mg progesterone per dose. Subjects were instructed to apply one measure of cream, twice daily, to a 100 cm2 templated area of the skin on the medial aspect of the forearm. Concomitant use of body creams and lotions was to be avoided since this had been associated with particularly poor absorption of progesterone in an earlier study. 21 To correct any dietary insufficiencies, all patients in the study were provided with a daily supplement of low-dose calcium magnesium carbonate.
Subjects were reviewed every six months. All pots were returned at the next assessment, including any unused cream. The pots were weighed and the weight of cream remaining was calculated. Adverse events that had occurred since the previous visit were recorded. A vascular ultrasound scan was performed to measure plaque thickness and IMT. Venous blood was taken for assessment of the parameters measured at screening. The measurement of bone density was repeated annually.
Sample size
We assumed a mean baseline plaque thickness of 1.30 mm with a standard deviation of 0.168 mm. A slow rise in plaque thickness, of about 0.03 mm over three years, was expected for untreated patients. 27,28 An 18% reduction in plaque thickness had been reported after six months in postmenopausal women treated with estrogen. 29 Using the nQueryAdvisor repeated-measures analysis of variance, it was determined that a sample size of 56 in each group would have 80% power to detect a difference in means of 0.09 mm, assuming a common standard deviation of 0.168 mm and using a two group test with a 0.05 two-sided significance level. To account for an anticipated drop-out rate of 15%, it was decided that 132 patients should be recruited into two equal sized groups.
Randomization and blinding
Identical pots were numbered consecutively and filled by the manufacturing laboratory with either pro-juven cream or placebo according to a predetermined computer-generated randomization schedule provided by Natural Medicine Company. One copy of the randomization code was held by the manufacturer and the other copy was held in a sealed envelope at the investigational site until the end of the clinical aspects of the study, at which time it was sent unopened to the statisticians. Eligible patients were assigned consecutive randomization numbers and were dispensed pots of cream bearing their unique randomization number.
Serum progesterone results were held at the laboratory until after the code was broken.
Statistical methodology
The primary outcome was the sum of plaque thickness measured in the common carotid and common femoral arteries on both sides. If there was more than one plaque in a vessel, the plaque thickness for that vessel was the sum of all the plaques measured in that vessel. If there was no plaque present, this was coded as zero. Every patient had a value recorded for all four vessels. Plaque thickness for the patient was then defined as the sum over the four vessels.
Secondary outcomes were mean maximum IMT and bone density. Like plaque thickness, IMT was measured in the right and left common carotid arteries and the right and left common femoral arteries. IMT for a patient was defined as the mean over the four vessels. Bone density of the lumbar spine and the neck of the femur were analysed separately.
The trial was analysed using a mixed model 30 with patient and patient–time effects fitted as random to take account of variation in response and in the timing and number of assessments between patients. Analyses were performed using the Statistical Analysis Systems version 6.12. Analyses were by intention to treat. All hypothesis testing was at the 5% level of significance and all tests were two sided. No interim analyses or subgroup analyses were performed.
Safety was assessed by means of effect on adverse events. An adverse event was defined as any illness, sign or symptom that appeared or worsened during the course of the clinical study regardless of whether it had a causal relationship to the treatment under investigation. For all adverse events the nature, duration and severity of the adverse event, as well as the action taken, if any, and the outcome, were recorded. All reported adverse events were coded according to MedDRA coding system. The incidence, severity, attributability and seriousness of adverse events were summarized by treatment group.
The effect on serum progesterone, total cholesterol, HDL cholesterol and triglycerides over three years was also monitored. Summaries of changes from baseline at six monthly intervals were calculated, by treatment group, together with 95% confidence intervals (CIs) for the mean change from baseline at each follow-up visit.
Results
The disposition of patients is shown in Figure 1. One hundred and thirty-one patients were randomly assigned to treatment, 65 to the progesterone cream group and 66 to the placebo group. All patients who were randomized did receive some study treatment, so summaries of serum progesterone and safety data were performed for this population. The intention-to-treat population comprised all patients from the safety population for whom at least one post-treatment efficacy assessment was available. Nine patients in the progesterone cream group and 10 patients in the placebo group did not have any post-treatment efficacy assessment. Thus, the intention-to-treat population comprised 112 patients, 56 in the progesterone cream group and 56 in the placebo group. Summaries and statistical analyses of the efficacy data were performed for this population.
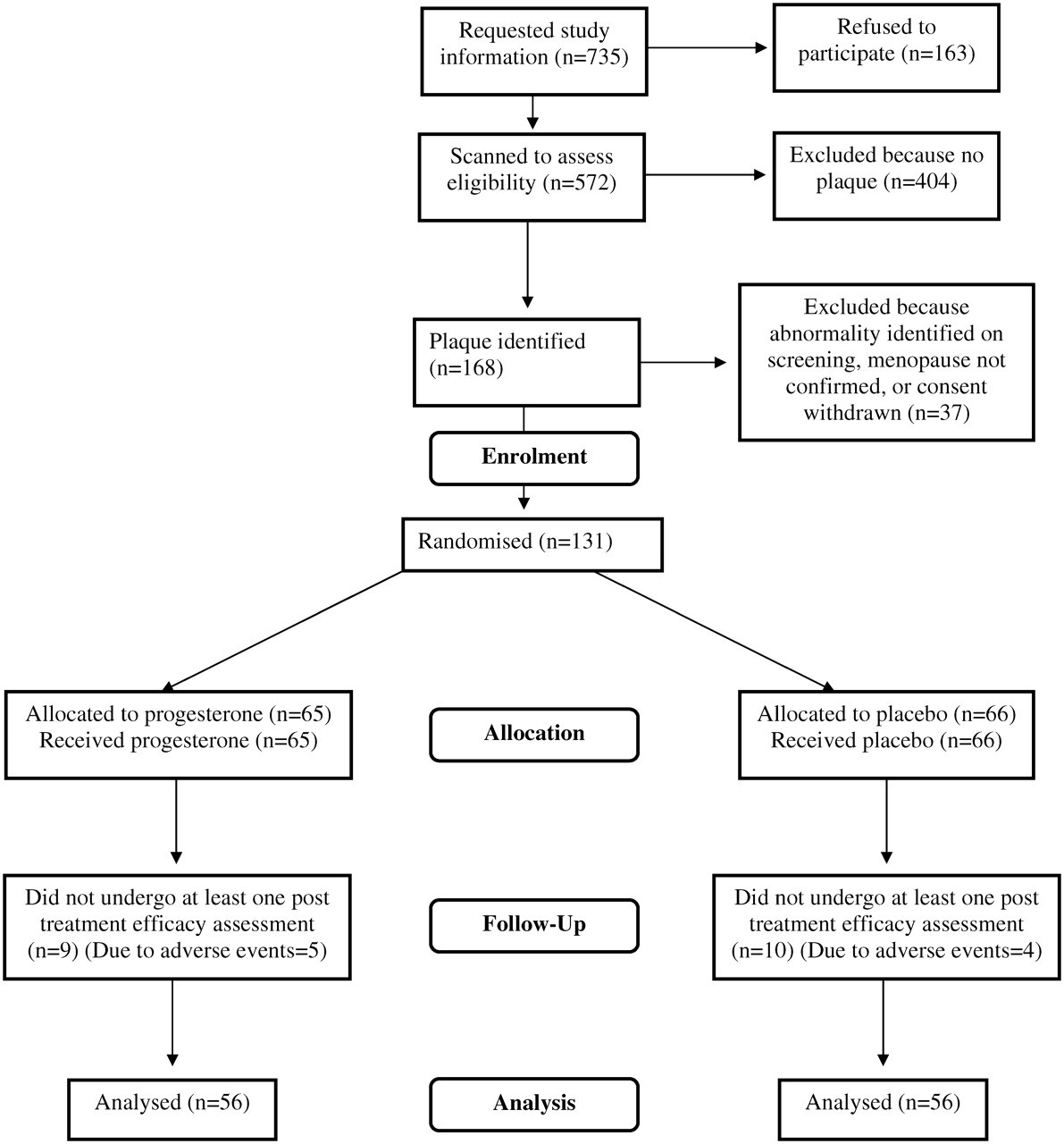
Consort flowchart
A further 25 patients withdrew prematurely from the progesterone group and from the placebo group there were 28. From the progesterone group, 15 were excluded for adverse events or the taking of medication prohibited by the protocol. Ten gave other reasons, mainly an inability to continue attending for follow-up. In the placebo group, the corresponding numbers were 19 and nine. Thus 31 patients in the progesterone group completed three years and in the placebo group there were 28.
Within the intention-to-treat group there were a further five patients (one in the progesterone group and four in the placebo group) who deviated from the protocol at some stage during the study.
Demographic and baseline data
Demographic characteristics of the intention-to-treat population are presented in Table 1 and baseline data in Table 2. The two treatment groups appear well balanced with respect to demographic variables, although plaque thickness, IMT and bone density at the spine and the hip were all higher in the progesterone group. The population was predominantly Caucasian and non-smoking. Most took regular exercise, a moderate alcohol intake and had tried hormone therapy in the past.
Demographic data
SD = standard deviation
Baseline data for efficacy parameters
Values are drawn from the intention-to-treat population and given as mean (standard deviation)
IMT = intima-media thickness
Efficacy analyses
Change from baseline in plaque thickness, IMT and bone density after three years is given in Table 3. The results of the random coefficients analysis are given in Table 4. There was no statistically significant difference in mean progression rate of plaque thickness, IMT or bone density at the lumbar spine or femoral neck between women randomized to progesterone and those randomized to placebo.
Change from baseline in efficacy parameters after three years
Values are given as mean (95% CI)
IMT = intima-media thickness
Rate of change of outcome measures for patients randomized to progesterone compared with those randomized to placebo
Analysis performed using random coefficients method. Values are given as mean (95% CI)
Serum progesterone
Values reported as <1 nmol/L were set to 1 nmol/L for the analyses. Mean serum progesterone was 1 nmol/L in both treatment groups before application of the cream. Mean change from baseline at six monthly intervals is shown, by treatment group, in Table 5. The greatest change from baseline occurred during the first six months. There was no accumulation thereafter. After 36 months, the mean (95% CI) serum progesterone for the group treated with progesterone was 3.54 (1.70–5.38) nmol/L.
Change from baseline in serum progesterone at six monthly intervals throughout the study
Values are given as mean change (95% CI)
Fourteen patients in the progesterone group and one patient in the placebo group returned serum progesterone levels in excess of 10 nmol/L. Contemporaneous hormone profile and pelvic scan results were reviewed for these patients. The 14 treated with progesterone cream all had FSH >50 U/L, oestradiol <200 pmol/L and a thin endometrium, consistent with menopause. The patient in the placebo group with a serum progesterone of 82 nmol/L at six months had an FSH of 17.7 U/L and an oestradiol of 218 pmol/L, and a pelvic ultrasound scan reported a functional ovarian cyst. This patient had failed to attend for assessment at 12 months. Serum was next sampled at the 18-month assessment when progesterone was once again 1.0 nmol/L, FSH 72.1 U/L and oestradiol 40 pmol/L. An isolated ovulatory episode is a likely explanation for the raised serum progesterone observed in this patient.
Lipids
In the progesterone group, the mean (95% CI) changes from baseline after three years in total cholesterol, triglycerides and HDL were 0.0 (−0.2, 0.2), 0.2 (0.1, 0.3) and −0.2 (−0.3, −0.1) mmol/L, respectively. Corresponding results for the placebo group were 0.4 (−0.1, 0.9), 0.3 (0.0, 0.6) and −0.1 (−0.2, 0.2). Thus there was a slight increase in triglycerides and decrease in HDL in the group treated with progesterone, although 95% CIs around the mean changes from baseline indicate that there is unlikely to be a statistically significant difference between the groups.
Adverse events
There were 11 serious adverse events over the course of the study. A 52-year-old patient with a history of Wertheim's hysterectomy and postoperative radiotherapy for stage IIb cervical cancer withdrew from the study two months after enrolment due to a recurrence of liver metastases. She died two months later. The laboratory holding the randomization code was contacted while the study was ongoing and it was revealed that she had been taking placebo. A 65-year-old patient was found to have microcalcification on a mammogram performed as a routine study investigation 17 months after enrolment. When the film was compared with an earlier mammogram performed nine months prior to enrolment, and at that time reported as normal, there were no appreciable changes. An ultrasound scan and fine-needle aspiration revealed malignant cells and she was excluded from the study and subsequently underwent wide local excision of grade two, vascular invasion negative tumour and axilliary node clearance. Her treatment group was not identified until after the study was complete when it was revealed that she had been taking placebo. A 66-year-old patient was diagnosed with colonic cancer 32 months after enrolment in the study. She underwent tumour resection and a course of chemotherapy. After the study was complete, it was revealed that she had been taking placebo. There were four additional serious adverse events in patients who were subsequently found to have been taking placebo: a hernia operation, a back operation, a hip replacement and a hospital admission for treatment of cellulitis secondary to longstanding lymphoedema of the left leg. All made full recoveries.
The following four serious adverse events occurred in patients subsequently found to have been taking progesterone: excision of breast scar tissue, laser excision of basal cell carcinoma, vaginal hysterectomy for prolapse and bunion surgery.
Adverse events occurred at broadly similar rates in the active and placebo groups. Sixty-six percent of patients in the progesterone group complained of adverse events compared with 61% in the placebo group. The majority of events were considered unrelated to the study drug. Twenty of the 34 patients (59%) who withdrew from the progesterone group gave adverse events as a reason. Twenty-three of the 38 patients (61%) who withdrew from the placebo group gave adverse events as a reason.
Discussion
Mean serum progesterone for the group treated with pro-juven was 3.54 (95% CI 1.70–5.38) nmol/L after three years. This is consistent with reports from studies of other formulations of progesterone cream used for short durations, either with or without concomitant estrogen. 21–24,31–33
The effect of progesterone cream on progression of asymptomatic atherosclerosis was evaluated. Unadjusted results gave a mean (95% CI) increase in plaque thickness over the course of three years of 0.93 mm (0.3–1.6) in patients randomized to progesterone. The corresponding increase in the placebo group was 0.94 mm (0.2 to 1.7). The annual progression rate was therefore 0.3 mm per year in both groups. For IMT the mean (95% CI) increase was 0.03 mm (−0.1 to 0.2) in the progesterone group and 0.11 mm (0.0 to 0.3) in the placebo group, which works out as an annual progression rate of 0.01 mm per year for progesterone and 0.04 mm per year for placebo. Using a random coefficients model, there was no statistically significant difference between the groups in the rate of progression of IMT.
The rate of progression of plaque thickness and IMT is in line with reports from other studies of postmenopausal women. 34–37
A secondary endpoint evaluated in this study was bone mineral density. In both treatment groups, there was no change in bone density of the neck of the femur and a slight fall in bone density of the lumbar spine over the course of the study. There was no significant difference between the treatment groups in change in bone density of either the lumbar spine or the neck of the femur over the course of the study. The fall in bone density of the lumbar spine was more pronounced in the placebo group, but this was of no clinical significance. The percentage fall in bone density of the lumbar spine in the progesterone group was 2.2% over three years. In the placebo group it fell by 2.5%.
No other study has examined the effect of progesterone cream on bone density over three years. Our findings are consistent with those of two other studies that have measured the effect of transdermal progesterone on bone. Wren 25 found no significant difference between progesterone and placebo in the change from baseline in markers of bone metabolism after 12 weeks. Leonetti 26 measured bone density at the spine, the neck of the femur and total hip after one year. There was a slight fall in bone density in both treatment groups. There was a statistically significant difference between the groups with respect to the femoral neck, bone density being higher in the placebo group, but this difference had been present before treatment. There was no statistically significant difference between the groups at the end of one year in terms of the other bone density parameters. The percentage of individuals in each group showing a greater than 1.2% increase in bone density over the course of the study was also calculated for each parameter and there was no difference between the groups.
In our study, adverse events occurred at broadly similar rates in progesterone and placebo groups. Overlapping 95% CIs indicated that there was unlikely to be a statistically significant difference between the groups in change from baseline over three years for total cholesterol, HDL cholesterol and triglycerides. This finding was consistent with that of Wren, who found no difference between pro-feme progesterone cream and placebo in effect on change from baseline in blood lipids after three months. 25
Conclusion
Pro-juven progesterone cream 20 mg twice daily did not affect the progression of arterial plaque, IMT or bone density over three years in healthy postmenopausal women.
Footnotes
Acknowledgements
We are grateful to Ms Cynthia Haliburn from Hartington's Statistics and Data Management for data management and statistical analysis. The trial was funded by Natural Medicine Company.