
Abstract
The time is ripe for universal understanding and acceptance of outcome assessment in venous disease. Outcome studies promote understanding of the diseases we treat and the results of treatment. The choice of a valid and reliable assessment tool is crucial. Patient-generated quality-of-life tools include generic instruments and disease-specific instruments. Generic instruments evaluate overall well-being and provide subjective measurements of treatment outcomes in various disease states. The 36-Item Short Form Health Survey and the Nottingham Health Profile are widely used generic surveys. Disease-specific instruments relate to a particular disease state. They are popular in venous disease reporting and have high sensitivity. The Chronic Venous Insufficiency Questionnaire, the Venous Insufficiency Epidemiological and Economic Study, the Aberdeen Varicose Vein Questionnaire and the Charing Cross Venous Ulceration Questionnaire are such devices. Physician-generated measurement tools are used to evaluate and classify the consequences of venous disease. The clinical, aetiology, anatomy, pathophysiology classification (CEAP) is a popular descriptive platform for chronic venous disease. The Venous Severity Scoring (VSS) system was derived from the CEAP classification to provide evaluative capabilities. The three elements of the VSS are the venous disability score, the venous segmental disease score and the venous clinical severity score (VCSS). The VCSS facilitates the follow-up of features of venous disease that change with treatment. Each of these outcomes tools has been validated, and each has strengths and weaknesses. Maintaining the dynamic nature of assessment with periodic review and revision is the way forward to generating universal applicability. Although the choice of instrument is debatable, the most important factor in improving treatment outcomes is the decision to examine results and to share them in a meaningful way.
It is not the strongest of the species that survives, nor the most intelligent, but the one most responsive to change. Charles Darwin
Outcome assessment is a term that dominates the global landscape of vascular interventions. Outcome reporting has become a catchphrase for determination of the acceptable standard. Its tools allow us to stratify disease and therapy. The way in which outcomes are reported allows results to be compared. In his 1996 presidential address to the Society of Vascular Surgery, Rutherford states: ‘The results of therapy for vascular diseases have little meaning if presented in isolation, no matter how uniform and valid the criteria used for reporting them. They are intended to be compared with something’. 1 For vascular specialists who strive to find something better for their patients and who are willing to change based on what they find, outcomes must be analysed and presented in such a way as to be shared and compared. 2
Outcome reports of therapy for venous disease are common in medical literature. With recent research into venous stasis ulcer therapies, 3 the role of medical compression stockings in chronic venous disease, 4 venous outflow stenting 5 and endovenous ablation, 6 the opportunity for compilation, analysis and reporting of outcomes is abundant. With this amount of clinical, scientific and third-party attention being paid to outcomes, clinicians treating venous disease need to assess their position on these issues. There is a groundswell of renewed interest in the academic and private realms of the international community. The following two simple questions can elicit your opinion: (1) Do you believe that it is important to follow clinical outcomes in venous disease? Yes or no; (2) What do you believe is the predominant reason why you are currently not following your outcomes more closely? (a) Do not care; (b) too cumbersome or time-consuming; (c) do not see the value; (d) have not figured out the available tools; or (e) no uniformly accepted standard.
Where do you stand? Mark your answers in the margin so that you can revisit them after you have finished reading this article. We believe that you will consider things differently after seeing them through our lens. We will provide you with a thorough discussion of the most commonly used reporting instruments and their applications to your venous practice. We will discuss the opportunity to arrive at a universally accepted standard. We invite your critical thought.
Definition of an outcome and assessment of its efficacy require an understanding of the disease process and a therapeutic goal that can be objectively measured. Padberg has studied outcome reporting extensively and in a recent article states that ‘everyone will benefit from an integrated assessment of symptoms, clinical findings, non-invasive examinations and functional outcomes to better define the role of surgical, physical and medical therapies for chronic venous disease’. 7
The goal of treatment in venous disease is primarily palliative and varies among physicians and their patients across the spectrum of conditions. To measure and report only the clinical outcome of therapy through morbidity and mortality statistics omits many collateral effects and potentially serious implications. To fully assess an outcome, the effects on the physician, the patient and the community should be reported. 8 This notion is at the heart of quality of care that considers quality of life (QoL). The value of the patient's perspective in assessing the outcome of therapy has recently come to the forefront of consideration. 9
Furthermore, differentiation between clinically important outcomes and ‘surrogate’ outcomes needs to be made. A clinically important outcome is that which improves a patient's symptoms, QoL or survival. A surrogate outcome implies connectedness to what is important to the patient, but in reality may contribute little to the patient's health and even less to clinically relevant evidence. It is in fact a replacement outcome and should be used with care. For example, in superficial endovenous treatments, an often-used study measurement includes vein ablation. Although this may be important in a catheter feasibility study, ultrasonographically proven vein ablation does not necessarily correlate with the patient's symptoms, QoL or clinical severity score. In his not yet published 2008 presidential address to the American Venous Forum, Meissner states: ‘Unfortunately, surrogate outcome measures are often based on an unproven, assumed relationship between the surrogate marker and an accepted clinical outcome. (…)we are now at a point in the evolution of these procedures where we should move beyond case series and surrogate outcome measures to investigation of long-term clinically important outcomes’. 10
Methods for reporting clinical outcomes in vascular surgery have been in existence for years. There has been more recent emphasis on physician-generated assessment tools that can be used longitudinally to track clinically defined endpoints and changes seen during treatment. In a chapter on assessment and reporting of outcomes in Rutherford's Vascular Surgery, White et al. 11 discussed the following requirements for a therapeutic assessment tool: an understanding of the course of the disease as seen by patient and physician, the overall effect of the disease on the patient's usual state of being, and coverage of all aspects of treatment, including risks and benefits to the patient.
There are basically two ways to follow outcomes in venous disease. We can use a patient-perceived quality-of-life measurement, or we (the physician) can evaluate and report clinical signs. There are many definitions of QoL and as many ways to measure it. Nevertheless, key concepts include attention to the patient's perspective, a realistic appraisal of the disease's functional effect on daily life, and a consideration of physical, social and psychological strata. 12 The World Health Organization issued a summary statement in 2002 that in part defined QoL as ‘a multidimensional construct relating to symptoms, impairments, functional status, emotional states and health domains’. 13
For a quality-of-life instrument to be a valuable measure of what is intended, it must be reliable and valid. For it to gain popularity among researchers and clinicians, it must also be practical. 12 Reliability evaluates the consistency of provided answers across the spectrum of patients using it. Patients with similar conditions should answer questions in a similar way. Validity evaluates the ability of a question to measure the object variable and examines the consistency of responses to questions over time. 11 Practicality is a function of the study at hand and the information that can reasonably be expected to be collected by study personnel to provide the necessary data.
There are two basic categories of quality-of-life surveys, generic and disease-specific. Generic instruments usually assess global states of well-being, provide a subjective measure of treatment efficacy, and as a result are appropriate for use across a wide spectrum of disease states. They have high comparative value for unrelated diseases and are generalizable between studies. 12 This helps establish the relative priority of a procedure, especially when determining cost-effectiveness in this era of limited resources.
Generic instruments
The 36-Item Short Form Health Survey
A widely-used and well-validated generic quality-of-life instrument is the 36-Item Short Form Health Survey (SF-36). The SF-36 has been developed over time with questions in the following two categories: physical health (assessed as the patient's level of functioning) and mental health (assessed as an indication of well-being). These two groups have been broken down into eight domains that include evaluation of physical and social functioning, role limitations due to physical or emotional problems, mental health, pain, vitality and health perception. When complete, the survey generates a score ranging from 0 to 100, with higher scores indicating better general health perception. 12 The SF-36 has proven to be a good fit for generic quality-of-life assessment in the population with chronic venous disease.
Kaplan et al. 14 studied 2404 patients for the presence of venous disease and application of the SF-36, finding that ‘even modest venous disease translates into functional limitations and limitations in daily activities. Venous disease does not appear to affect emotional aspects of health related quality of life’. Another large epidemiological study using the SF-36 is the Bonn Vein Study. This population survey was undertaken in Germany with 3072 participants and was designed to determine the rate of occurrence and severity of chronic venous disease among the general public. 15,16 A study evolving from the Bonn Vein Study was an investigation by Pannier et al. 4 on the use of medical compression stocking in the Bonn Vein Study population, including the reasons they were prescribed and the patients' acceptance of them in the short and long terms. The SF-36 performed well in these studies because of the specific objectives. All three studies enrolled patients from the community without prior knowledge of their venous disease status. By using the reliability and validity of the SF-36 along with physical examinations, it was possible to determine the rate of occurrence of chronic venous disease and its effect on several quality-of-life parameters.
The International Quality of Life Assessment Project aims to translate and adapt the SF-36 into all major languages. If this undertaking is successful, the SF-36 will gain strength internationally as a measure of health-related QoL. 3
Nottingham Health Profile
Another generic instrument, the Nottingham Health Profile (NHP), was devised to be applied in many conditions. It was designed as a short assessment of emotional, social and physical health problems from the patient's perspective across a wide spectrum of disease states and severity. 3 In a 2003 study, Wann-Hansson et al. 17 compared the SF-36 with the NHP in patients with varying degrees of chronic limb ischaemia. Ninety patients were evaluated with each survey following revascularization using percutaneous transluminal angioplasty or surgery for lower extremity disease ranging from claudication to severe ischaemia. The investigations showed validity in the postoperative period, with good correlation of information. Although the SF-36 demonstrated more internal consistency among patients with claudication and milder ischaemic symptoms, the NHP had greater sensitivity to change among patients with more severe ischaemia. 17
Disease-specific instruments
Disease-specific surveys focus on elements associated with particular disease processes and treatment effects. This increases the sensitivity to trends and outcomes of the condition being studied. 12 The survey questions are geared towards expected trends in the study of a particular disease and are more focused in their scope than generic instruments. They have become much more popular in venous disease reporting.
To learn more about quality-of-life issues directly related to chronic venous disease and its treatment, the use of a disease-specific measurement along with a generic instrument is advocated. 18 There is an important relationship here that needs to be better understood. Four instruments specific to venous disease have been used and validated to a degree during the past several years. Two of these, the Chronic Venous Insufficiency Questionnaire (CIVIQ) and the Venous Insufficiency Epidemiological and Economic Study (VEINES), consider venous disease as a whole, while two others, the Aberdeen Varicose Vein Questionnaire (AVVQ) and the Charing Cross Venous Ulceration Questionnaire (CXVUQ), address particular facets of venous disease.
Chronic Venous Insufficiency Questionnaire
The first version of the CIVIQ instrument, the CIVIQ 1, was validated in a sample of 2001 patients, 50% of whom had been diagnosed as having venous insufficiency, while the remainder had seen a general practitioner for other reasons. The following four areas of suspected quality-of-life effects were studied: physical, psychological, social and pain. Different numbers of questions were asked in each category, rendering generation of a representative composite score difficult. A revised version of the instrument, the CIVIQ 2, equally weighed the categories across 20 questions to provide a global score. 8 Both versions of the CIVIQ have been used in studies 5,8,19 and proven to be valid quality-of-life measurements.
A study by Launois et al. 8 initially developed the CIVIQ questionnaire through pilot testing and then validated the instrument in a clinical trial of 934 patients and an epidemiological survey of 26,681 patients. The results of these trials indicate that the CIVIQ is valuable in the assessment of chronic venous insufficiency (CVI). 8
Neglén et al. 5 used the CIVIQ along with the clinical, aetiology, anatomy, pathophysiology (CEAP) classification in an eight-year study on venous outflow stenting in 870 patients. QoL was evaluated before and after the intervention using the CIVIQ to measure pain, sleep disturbance, morale, social involvement, and routine and strenuous physical activities. Patients completed the questionnaire before surgery and again at each follow-up visit. An adverse effect on QoL due to chronic venous disease was observed, but patients noted significant quality-of-life improvement following the intervention. The CIVIQ was chosen in this study because of its validated relevance in chronic venous disease. 5
Perrin 19 applied the CIVIQ questionnaire to 3948 patients with lower extremity symptoms. The questionnaire was administered at regular intervals throughout the study to assess relevant symptoms and to identify factors contributing to quality-of-life improvement. Pain and heaviness had the greatest effect on patient-reported QoL, and a trial of Daflon relieved symptoms and led to improvement in quality-of-life scores. 19
Venous Insufficiency Epidemiological and Economic Study
The VEINES instrument consists of 35 items in two categories to generate two summary scores. The VEINES quality-of-life questionnaire (VEINES-QOL) comprises 25 items that estimate the effect of disease on QoL, and the VEINES symptom questionnaire (VEINES-Sym) has 10 items that measures symptoms. The focus of this instrument is on physical symptoms as opposed to psychological and social aspects. This, coupled with the division of summary scores into symptoms and disease effect, makes the VEINES instrument applicable on a range of clinical arenas. The evaluation of the condition as opposed to its treatment renders the VEINES useful in comparing studies that use different therapies for cardiovascular disease (CVD). 20 The VEINES has been validated in four languages. Responses are made on a two- to seven-point scale that rates intensity, frequency and agreement. Higher scores are associated with better QoL. 12
In a 2006 assessment by Kahn et al. 20 of the validity of the VEINES instrument regarding QoL in deep vein thrombosis (DVT), 359 patients with acute DVT were surveyed at regular intervals during their therapy. Results from the VEINES questionnaires were compared with similar categories on the SF-36 for assessment of instrument validity. The VEINES-QOL/Sym questionnaire was found to be acceptable, reliable, valid and responsive for use as a patient outcome measure in DVT. 20
Two additional studies used the VEINES with the SF-36 to provide generic and disease-specific quality-of-life profiles in venous disease. A 2004 study by Kahn et al. 21 compared the VEINES and the SF-36 with the CEAP classification in 1531 patients from four countries to examine the effect of patient-related quality-of-life reporting on interpreting outcomes in venous studies. After completing the VEINES-QOL and SF-36 questionnaires, patients were examined and scored by a physician based on the clinical category of the CEAP classification. Correlations between the CEAP classification, VEINES-QOL and SF-36 were examined. Higher CEAP class was directly associated with and predictive of the VEINES-QOL – assessed disease-specific quality-of-life measurement but not the generic SF-36. According to Kahn: ‘This provides further evidence of the validity of the VEINES-QOL and VEINES-Sym and the specificity of CEAP classification in terms of detecting morbidity directly attributable to chronic venous disease and not to other co-morbid conditions or patient characteristics’. 21
A 2001 study by Kurz et al. 22 used the SF-36 and the VEINES-QOL/Sym to assess the direct effect of varicose veins on patients' QoL. A cohort of 1313 patients with varying degrees of varicose veins and co-morbid conditions as evaluated using the CEAP score were studied. The population included a group of reference patients without varicose veins. Quality-of-life surveys were administered before the initial clinical visit. Patients were evaluated for the presence of varicose veins and any co-morbid conditions according to the CEAP classification. Findings showed that ‘impairment in physical QoL (in patients with varicose veins) is associated with concomitant disease, rather than the presence of varicose veins per se. This is particularly apparent when the concomitant disease is a healed or active ulcer. In patients with varicose veins, the objectives of cosmetic improvement and improvement of QoL (including relief of symptoms) should be considered separately’. 22 In terms of the degree of quality-of-life impairment assigned to varicose veins, the change in the VEINES and SF-36 results observed in patients categorized as CEAP 0 or 1 was equal to that observed for patients with isolated varicosities. 22
Lamping et al. 23 tested the VEINES instrument in a 2003 international study for use in the spectrum of venous diseases, including telangiectasias, varicose veins, oedema, skin changes and leg ulcers. Numerous study populations were used for field testing, test–retest and responsiveness, including 1531 patients from the original VEINES study population and 1516 in the responsiveness group. The survey was administered along with a clinical assessment at baseline, at three to six months and at 12 months to provide correlations between the outcome of treatment and the patient's quality-of-life perspective. Because patients were undergoing different therapies for different types of venous diseases, the questionnaire was the only common denominator in the evaluation. The validity of the instrument across the study population allowed ‘evaluation of the comparative impact of different clinical manifestations of chronic venous disorders of the leg, such as ulcers and varicose veins, on QoL and symptoms in the same study or across studies’. 23
A 2003 commentary by Padberg 7 on the article by Lamping et al. 23 focused on psychometric review of the VEINES questionnaire in determination of the underlying factors and the range of outcomes noted in chronic venous diseases. His main concerns with the VEINES project were two-fold. First, the use of diagnostic elements excluded classification of anatomical and physiological parameters that might aid in the choice of treatment. Secondly, he questioned whether the VEINES outcome scores were able to be scaled and had been presented in such a way so as to delineate clinical significance and degree of change over time. 7
Aberdeen Varicose Vein Questionnaire
The AVVQ is a 13-question survey addressing all elements of varicose vein disease. Physical symptoms and social issues, including pain, ankle oedema, ulcers, compression therapy use and the effect of varicose veins on daily activities, are examined in addition to the effect of varicose veins from a cosmesis standpoint. The questionnaire is scored from 0 (indicating no effect on the patient from varicose veins) to 100 (indicating severe effect). 12
In their 1993 article detailing the development of the AVVQ questionnaire, Garratt et al. 24 evaluated 373 patients seeking treatment for varicose veins along with 900 persons from the community. The AVVQ was sent with an SF-36 questionnaire to all participants. After scoring, a high correlation was found between the AVVQ and the SF-36 for referred patients and for community members, with the perceived health in the patients with varicose veins lower than that in the general population. The impetus for the development of a questionnaire specifically addressing the effect of varicose veins on QoL was to establish an instrument to measure outcome variables and treatment effects in varicose vein disease. According to Garratt et al. ‘varicose veins are often considered a relatively unimportant condition… This study showed that there are significant differences in health between patients with varicose veins and the general population… Because of its restricted focus, however, our clinically based questionnaire may be more sensitive in showing change over time and in discriminating between patients with mild symptoms. Thus it may be more useful in managing individual patients’. 24
Smith et al. 25 evaluated the AVVQ in a 1999 study of patients with varicose veins undergoing surgical therapy. A total of 137 patients completed the SF-36 and the AVVQ before undergoing saphenous stripping with phlebectomy and at six weeks after the procedure. Compared with a sample from the general public, patients with varicose veins demonstrated lower overall QoL on both questionnaires at the preoperative survey. At six weeks after the procedure, scores on both instruments had increased, and similar questions on both surveys indicated a high degree of agreement between the SF-36 and the AVVQ. Most notably, health transition scores showed a significant increase, indicating improvement in health status following surgery. 25
In a 2006 study comparing endovenous laser therapy (EVLT) with stripping and ligation, Mekako et al. 6 used the SF-36, the AVVQ, and Venous Clinical Severity Scoring (VCSS) to assess QoL at specific intervals following an intervention. Seventy patients underwent EVLT, and 62 patients underwent high saphenous vein ligation, stripping to the knee and microphlebectomy as indicated. The primary study outcome was quality-of-life measurement and change. All patients were administered the SF-36, AVVQ, and VCSS instruments before the procedure and at one, six, and 12 weeks afterward. Although both groups experienced improvement in QoL by the 12th post-therapy week, there was a significant difference between the groups early after treatment. The surgery group reported an initial decline in quality-of-life parameters on the AVVQ and in the physical domains of the SF-36. By the 12th week, QoL was improved for both groups, but the EVLT group had greater AVVQ improvement. This finding may have been a result of the specificity of the AVVQ for varicose vein–related QoL or perhaps due to baseline differences between the two groups. The VCSS values also were improved for both groups by the 12th week. 6
Charing Cross Venous Ulceration Questionnaire
The CXVUQ was developed to provide a valid quality-of-life measure for patients with venous ulcers. Although it can be intuitively assessed that venous stasis ulcers negatively affect patient-perceived QoL, there was no reliable instrument in place to evaluate the effects of the various treatments available for venous ulcers before the development of this questionnaire. Smith et al. 26 developed an ulcer-specific questionnaire from several sources and used it in conjunction with the SF-36 to validate the instrument for use in patients with venous ulcers. The new questionnaire and the SF-36 were tested among a cohort of 98 patients meeting criteria for ulcer size and duration. The questionnaire showed correlation with the eight domains of the SF-36, and the responses to questions on the instrument being tested matched well with those of specific questions on the SF-36. This disease-specific questionnaire provides a consistent measure of patient-reported QoL in venous ulcers regardless of the treatment option selected. Combining it with a generic measure such as the SF-36 may provide valuable information on the progression of ulcers and on the treatment measures chosen. 26
Howard and Davies 9 undertook a review of health-related quality-of-life assessments pertaining to venous ulcers. They examined several specific and generic instruments for their measurement properties, including the context in which they are to be used, the cultural variations that need to be addressed with translation and their consistency in administration. In consideration of the application of a health-related quality-of-life instrument, areas that might benefit most from evaluation were determined. These included the usefulness of a treatment method, results reporting in research studies, analysis of the cost to benefit ratio in treatment, establishment of treatment guidelines and public health policy, evaluation of symptoms that may be difficult to assess objectively, and extension of care and treatment to a wider community. They concluded that combining traditional clinical outcome measures, a generic instrument such as the SF-36 and a specific quality-of-life measurement may generate a more complete outcome assessment in patients with venous stasis ulcers. 9
In a 2007 chapter by Meissner et al. 27 on venous disease, they recommend that outcome assessment in vein disorders be based on pretreatment and post-treatment status using an objective measurement instrument to avoid observer variability. Patient-reported quality-of-life assessments are seen as a valuable adjunct to clinical observations and to physician-generated assessment tools. The four specific assessment tools (the CIVIQ, VEINES, AVVQ and CXVUQ) are noted to be generally acceptable but are inapplicable to the wider spectrum of venous disease. The CIVIQ is thought to be consistent and stable, but insufficiently thorough in its emphasis to address more severe venous disease and insufficiently specific in its determination of endpoints. The VEINES is noted to have been extensively studied and validated within a select research group. It is considered to be in need of additional study outside the original research and patient groups. The AVVQ and the CXVUQ have been well validated in wide use, but both primarily address specific elements of venous disease and not the entire spectrum of issues surrounding disease course and treatment. Meissner et al. 27 recommend that definitive action be taken to find the best combination of attributes in a questionnaire that will allow the most insight into quality-of-life issues across the spectrum of venous disease.
Guex et al. 28 designed a survey to address this gap in quality-of-life instruments and to be used in clinical practice. Their Specific Quality of Life and Outcome Response–Venous survey considers the primary complaint of the patient and the relevance to venous disease. They refer to this as a ‘patient-reported outcome’ in that it is a completely patient-driven ‘autoquestionnaire’ designed following a review of the existing questionnaires. This tool is unique in its consideration of symptoms, impairment of activities, appearance of the legs and health-risk concerns. Consideration is given to account more completely for the main concerns of patients, including those in the CEAP C0 to C3 categories. Validated in a test (n = 202) and retest (n = 152) of a European patient cohort, the survey is undergoing English-language validation and additional studies to determine its ability to assess the effect of treatment across the spectrum of venous disease.
Patient-related quality-of-life surveys are not without inherent problems. The amount of time required for patients to complete them can be significant, and the study results can be cumbersome to follow-up and to analyse in daily practice applications. The reliability of the responses may vary because of time elapsed since the onset of symptoms. In some surveys, the replies may be overly subjective relative to objective outcome. The sheer number of surveys and the design and specificity of each can prove confounding to researchers trying to select a survey best suited for the problem at hand.
Physician-generated measurement tools
Although patient-reported quality-of-life surveys have become important elements in the evaluation of disease states and the effect of therapy, another level of outcome assessment needs now to be considered, namely, the physician-generated measurement tool. Several of these tools are in use to evaluate and classify the condition, treatment and consequences of venous disease.
CEAP classification
The CEAP classification was developed as a common descriptive platform for the reporting of diagnostic information in chronic venous disease. Eklöf et al. 29 reported that the CEAP classification was also designed as a tool for regular patient documentation and management. The clinical component is scored from 0 to 6 and indicates increasing disease severity, ranging from none (0 points) to active ulcers (6 points). The aetiological component is used to denote whether the venous disease is congenital, primary or secondary in nature. The anatomical classification pinpoints the veins involved as superficial, deep or perforating. The pathophysiological classification identifies the presence or absence of reflux in the superficial, communicating, or deep systems, as well as the existence of outflow obstruction. 30 The primary drawback in using the CEAP classification as a stand-alone physician-generated disease assessment is the responsiveness of the instrument. This is especially true for clinical C4 and C5 disease. The static nature of these measurements makes it difficult for a physician to track changes over time in response to therapy. 31
Early studies 21,32,33 using the CEAP classification noted a relationship between trends in the CEAP scores and other outcome assessments, including physician- and patient-centred instruments. In a study among patients with deep venous reflux, Gillett et al. 32 noted that ‘a significant increase in the Venous Clinical Severity Score (VCSS) and Venous Segmental Disease Score (VSDS) paralleled CEAP clinical class’. 32 Kahn et al. 21 in a study relating clinical classification of venous disease with patient-related QoL found that ‘clinically assessed CEAP class was significantly associated with generic and venous disease-specific QoL’. 21 Ricci et al. 33 noted that the ‘CEAP classification and VCSS had equally high negative predictive values’. 33 To increase sensitivity to changes during the course of therapy and to encourage wider use as a clinical assessment instrument, the CEAP classification underwent a revision in 2004. The framework of the CEAP system was maintained, but several categories were refined and expanded to enhance the dynamic response to therapy. 34 These included a change in the C classification to divide the C4 class into ‘a’ and ‘b’ categories that predict the risk of ulceration based on the type of skin changes observed, as well as revision of the E, A and P classifications to include the use of the descriptor ‘n’ to indicate no venous abnormality. In addition, a basic CEAP system was introduced using the highest descriptive element for clinical classification. This rendered the clinical CEAP system more attractive to the clinician for regular use. An advanced CEAP classification, including all parameters, was made available for research and for standardized reporting. 29
In 2007, Chiesa et al. 35 recruited volunteers from the general population via media advertisements for the evaluation of chronic venous disorders. After enrolment, 16,251 participants were identified. These subjects underwent clinical examination by a physician, CEAP scoring and ultrasonographic evaluation. After workup, a correlation was noted between the signs of disease based on the CEAP classification and the ultrasonographic findings of reflux. The relationship between patient-reported symptoms and venous disease varied between men and women. 35
More recently, the CEAP system was used to classify venous disease in patients seeking evaluation at the American Venous Forum's National Pilot Screening Programme. McLafferty et al. 36 reported on the first annual event, held in 2005 at 17 centres across the country. Screening examinations were provided for 476 people from local communities who sought evaluation of their risk for venous thromboembolism. Along with a patient questionnaire and an abbreviated Doppler study, patients had their legs inspected and scored using the CEAP classification by a trained vascular professional. Following this, they had an exit interview with a physician to review their risk factors. Findings of reflux in the screening duplex examination correlated with CEAP scores. This demonstrated the value of combining Doppler measurements with the CEAP scoring system in screening for venous disease and risk assessment for venous thromboembolism. 36
Venous Severity Scoring
Although the CEAP classification has proven to be a useful descriptive instrument in classifying venous conditions, more information is needed regarding disease severity and longitudinal changes in patient conditions during treatment. 27 In response to this need for a disease severity measurement, the American Venous Forum in 2000 derived the Venous Severity Scoring (VSS) system from elements of the CEAP classification. 37 The VSS system is first and foremost an evaluative instrument. It was designed not to replace the CEAP system, but to supplement it and to provide a method for serial assessment. It has been proven to weather intraobserver and interobserver variability. 38 The basic components of the system are easy to learn and to apply. The features of the VSS are critically needed for longitudinal follow-up of a patient's clinical condition during and following an intervention. 2 There are three components of this new scoring system.
Venous Disability Score
First, the Venous Disability Score (VDS), which is basically an extension of the CEAP classification, evaluates the effect of venous disease via the level of work-based disability. The VDS is scored on a scale of 0–3 and is based on the ability to work an eight-hour day with or without a ‘support device.’ The total score represents the degree of disability caused by the venous disease. Rutherford et al. 37 recommended revising the VDS to consider the effect of venous disease on the patient's usual activities, not just his or her ability to work a traditional job, and to clarify the support device to represent the usual complementary therapies of compression and elevation. 37
Venous Segmental Disease Score
Secondly, the Venous Segmental Disease Score (VSDS) uses the anatomical and pathophysiological classifications in the CEAP system to generate a grade based on venous reflux or obstruction. Vein segments are evaluated using duplex Doppler or phlebography, which provides the information required to generate the VSDS. Despite the use of ultrasonography, the VSDS has been reported to be arbitrary and difficult to grade. 37,38
Venous Clinical Severity Score
Thirdly, the VCSS was designed by a committee to include nine hallmarks of venous disease scored on a scale of severity ranging from 0 to 3. To avoid confusion with the CEAP scale and to generate a dynamic score, the categories of the VCSS are presented on an elemental basis to add emphasis to the most severe sequelae of venous disease that are likely to show the greatest change in response to therapy. These include skin changes (which were expanded to include pigmentation), inflammation and induration, and ulcers (including number, size and duration). 37 The current version of the VCSS contains a category for compression, with higher scores representing greater compliance.
The VCSS has been discussed extensively in studies 6,32,33,38–43 examining the outcome of therapy for venous disease. The ease of use of the VCSS makes it attractive as a stand-alone scoring instrument for longitudinal surveillance of venous disease in patients undergoing therapy. The clarity of the CEAP scale is represented but in a flexible manner with adjustment capability for physician and patient perceptions throughout the treatment course. 38
In the 2006 study by Mekako et al. 6 comparing the outcomes of EVLT and surgical vein stripping, 132 patients were assessed before treatment and at one, six and 12 weeks after using the SF-36 and the AVVQ. The VCSS was administered before treatment and at 12 weeks. All surveys demonstrated significant improvement in both groups by the 12th week after treatment, with the VCSS and the SF-36 showing no intergroup differences between treatment modality. When classified using the CEAP system, most patients in both groups were classified as C2. The EVLT group had a higher proportion of C4 patients. There were no C0 or C1 patients in either arm and no patients were classified as C6. The VCSS values for both groups dropped to 0 by the 12th week post-treatment. 6
Gillet et al. 32 classified 2894 patients using the CEAP system in a study of patients seeking evaluation of CVI with reflux. After initial screening, 60 patients (71 limbs) were identified as having CVI and were enrolled for further study. All patients were classified as CEAP C3–C6 with deep reflux as identified on duplex examination. All patients were evaluated using the VCSS, VSDS and VDS to assess the severity of their CVI. All elements of the VSS system were found to be useful in disease stratification, with some deficiencies in each. The lack of separate consideration of isolated small saphenous insufficiency by the VCSS presented a problem in scoring. For the VSDS, point assignment for calf vein incompetencies and distinction of the number of incompetent perforators confounded scoring attempts. The main concern regarding scoring of the VDS arose in the assessment of patient activity types and levels that conformed to the definition given by the VDS. There was additional concern in scoring bilateral disease using the VDS.
Increased VCSS values were found to parallel the CEAP classification. In addition, the existence of incompetent perforating veins caused an increase in the VCSS. The VSDS also increased significantly with higher CEAP scores. Higher VDS values, although not significant, were found for CEAP C3 and C6. This finding may have been at least in part due to small sample sizes for C3 and C6. The study concluded that all elements of the VSS system were useful in determining the severity of CVI and that, with some modifications, the VSS system could become useful on a regular basis for evaluation of CVI and the available therapies. 32
Ricci et al. 33 evaluated the VCSS and the VSDS in a cohort of 210 patients with a shared pedigree for protein C deficiency with and without clinical diagnosis or associated symptoms. The intent of the study was to use the VCSS to measure disease severity and to validate the VCSS results with the ultrasonographic measurements provided by the VSDS. The VDS was used as a further confirmatory tool. The VCSS was found to correlate well with the VSDS-assessed abnormalities. An unexpected finding was the ability of the VCSS to act as a screening tool for CVI. When the VCSS was 0, there was little likelihood of correlation with abnormal ultrasonographic findings. The use of the VCSS as a stand-alone screening instrument is discussed, with the caveat that additional validation is required. As a predictive tool, the VCSS could identify patients at greater risk for complications and severe disease. 33
A 2006 study by Perrin et al. 39 on the VSS system examined the value and usefulness of each component among a group of 398 angiologists. Each physician used the VSS components on five consecutive patients with chronic venous disease classified as CEAP C4–C6. Each patient was administered the VCSS to assess the degree of disease severity, the VSDS to measure any reflux or obstruction as noted by Doppler examination and the VDS to note the degree of effect that venous disease had on regular activities. After evaluating five patients, the angiologists completed a questionnaire on the ease of use of the VSS components, the contribution to medical decision-making and the value of regular use in their practice. Although reportedly easy to use, the VDS in their view was more likely to be of value in more severe cases of CVD.
Of 1900 patients evaluated in that study and despite the CEAP C4–C6 inclusion criteria, 484 patients were classified as CEAP C1–C3. On the physician questionnaire, the angiologists reported that the VSS components were straightforward to use and provided valuable information, especially the VCSS. They remarked that scores did not include all possible diseased vessels or bilateral disease. The VSDS was noted to be especially difficult to interpret as a stand-alone measure. In addition, they thought that the VCSS did not adequately represent inflammatory skin changes, including dermatitis. When surveyed as to the willingness of the angiologists to continue to use the VSS parameters in regular patient evaluation and management, there was a discrepancy in opinions based on the patient cohorts. For the original C4–C6 population, 42% of angiologists reported that they would use the VCSS regularly. For the C1–C3 population, only 21.6% thought that it would make a useful regular addition. Scores were similar for the VSDS and the VDS, although the VSDS had the lowest positive response of the components. Among angiologists providing comments regarding the VSS system, 56.6% were unlikely to implement the VSS system on a regular basis in their practices and 16.9% said that the system should be used only in clinical research. 39
The study by Masuda et al. 40 on incompetent perforator veins treated with sclerotherapy examined the effect of treatment on scoring of the VCSS and the VDS. During four years, 80 limbs demonstrating perforator incompetence were treated with ultrasonically guided sclerotherapy. Patients were scored using the CEAP classification, VCSS and VDS before the procedure, less than one month after the procedure, and at three- to six-month intervals for up to five years after therapy. On the pretreatment CEAP classification, 76% of all participants were C4 or higher, with 46% being C6. There were no C0 or C1 scores and all patients reported significant pain at the site of the perforator. The pretreatment median VCSS was 8 and the median VDS was 4. At the initial post-treatment visit, the median VCSS had decreased to 2 and the median VDS to 1. Following perforator sclerotherapy, CEAP C4 and C6 patients demonstrated significant improvement. 40 Although this study did not set out to evaluate the usefulness of the components of the VSS system, it demonstrated meaningful application of the VCSS and the VDS, as well as a correlation between the two in terms of demonstrating significance. The analysis of the CEAP scores further demonstrated the usefulness of combining these instruments in evaluating the outcome of therapy.
Meissner et al. 41 evaluated the validity of the VCSS in a 2002 study involving 128 limbs. Consecutive patients with known chronic venous disease were scored for pain, varicose veins, presence of oedema, pigmentation changes, inflammation, induration, use of compression hose and presence, duration and size of ulcers. Limbs were scored twice by the same observer and again by a second observer. On the CEAP classification, classes C2–C6 were represented and class C1 was excluded. The VCSS values were recorded for each observer and were used to evaluate interobserver and intraobserver variability. The results of this study indicated that the VCSS is a valid measurement tool, with scores increasing as the CEAP clinical class increased. Reliability of the VCSS was confirmed by the results of observer variability measures. There was no significant difference in limbs scored by the same observer during 28 days, and interobserver reliability was good, although there were significant differences between observers. The main areas of interobserver difference were pain scores, pigmentation change measures and inflammation, leading to the question of possible refinements of the VCSS to further clarify these categories. 41
Marston et al. 42 studied the outcome of EVLT or radiofrequency ablation (RFA) in relieving physical symptoms and clinical indications of chronic venous disease. Eighty-nine limbs in 80 symptomatic patients with CEAP C3–C6 were examined using ultrasonography and were scored using the VCSS before and after treatment. The CEAP clinical class breakdown was 37% C3, 30% C4, 12% C5 and 20% C6. The initial VCSS mean score was 11.5, which decreased to a mean score of 4.4 within three months of EVLT or RFA. No significant difference was noted between the VCSS values in patients undergoing EVLT vs. RFA. Long-term follow-up is planned to evaluate the outcome of the procedure and the symptomatic progress over time. 42 The CEAP classification and the VCSS were useful instruments in evaluating patients for minimally invasive therapy and to follow-up clinical and subjective changes.
A 2005 study by Hartung et al. 43 evaluated 48 limbs in 44 patients diagnosed as having chronic obstructive venous insufficiency from non-malignant iliocaval obstructive lesions of greater than 50%. Patients were scored by CEAP clinical class, with 23% C2, 65% C3, 8% C4, 2% C5 and 2% C6. All patients had VCSS and VDS values obtained before treatment and at one, three, six and 12 months after treatment. The median VCSS improved from 8.5 to 2 and the median VDS from 2 to 0 during the 12-month follow-up period. The VCSS and the VDS were used in this study to measure the effectiveness of stenting as treatment for occlusive lesions. The improvements in both instruments during the follow-up period indicated the value of therapy and the usefulness of the survey. 43
In our study, 38 we set out to evaluate the usefulness of the VCSS in patients undergoing saphenous vein RFA therapy. Four hundred and ninety-nine patients (682 limbs) seeking evaluation of chronic venous disease were scored by CEAP clinical class and by the VCSS before and after the procedure. The preprocedure CEAP clinical classifications were as follows: 7% C2, 64% C3, 16% C4, 5% C5 and 8% C6; the preprocedure mean VCSS was 8.8. Patients were followed-up with duplex Doppler after the procedure at four days, four weeks, four months and 12 months, with the VCSS administered at each visit. All components of the VCSS demonstrated significant improvement at each postprocedure visit (P < 0.001 for all), except for the compression component, which varied throughout the follow-up period. At the initial postprocedure visit, the greatest improvement was noted in the pain, varicosity, oedema and inflammation components (Figure 1). The overall mean VCSS for all 10 components decreased from 8.8 to 5.2 at the first follow-up visit. During the follow-up period, all VCSS components continued to improve, reaching a significant mean of 3.3 at the four-month visit (P < 0.001). The ulcer components of the VCSS proved useful in tracking the number, size and duration of stasis ulcers after RFA, with 86% of ulcers healing by the four-month follow-up. This serial application of the VCSS indicated usefulness as a stand-alone instrument to track changes in symptoms and clinical manifestations over time following RFA. The VCSS components were found to be easy to use and to follow-up throughout the study. 38
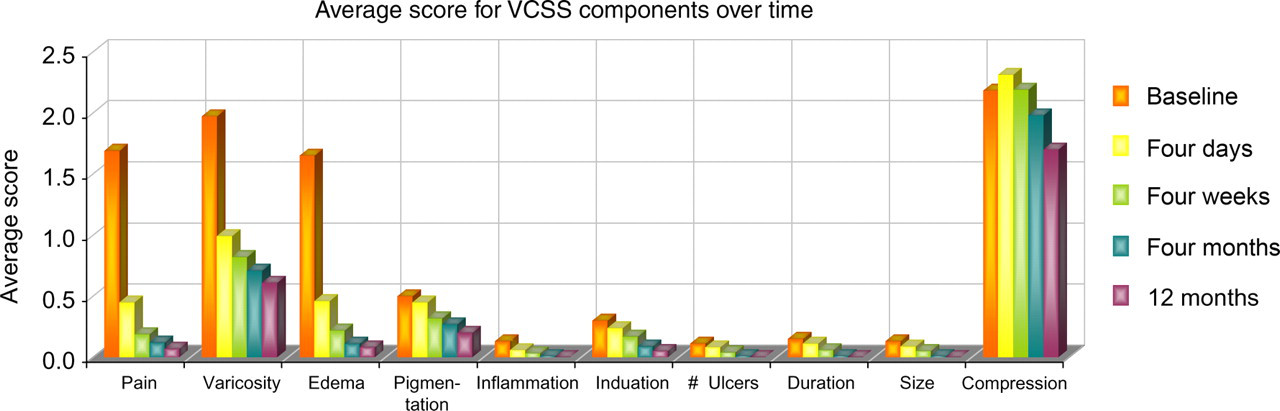
Scores for each Venous Clinical Severity Scoring component showed significant improvement at each time interval over the course of follow-up
The strength of the VCSS lies in its evaluative properties in identifying subtle intrasubject changes after an intervention over time. 38 An evaluation of each VCSS component allows outcome analysis on many levels, including technical, patient-reported and clinical. In this sense, the VCSS is unique among clinical outcome assessments and quality-of-life instruments. Although it is administered by a physician, components such as pain are scored based on patient responses to subjective questions. In contrast to more focused instruments such as the AVVQ and the CXVUQ, the VCSS considers most of the salient features of vein disease through clear categories and evaluative parameters for each of its 10 components.
With our experience using the CEAP classification and the increased VCSS, we have become comfortable using them to evaluate changes in patients of all CEAP clinical classes. Although the usefulness of the VCSS has been previously recognized in patients with moderate to severe (C4–C6) disease, 39 patients with even minor symptoms improve after superficial vein ablation. 2,6,38,42 Having a single tool to evaluate patients at all CEAP clinical levels allows assessment of outcomes throughout the spectrum of chronic venous disease. Figures 2 –6 give examples of the ease of application of each component of the VSS system among patients who are commonly seen.

The ‘visual language’ of Venous Clinical Severity Scoring (VCSS). Consistency in physician scoring and reporting allows a common language of venous disease to emerge. Basic Clinical CEAP 3, VCSS 8

(a) Venous Clinical Severity Scoring (VCSS) scoring is useful in severe venous disease, both to evaluate and track progress. Initial Clinical CEAP 6, VCSS 26. (b) Initial Clinical C6 – V26 changes to C5 – V12 one month post-treatment
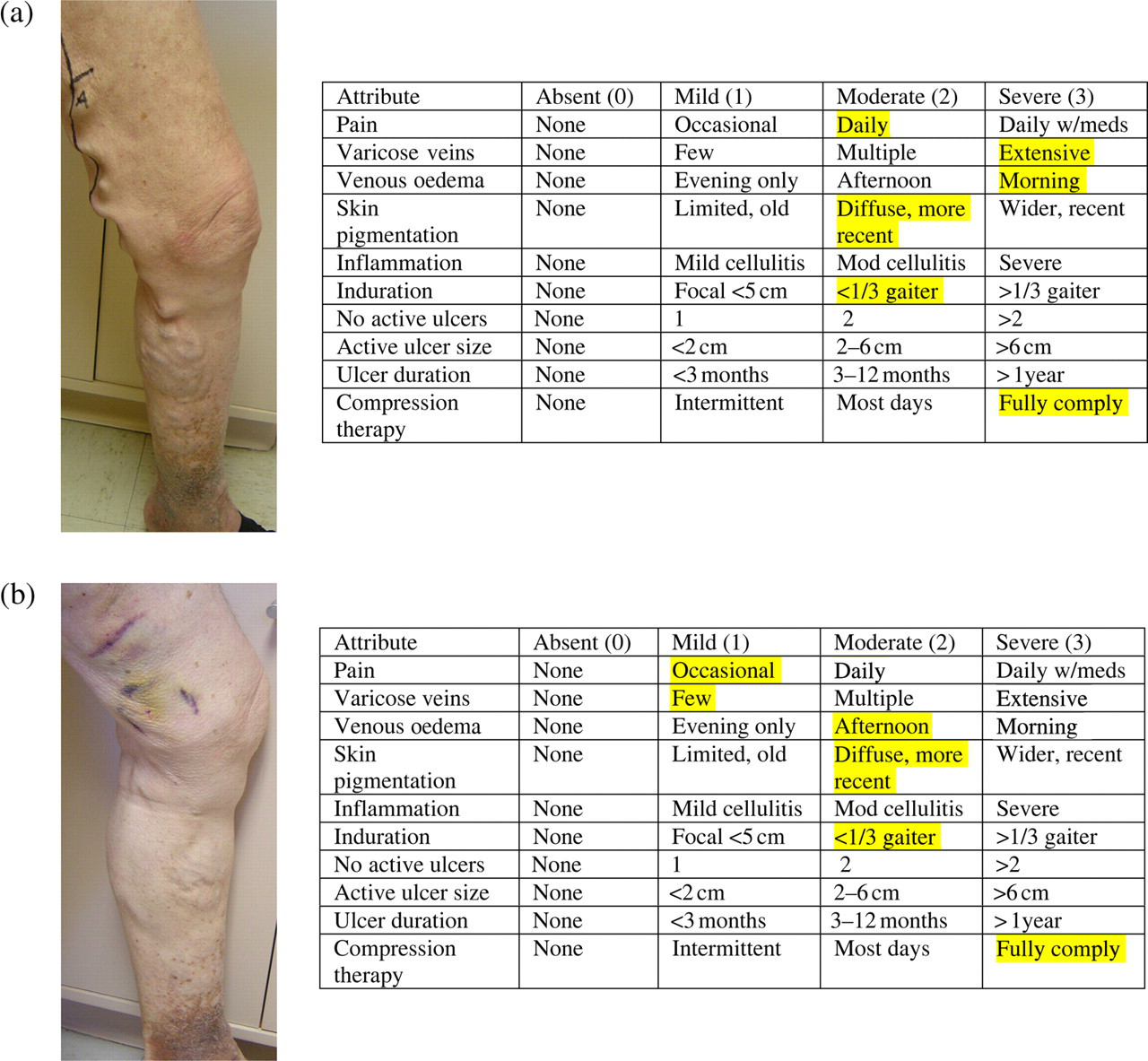
(a) Venous Clinical Severity Scoring (VCSS) Scoring illustrated. Clinical C4 – V15. (b) The difference between the same CEAP C4 patient before and after treatment. C4 – V15 changes to C4 – V11
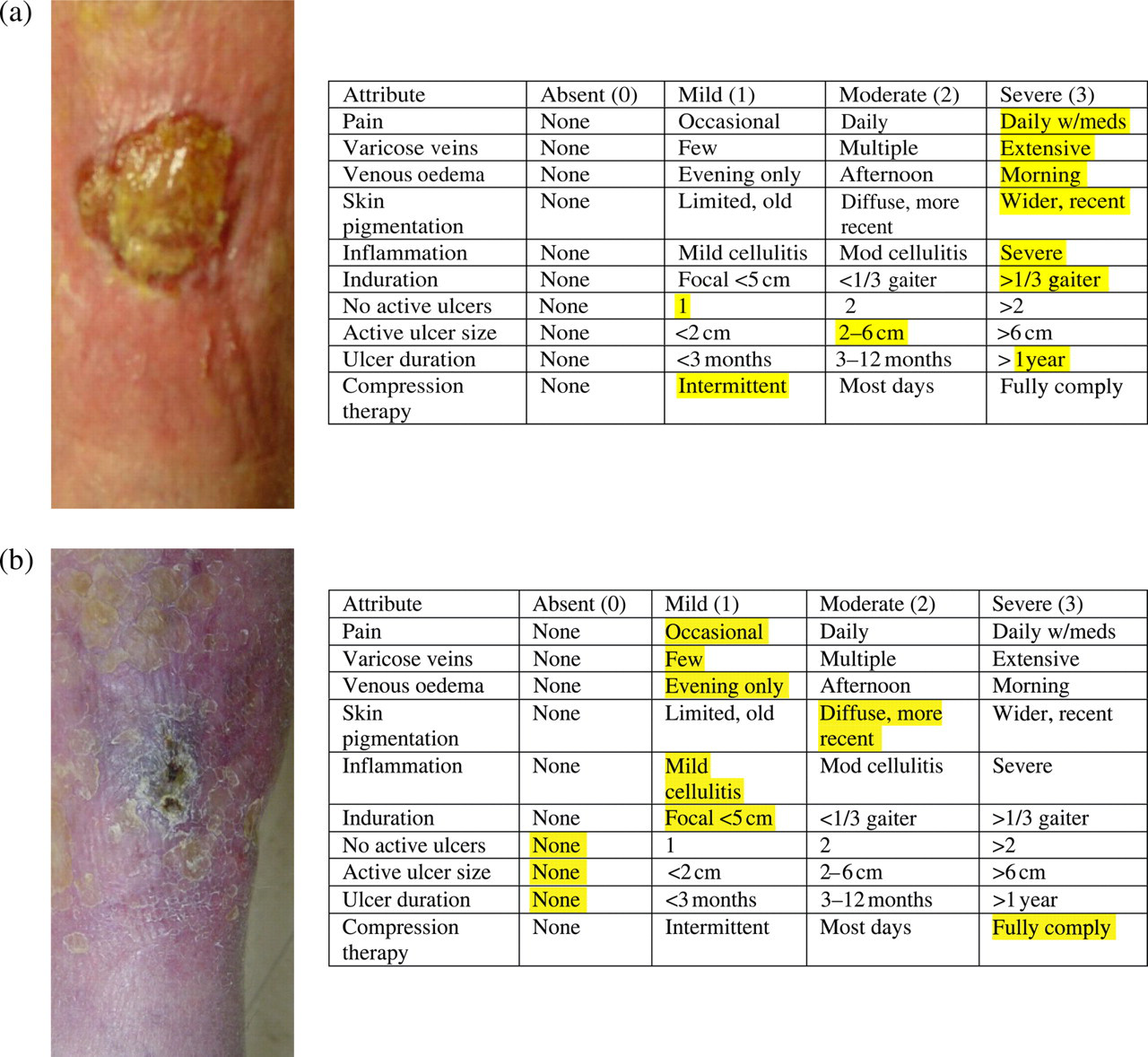
(a) The continuum of Venous Clinical Severity Scoring for an ulcer. C6 – V25 at initial scoring. (b) The healing ulcer. After 47 days, the same patient is now scored C5 – V10

The physician-generated ‘universal language’ of Venous Clinical Severity Scoring and CEAP scoring cardiovascular disease. The same patient changes from C6 – V27 to C6 – V19 and at last C5 – V5
The VCSS has proven to be a useful assessment tool that is easy to administer. However, there has been critical review of its elements and its validation. 32,33,39
Gillett et al. 32 used the CEAP classification and all three VSS components (the VCSS, VSDS and VDS) to evaluate a cohort of patients with deep venous reflux. The value of using all three measurements not to evaluate treatment but to confirm the presence of venous disease and to quantify severity was noted. They saw this application of the VSS system as a benefit in the evaluation of patients with chronic venous disease. However, they believed that, for the VSS components to become part of the regular clinical evaluation of patients, some clarification was required. In terms of the VCSS, the lack of separate consideration for small saphenous insufficiency was seen as problematic, as was some confusing language regarding the scoring of different types of oedema and pigmentation changes. Questions also arose about compression therapy and scoring, especially regarding compression with and without limb elevation and the strength of compression. 32
Ricci et al. 33 used the VCSS, VSDS and VDS in evaluating patients with chronic venous disease. They found that the VCSS and the VSDS were useful in evaluating the outcome of therapy. The VCSS was not evaluated as a stand-alone instrument. Although they saw value in the VCSS as a clinical screening tool, they believed that prospective validation needed to be in place first. 33
The study by Perrin et al. 39 of VSS evaluation among French angiologists also identified some areas of recommended change in the VCSS. Although they noted that the VCSS is easy to score and is relevant in patients with chronic venous disease, there were areas that require clarification. Most notably, the question arose as to the precision of the VCSS in evaluating skin changes that were not necessarily classical pigmentation changes, including dermatitis and hypodermic inflammation. 39
Outcomes revision project
In light of the revision of CEAP scoring and in consideration of these and other reviews of the VCSS as a valid but imperfect instrument to evaluate the severity of venous disease and the outcome of therapy, it seems that the time has come to revise the VCSS. The question of precisely what this revision should include has been raised among researchers and clinicians charged with designing a single instrument that will be reliable, valid and easy to use, while retaining sensitivity during the course of therapy.
In our use of the VCSS, care has been taken in the study design and protocols to avoid confusion in scoring and to ensure completeness of results reporting. We try to incorporate a method for scoring most of the manifestations of venous disease based on what we see and what patients relay to us. We believe that a revision in the VCSS would be helpful; however, only symptomatic patients will derive the benefit of this tool. In our study, 38 74% of patients were CEAP C2 and C3, and significant changes were noted in these patients over time. Nevertheless, adding cosmesis to this type of clinical outcome reporting that this tool is inappropriate.
Kakkos et al. 31 recommend revision of the VCSS by possibly removing elements that would make it easier to use without affecting the sensitivity to the spectrum of venous disease. Their initial recommendation is to further evaluate the static measurement elements most often found in CEAP C4–C6 patients, including induration and pigmentation changes. They recommend research among a large patient cohort to examine elements that could likely be removed.
In compiling the current scale, the American Venous Forum's Ad Hoc Committee on Venous Outcomes Assessment 37 intended that the VCSS would need to be modified based on objective findings of future research. The primary notion is to reassess the VCSS for focused revision and not for complete overhaul. Keeping the framework of the current version of the VCSS intact, while refining some elements, will enhance the ability of the VCSS to provide evidence-based evaluation of all outcome measures, while allowing ongoing clinical trials using the VCSS to continue with only minor adjustments.
With these thoughts and opinions on the future of the VCSS and its necessary revisions, where do we stand on the use of this measurement tool in evaluating the disease process and the therapeutic outcome in chronic venous disease? We believe fully in the usefulness and the easy applicability of the VCSS for all venous practitioners. Those who treat patients who suffer want to follow-up their clinical outcomes because these practitioners know that they are making a difference. They want a system that they can rely on and that they can use to compare outcomes with others elsewhere. If the VSS system, especially the VCSS, is modified and refined to a form that is palatable and valid, it would have tremendous international appeal.
Clarification and revision of the VCSS should be sufficient to incorporate all common symptoms of venous disease into pretreatment and post-treatment scores. Major changes are not required to accomplish these goals. We can take a page from the well-received revision of the CEAP consensus statement as an excellent model of an accepted refinement. Descriptors and subclassifications were added to the existing information to increase the relevance of the instrument. Similarly, the VCSS could be revised by adding subclasses to existing categories to include more features of chronic venous disease.
The obvious truth is that QoL and the VCSS are complementary tools. Quality-of-life language is descriptive, comprehensive and patient-centred. That is why QoL is widely appreciated by so many practitioners and payors. We believe that descriptive quality-of-life language should be added to the VCSS to clarify and improve it. Because the VCSS is physician-driven, this seems to be the natural conclusion. If we can find a way to marry the two tools, we can have something truly powerful to engage clinically.
For example, the pain component of the VCSS is the most subjective measurement in the survey. The terms achiness, heaviness, tightness, cramping, burning, soreness and fatigue need to be included to allow proper reporting of common patient symptoms. The vein component should be broadened to include vessel turgidity or size to reflect appropriate decompression after treatment, although the distribution of veins remains unchanged. For the oedema component, many patients with CVD are found to have reflux-related oedema without varicosities. A method for reporting this would be useful in isolating this condition. In consideration of the pigmentation component, the Bonn Vein Study 15,16 discussed the incidence of ‘corona phlebectatica’ among patients with CVD. Adding this to the VCSS is reasonable as long as it is differentiated from routine telangiectasias. The terms white atrophy and lipodermatosclerosis could be included here as well. The inflammation component needs to be more permissive. ‘Cellulitis’ alone is insufficient to describe the inflammatory issues encountered in CVD. 37 Erythema, subdermal irritation, venous eczema and phlebitis should be included in this component. Consideration might also be given to the classification of a scab formed over a recent bleeding varix.
The compression component has been debated extensively in discussions of the VCSS revision. We believe that it needs to remain part of the VCSS in the future. Compression is a measure of compliance and affects disease severity. In fact, compression has no impact on the severity score if the background of compression and/or leg elevation is not changed during the therapy. However, compression prevents some researchers and practitioners from using the VCSS. A solution to this conundrum is found in the example of the revised CEAP classification. In the revised CEAP system, the subscripts ‘a’ and ‘b’ are used to clarify C4 disease. In a similar light, for the VCSS we might implement an ‘initial visit’ or a ‘non-compliant’ qualifier. Subscript ‘a’ might indicate a patient in compression garments and subscript ‘b’ a patient not using compression for whatever reason. This would allow flexibility when comparing studies containing patients using or not using compression therapy. The American Venous Forum Outcomes Committee, of which one of us (MAV) is a member, is debating the issue of including or discarding the compression component.
Universal consensus
Will we arrive at a universal consensus as to which outcome tool we should use? It is incumbent on the responsible practitioner to do so. We can rein in this ‘veins gone wild’ scenario by facilitating the use of a responsive instrument. However, we have to find a way to use these tools together. Quality-of-life instruments are valuable indicators of patient perspective and are proven to be reliable, but the number of choices seems overwhelming. The VCSS is physician-driven, practical and proven, but needs refinement. To blend the patient language of QoL with the physician evaluation of the VCSS seems too obvious a solution to ignore. What powerful simplicity! At the 2006 American Venous Forum's Hawaiian Forum, Eklöf et al. 44 proposed venous disease standardization based on four activity phases comprising discovery, dream, design and destiny. This will pave the way for a positive future in the management of venous disease. The word imua is Hawaiian for ‘moving forward’ and summarizes the forum's intent to welcome advances in research and clinical practice in the coming years. 44
Therefore, our opinion is this: for physicians who want to follow their results and to learn from them, a revised VCSS can bring us together. As the progeny of the clinical CEAP classification, a revised VCSS has a precedent in the revised CEAP system and provides common physician-driven clinical language that we all speak. A revised VCSS that incorporates the language of QoL can become a tool that we will use and from which we will benefit. Furthermore, when a physician says that a patient is C6 – V27, who after treatment becomes C6 – V19 and one month later is C5 – V5, you will know what he or she is talking about (Figure 6)!
In his presidential address to the American Venous Forum, Meissner asserts: ‘As physicians, we also have obligations to our individual patients and to society. All of us should commit to evidence-based practice, understanding that this does not require submitting to “a tyranny of the evidence”, but integrating our own clinical expertise with the patient's values and preferences… we need to individually participate in both scientifically questioning the existing evidence and generating new evidence'. 10 With the goal set to provide high-quality comprehensive care in the treatment of venous disease, we believe that the international venous community needs to arrive at a consensus as to how outcomes will be assessed and reported. Erratic reporting with differing measures around the world is useless to appropriately compare results. For those of us who are willing to subject ourselves to public scrutiny, who are driven to find something better for our patients, and for those who are willing to change what we do based on what we find, we need to follow-up and compare our outcomes or acquiesce limply to the status quo.
So, we ask you again: (1) Do you believe that it is important to follow clinical outcomes in venous disease? Yes or no; (2) What do you believe is the predominant reason why you currently do not follow your outcomes more closely? (a) Do not care; (b) too cumbersome or time-consuming; (c) do not see the value; (d) have not figured out the available tools; or (e) no uniformly accepted standard. Where do you stand?