
Abstract
Objectives
A variety of endovenous therapies for the treatment of superficial venous incompetence are currently available. The aim of this study was to evaluate the prevalence of endovenous techniques used by consultant vascular surgeons in the United Kingdom.
Methods
An anonymous online survey of 16 multiple choice questions relating to the nature and provision of treatment for varicose veins was devised. Consultant members of the Vascular Society of Great Britain and Ireland were invited to participate by email.
Results
A total of 108/352 (31%) surgeons completed the survey. The majority offered surgery as the first-line treatment for primary great saphenous vein (GSV) and small saphenous vein (SSV) incompetence (69% and 74%, respectively). Endovenous procedures were offered as first-line treatment by 32/108 (29.6%) for GSV reflux, 36/51 (70.6%) surgeons performed these under local anaesthetic and 21/51 (41.2%) were performed as an outpatient procedure. The most important factor influencing treatment decisions was considered to be patient preference by 77/108 (71.3%) surgeons, although 48/61 (78.7%) respondents were restricted by primary care trusts with regard to endovenous treatments, and 33/108 (30.6%) offered different treatments to private patients.
Conclusion
Traditional surgery remains the most commonly offered treatment for patients with varicose veins. The provision of endovenous therapies varies greatly, and there are significant differences in local availability regarding these treatments.
Introduction
Varicose veins are a common clinical problem affecting approximately 30% of the UK population. 1 Patients seek treatment for a number of reasons ranging from cosmetic concerns to chronic venous ulceration. Traditionally, surgical treatment consists of saphenofemoral disconnection and stripping of the great saphenous vein (GSV). This is known to be effective, but may be associated with wound complications, high recurrence rates and subsequently a degree of patient dissatisfaction. 2–4 In recent years, minimally invasive endovenous techniques have become increasingly popular in the United Kingdom as an alternative to traditional surgery. Previous postal surveys conducted in 2005 showed that endovenous treatments, including laser and radiofrequency ablation, were used by less than 30% of surgeons in the UK. Interestingly, over 50% of surgeons reported local referral guidelines restricting the treatment of varicose veins in 2005, and in the majority of cases the use of endovenous techniques was restricted to private practice. 5,6 Foam sclerotherapy was reported to have been used by 20–42% of surgeons in postal surveys conducted in 2006 and 2007. 6,7
The aim of this study was to evaluate the prevalence of endovenous techniques used by consultant vascular surgeons in the United Kingdom.
Methods
A questionnaire consisting of 16 multiple choice questions was designed by members of Imperial Vascular Unit at Charing Cross Hospital and an online survey was created using an academic online survey website. 8 Consultant members of the Vascular Society of Great Britain and Ireland (VSGBI) with published email addresses were invited to participate by email. The questions related to the following: routine treatments offered to patients with varicose veins; use of venous duplex scanning; indications for re-intervention; anaesthesia and the location in which the treatment was performed; factors influencing the decision regarding treatment; the use of postoperative compression and thromboprophylaxis; restrictions imposed by primary care trusts regarding treatment of varicose veins and the nature of treatments offered in the private sector (see Appendix). All responses were anonymous. Where responses were incomplete, the number of responses received for that particular question was given as the denominator.
Results
A total of 352 consultant members of the VSGBI were contacted by email and invited to complete the survey; there were 108 responses, of which 80 were complete.
Current use of endovenous treatments
The majority of surgeons, 99/108 (91.6%), regularly performed traditional surgery for varicose veins, whereas sclerotherapy was routinely performed by 66/108 (61.1%) and endothermal procedures were frequently performed by 48/101 (48%) surgeons (endovenous laser therapy [EVLT] by 43 and radiofrequency ablation [RFA] by 11 respondents); 23/101 (23%) respondents did not offer any endovenous procedures. Traditional surgery was the most frequently performed treatment for GSV and small saphenous vein reflux (see Figure 1). Of the surgeons offering endovenous treatment, half performed concomitant phlebectomies for varicosities and half performed subsequent sclerotherapy of varicosities, if required. In patients deemed suitable for all treatment modalities, 60/108 (55.6%) surgeons performed traditional surgery, whereas 24/108 (22.2%) preferred EVLA. Radiofrequency ablation (6/108) and foam sclerotherapy (11/108) were used relatively less frequently (5.5% and 10.2%, respectively).
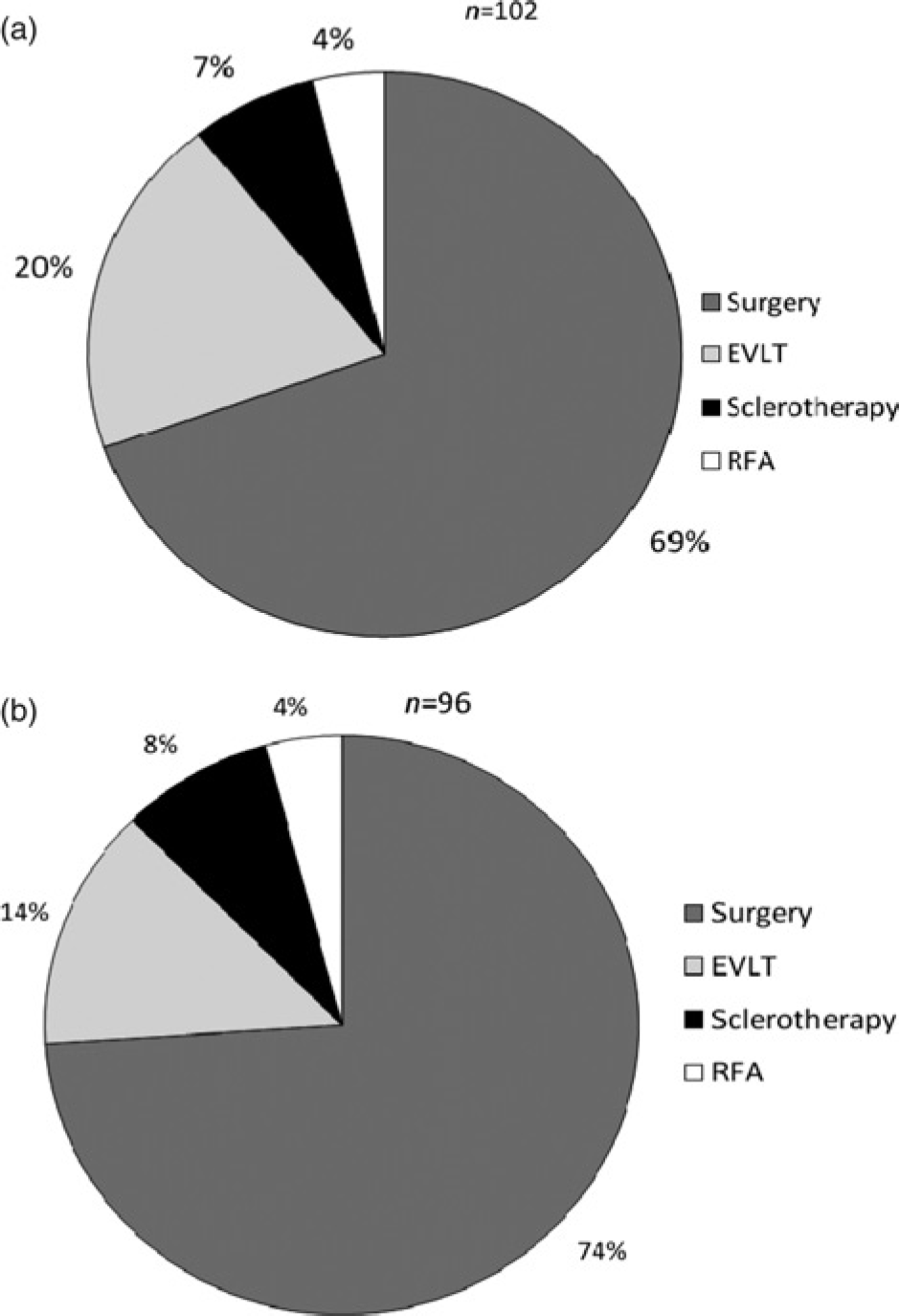
(a) First-line treatments offered to patients for great saphenous vein incompetence (b) First-line treatments offered to patients for small saphenous vein incompetence
A total of 77/108 (71.3%) surgeons stated that patient preference was the most important factor when deciding which treatment to offer. The time taken for the procedure, cost or space considerations were considered relatively unimportant.
Anaesthesia and location of treatment provision
Endothermal treatments were performed in an operating theatre by 30/51 (58.8%) surgeons, with the remainder performed in an adapted outpatient clinic or outpatient theatre. Local anaesthesia was used by 36/51 (70.6%) surgeons performing endothermal treatments, whereas one surgeon used regional anaesthesia and the remaining 14/51 (27.5%) preferred general anaesthesia. Almost half the endothermal treatments (25/51, 49.0%) were performed with concomitant phlebectomy, with the intention of completing treatment in a single hospital visit.
Thromboprophylaxis
In total, 66/98 (67.3%) prescribed subcutaneous heparin or low molecular weight heparin and 42/98 (42.9%) advised TED stockings. Of those prescribing subcutaneous heparin, 42/66 (63.6%) would use a single dose only, 18/66 (27.3%) would prescribe it for the duration of their inpatient stay and two surgeons would routinely advise it for one week. Two surgeons prescribed subcutaneous heparin for bilateral or recurrent varicose veins only and many commented that they may alter thromboprophylaxis based on the individual risk of the patient. Four surgeons stated that they would not use pharmacoprophylaxis for patients undergoing foam sclerotherapy; however they would do so for endovenous or traditional surgery. A total of 16/98 (16.3%) did not routinely prescribe any form of thromboprophylaxis; of these 6/16 were performing surgery and foam sclerotherapy only, 6/16 were performing all treatments, 1/16 was performing EVLA and foam sclerotherapy, and 3/16 were performing surgery only.
Postoperative management
Postoperative compression was most frequently recommended for 7–14 days (Figure 2). Over half of the surgeons, 54/101 (53.4%), applied compression bandaging immediately following the procedure, which was replaced with TED stockings (<18 mmHg) prior to discharge (usually within 24 hours) whereas 6/101 (5.9%) replaced the bandaging with TED stockings after 24 hours. Grade I (14–17 mmHg) and grade II (18–24 mmHg) graduated compression stockings were used by 8/101 (7.9%) and 16/101 (15.8%) surgeons, respectively. Some surgeons, 14/101 (13.8%), did not use elastic compression hosiery and preferred bandaging, usually crepe, Pannelast® (Vernon Carus, Preston, UK) or Coban™ (3M™, Berkshire, UK). There was considerable variation in regimes and duration of compression.
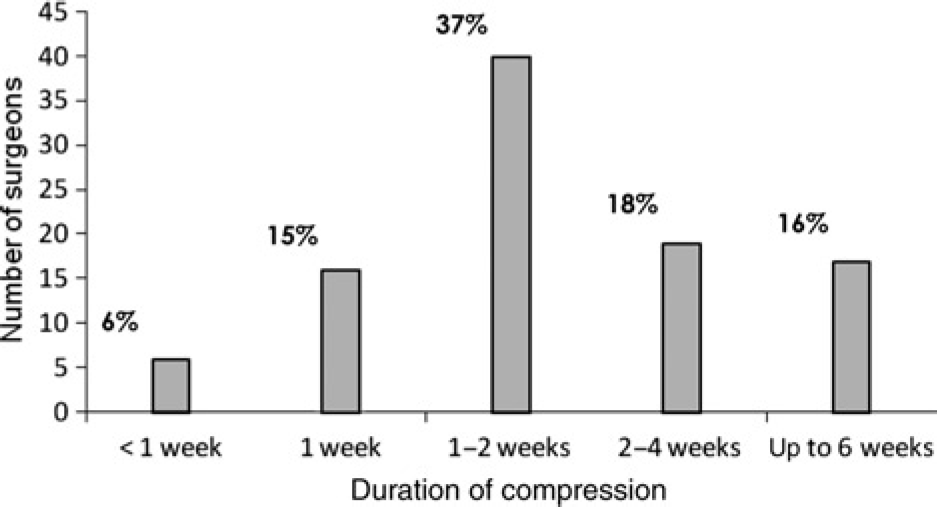
Duration of compression prescribed by surgeons following varicose vein treatment
Following traditional surgery, only 2/108 (1.9%) surgeons would routinely perform colour duplex, whereas 30/48 (62.5%) would investigate patients with colour duplex after EVLT or RFA and 33/71 (46.5%) would do so following foam sclerotherapy. The commonest stated reason for postoperative duplex was to ensure successful ablation of the treated vein (29/38 [76.3%] following EVLA, 17/21 [81.0%] following RFA and 29/44 [65.9%] following foam sclerotherapy). Of the surgeons who performed colour duplex following treatment, 10/51 (19.6%) would re-intervene following endothermal treatments and 14/68 (20.6%) following sclerotherapy, if a patient still had truncal incompetence even in the absence of clinical symptoms. No surgeons reported that they would offer additional intervention in the absence of clinical symptoms following traditional surgery.
Local rationing of varicose vein treatments
Local restrictions to the provision of varicose vein treatment were reported by 48/108 (44.4%) respondents. Restrictions were imposed on 28/108 (25.9%) surgeons offering open surgery and 23/80 (28.8%) of those offering foam sclerotherapy; however, 48/80 (60.0%) and 48/61 (78.7%) surgeons reported restrictions regarding the use of EVLT and RFA, respectively. The lack of funding for endovenous equipment was given by many surgeons (28/80 35%) as the reason for not performing endovenous procedures, although the lack of theatre time, space due to pressure from other departments, the lack of a laser approved room and the fact that traditional surgery was cheaper than laser or radiofrequency were also given as reasons. When asked about the treatment of private patients, 33/108 (30.6%) surgeons stated that they would advise venous treatments that they were unable to offer in their National Health Service (NHS) practice.
Discussion
This online survey of consultant vascular surgeons in the UK conducted in 2008 showed that traditional surgery is still the most widely offered treatment for varicose veins, despite the apparent increasing popularity of endovenous procedures. These findings mirror the results from a recent postal survey of consultants and vascular trainees published in 2008, which reported that the majority (96%) of surgeons were performing conventional surgery, 27% were offering foam sclerotherapy, 19% were offering EVLT and 3% were offering RFA to NHS patients. 6 However, these data appear to show a small increase in the use of endovenous therapies, compared with previous surveys, 5,7 suggesting a slow movement towards newer techniques. Many surgeons who were performing endovenous treatments were favouring procedures performed under local anaesthetic and a significant number performed treatments on an outpatient basis. Although this survey asked which treatments surgeons were able to offer and why, it did not investigate the patients' perspectives. Research has shown that patients generally have little knowledge of treatment options prior to their consultation and so are likely to rely strongly on the opinion of the physician at their initial consultation, 9 which will undoubtedly be influenced by the treatments they are able to offer. The lack of uptake of endovenous procedures may be due to the high initial costs of endovenous equipment and training, at a time when varicose vein surgery is subject to increasing scrutiny and significant funding restrictions by a large number of health-care providers. 10,11 At present, both laser and radiofrequency equipment are readily available; however, the cost of the generator and catheters varies significantly between the two. Undoubtedly, the cost-effectiveness of new therapies will be under great scrutiny prior to widespread use.
Despite reminder emails, the response rate in this survey was disappointingly low. Response rates from postal surveys in the UK are extremely variable; recent postal surveys sent to both consultants and vascular trainees had significantly higher response rates 5,6 but other postal surveys have achieved similarly poor responses. 12 Our response may be due to inaccurate or unavailable email addresses, but may also reflect a reluctance on the part of consultant vascular surgeons to engage with online surveys. Indeed, responses to previous email surveys appear to have had a poorer response rate compared with postal surveys among vascular surgeons. 11 Research into the response rates comparing postal surveys with email/web surveys sent to medical professionals confirms that the response rate is frequently lower from electronic surveys; however, electronic surveys have been shown to result in a more rapid response at lower cost compared with postal surveys. 13–15 We acknowledge that these limitations may mean that our findings are not truly representative of the entire UK practice, with enthusiastic advocates for endovenous therapies or more computer-literate surgeons potentially being more likely to respond.
At present there is no consensus regarding the nature and duration of postoperative compression that should be applied following surgical or endothermal procedures. Evidence suggests that TED stockings are adequate following foam sclerotherapy; 16 however, compression following endothermal treatments varies widely throughout the country. 16 This study highlighted the wide variations in practices in terms of thromboprophylaxis, postoperative compression and use of duplex imaging. Interestingly, postoperative duplex use and treatment of residual truncal reflux varied between traditional and endovenous treatments. As the prevalence of varicose veins is high, it is likely that patient demand for treatment will remain high for years to come. Each treatment modality has advantages and disadvantages, but long-term outcomes are unclear. This confusion is demonstrated by the huge variability in treatment modality, type of anaesthetic, location of therapy and postoperative management in this survey. With patient choice regarding treatment becoming ever more important, further evaluation of patient preferences regarding treatment strategy is required. Despite the introduction of minimally invasive treatments for varicose veins, traditional surgery remains the most frequently performed treatment for varicose veins in the United Kingdom and in Europe. 17 Of the surgeons performing endovenous treatments, perioperative management varies greatly. It is clear that further clinical trials are needed to clarify some of these issues and guide clinical practice.
Footnotes
Acknowledgements
The authors would like to thank the members of the Vascular Society of Great Britain and Ireland who completed this survey.