
Abstract
Lasers have affected health care in many ways. Clinical applications have been found in a number of medical and surgical specialities. In particular, applications of laser technology in phlebology has made it essential for vein physicians to obtain a fundamental knowledge of laser physics, laser operation and also to be well versed in laser safety procedures.
This article reviews recommended text books and current literature to detail the basics of laser physics and its application to venous disease. Laser safety and laser side effects are also discussed.
Keywords
Introduction
Lasers are used today in many medical and surgical specialties. A variety of different lasers have been developed to treat leg telangectasia. Recently, endovenous laser ablation (EVLA) has been introduced for the effective treatment of varicose veins. It has become essential for the phlebologist to understand the basic principles of how light interacts with tissue as well as how to use lasers safely and effectively.
Laser concepts
Spontaneous and stimulated emission
Most atoms exist naturally in a low energy (ground) state. Electrons in their ground state can be excited to a higher energy state when they absorb thermal, optical or electrical energy. An electron in a higher energy orbit is unstable and wants to return to the ground state; when it does, it releases its defined energy as a photon (particle of light). The amount of energy released determines the wavelength or colour of the light emitted. This is known as spontaneous emission (Figure 1). In spontaneous emission the photon emitted travels in random directions.

Spontaneous emission: this process occur when the electron is in its upper state and spontaneously returns to its ground state, releasing its defined energy as a particle of light/photon (
If an electron already in an excited state encounters a photon of the proper energy, the electrons drop to a lower orbit and emit a photon. The stimulating photon is not absorbed but continues on its way, resulting in two photons of identical energy or wavelength. Einstein called this stimulated emission (Figure 2).
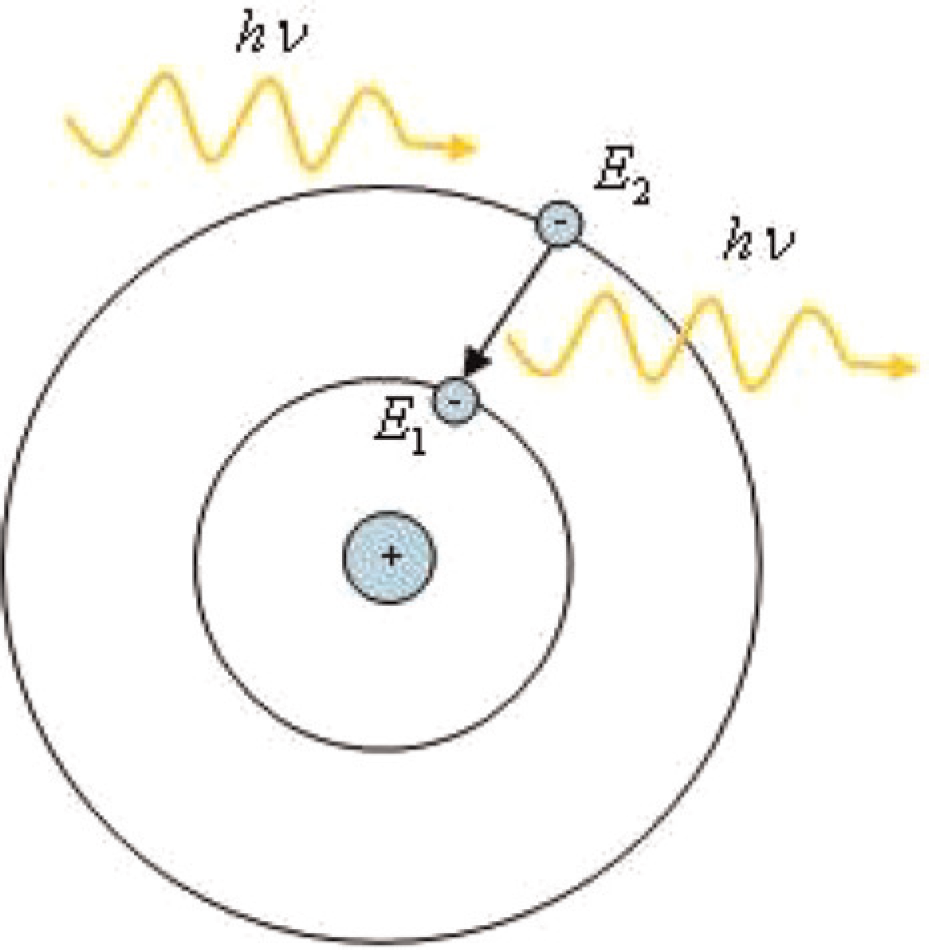
Stimulated emission: it occurs when the electron is in its upper level and an electromagnetic radiation at (or near) the same frequency is present: it can emit an additional photon by stimulated emission decaying to the lower energy level (
In nature, spontaneous emission is dominant. Atoms try to be in their lowest possible energy states and remain excited for such a short time that there is little chance of the right photon coming along to produce stimulated emission. 1
Population inversion
For stimulated emission to predominate it is necessary for more electrons to be in the upper energy level. This is known as population inversion. Population inversion is created by pumping electrical or light energy into the population of atoms (the gain medium) to move them to higher energy levels.
When the laser is switched on, the gain medium is pumped, population inversion occurs and individual atoms in the population undergo spontaneous emission, emitting photons in random directions. A photon will pass by an atom with electrons in the upper level and cause it to emit a second photon travelling in the same direction, phase and wavelength. There are now two photons; each can cause stimulated emission and give four photons, etc.
Amplification
The final stage is to get the photons to continue amplifying; this is done by placing the gain medium between two mirrors. One of these emitted photons, purely by accident is in the axis of the two mirrors and is reflected back into the gain medium, continuing the amplification. Each photon reflected back causes stimulated emission and photon numbers go on increasing; this chain reaction causes an avalanche of coherent light (Figure 3). 2,3

(a) Pumping of an active medium and starting of the population inversion. (b) The reflected photons transverse the cavity, they stimulate other atoms to emit photons and the beam builds up. Amplification. (c) Almost the complete medium contributes to the stimulated emission and laser action takes place (encyclopedia2.thefreedictionary.com)
One of the mirrors is designed to allow some of the light through. This is the output beam. The beam is monochromatic, collimated and coherent (Figure 4).

A laser consists of a pumped amplifying medium positioned between two mirrors (
Laser construction
The basic laser device consists of three components: an energy source or a pump, a gain medium and two mirrors that form an optical resonator. The pump source provides energy to the laser system. Pump sources include electrical discharges, flash lamps, light from another laser and even chemical reactions. The type of pump source used principally depends on the gain medium.
The gain medium is the major determining factor of wavelength and energy emitted by the laser and can be a gas, liquid, solid or semiconductor (diode laser). It is in the gain medium that spontaneous or stimulated emission of photons takes place.
The optical resonator, or optical cavity, in its simplest form is two mirrors at each end of the gain medium. Light from the medium, produced by spontaneous emission, is reflected back into the medium many hundreds of times amplifying the beam. The output mirror allows some of the light to escape (Figure 4).
Thus we have LASER: Light Amplified by Stimulated Emission of Radiation. 2,3
Radiation
Radiation means electromagnetic radiation, a form of energy that travels at the speed of light and spreads out or radiates. It comes in various forms including visible light, infrared, ultraviolet, radio waves, microwaves and X-rays. Electromagnetic radiation carries energy and momentum that may be imparted when it interacts with matter.
The electromagnetic spectrum is a complete range of electromagnetic waves (waves with both electric and magnetic components) ranging from those with low frequency and energy levels along with correspondingly long wavelengths to those with high frequency and energy levels with correspondingly short wavelengths (Figure 5).

Electromagnetic spectrum (
This relationship is explained by the formula:
5


Laser–tissue interaction: when laser energy hits a target tissue it may be transmitted, scattered, reflected or absorbed (
Qualities of laser light
Laser light is monochromatic – of one wavelength or colour (if within the visible light spectrum). A laser's characteristic wavelength is associated with the energy gap between electrons in the ground state and electrons in the excited state.
Laser light is coherent – this refers to the wave nature of light; the peaks and troughs occur synchronously or in phase.
Laser light is collimated – the light rays are parallel, non-diverging unlike conventional light sources that emit light in all directions. This property allows a laser to be more powerful than ordinary light of the same power. If light from a 60 W bulb enters the eye it would not damage the retina. A collimated beam is a focused, concentrated light and is damaging to the eye at much lower power.
So we know that a laser device converts energy to a concentrated light of a particular wavelength, but what happens when the laser beam interacts with living tissue?
Laser tissue interaction
A variety of interactions occur when applying laser light to biological tissue.
When laser energy hits a target tissue it may be reflected, scattered or absorbed (Figure 7). These optical tissue properties determine the total transmission of the tissue at a certain wavelength. 4
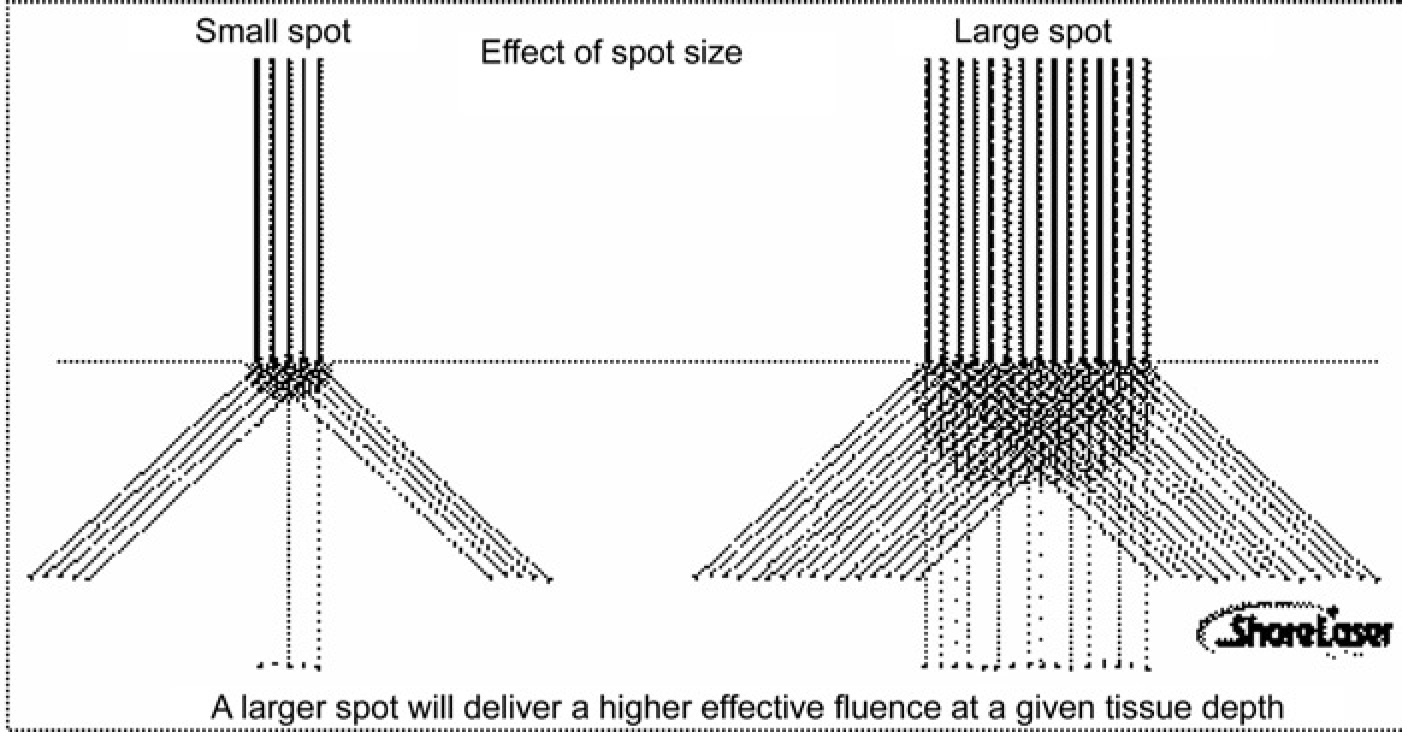
Scattering and spot size: scattering in tissue broadens the incident beam, decreasing the effective fluence in the intended target area (
Reflected
The optical reflection determines what proportion of the beam will penetrate tissue. Knowledge of tissue reflectivity is important as it can reach high levels and is one of the reasons why proper eye protection is always required.
Reflection of light increases with increased angle of incidence and can be minimized by applying the incident beam perpendicular to the tissue surface.
Transmitted
When a laser beam is directed towards tissue, the resulting reflection accounts for a portion of the incident light; the rest penetrates into tissue where absorption and scattering takes place.
Scattered
As light passes into matter, the direction of the incident ray is changed by the molecules present and scattering plays an important role in the spatial distribution of absorbed energy. Increasing the diameter of the incident beam (spot size) keeps scattered photons in the beam path to the target area, increasing the energy density in the target. This means that a lower energy can be used to achieve an effective energy density at the target (Figure 8).
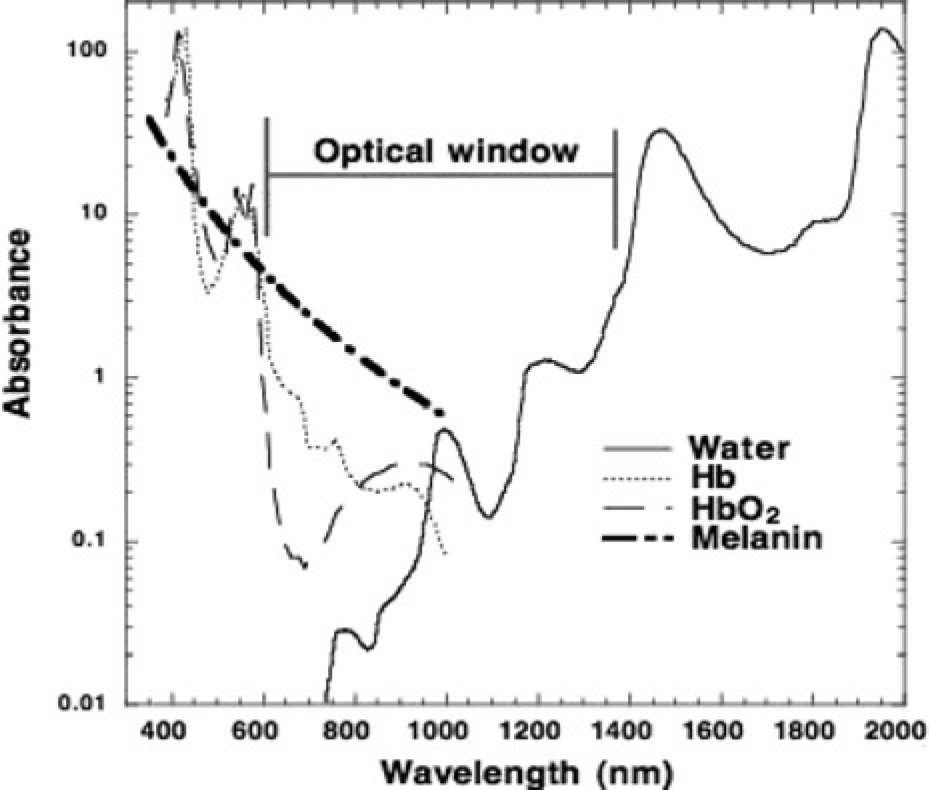
Absorption spectrum of the three main chromophores in tissues: water, haemoglobin and melanin (
Absorbed
Light absorption must take place for a biological effect to occur. The greater the degree of absorption, the greater the degree of transformation to heat. A given wavelength may be absorbed by one tissue and scattered by another. The main light absorbing components of tissue (chromophores) are haemoglobin, melanin, protein and water. In order to target a specific tissue one should select a wavelength which is strongly absorbed by a chromophore present in that tissue. Infrared light is absorbed primarily by water, while visible and UV light is primarily absorbed by haemoglobin and melanin, respectively (Figure 9).

Map of laser–tissue interaction. The circles give only a rough estimate of the associated laser parameters. Modified from reference 5
Absorption for competing chromophores can be managed by cooling the structure containing the competing chromophores to minimize collateral thermal injury.
In general as the wavelength of light increases so does the depth of penetration into skin. However, in the far infrared where water absorption dominates, the depth of penetration falls. Because of the strong absorption of water at 418, 542 and 577 nm, depth of penetration is attenuated. 4,5
Biological effects of lasers
Three types of reactions occur when laser light interacts with tissue: photothermal, photochemical and photoplasmal (Figure 9).
Photothermal
Laser light is absorbed by tissue chromophores and converted to heat, depending on the duration and peak value of the temperature achieved; different effects like coagulation, vaporization, carbonization and melting may be distinguished.
At tissue temperatures of 42–50°C (hyperthermia) bond destruction and membrane alteration occur. If hyperthermia lasts for several minutes some of the tissue will undergo necrosis.
Beyond 50°C – enzyme activity is reduced, cell immobility occurs and cell repair mechanisms are disabled.
At 60°C – denaturation of proteins and collagen occurs which leads to coagulation of tissue and necrosis of cells.
At >80°C – membrane permeability is increased.
At 100°C – water molecules start to vaporize, dehydrating tissue, gas bubbles are formed inducing mechanical cell rupture and thermal decomposition of tissue (photoablation).
At temperatures exceeding 100°C – carbonization occurs; beyond 300°C, melting can occur depending on the target material.
In general, the exact temperature for the onset of cell necrosis is difficult to determine and is dependent not only on the temperature achieved but on the duration of this temperature. Frequently not only one but several thermal effects are induced depending on laser parameters; in most applications, however, only one specific effect is aimed at (Figure 9). 4,6,7
Photochemical
At very low-power irradiation laser light induces chemical effects and reactions within tissue. The temperature increase is indiscernible. An example of this is photodynamic therapy (PDT), used in the treatment of tumours. During PDT, chromophores are injected into the body and laser light may then trigger selective photochemical reactions.
Also in the group of photochemical interactions is biostimulation. Potential anti-inflammatory and wound healing effects of extremely low laser powers (1–5 mW) is a subject of controversy. Studies show contradictory results.
Photoplasmal or photomechanical
Mechanical effects can result from either the creation of a plasma, an explosive vaporization or the phenomenon of cavitation, each of which is associated with the production of a shock wave:
With nano-second pulsed lasers, a very high-intensity pulse over a small area (between 1010 and 1012 W/cm2) ionizes atoms and creates a plasma. At the boundary of the ionized region, there is a very high pressure gradient that causes the propagation of a shock wave. It is the expansion of this shock wave that causes the destructive effect; When the exposure time of the laser is lower than the characteristic time of thermal diffusion in the tissue, it produces a thermal containment, with an accumulation of heat without diffusion and an explosive vaporization of the target occurs – this effect is produced during removal of tattoos with a Q-switched Nd:YAG laser. The large particles of pigment in the skin explode and result in smaller particles which are reabsorbed; Finally, if a mechanical containment is added to a thermal containment, the explosive vaporization does not occur, and a gas bubble is created which will implode when the laser beam is interrupted, creating the phenomenon of cavitation. This is the mechanism that is used for fragmentation of urinary calculi by a laser emitting micro-second pulses. The optical fibre is placed in contact with the stone under endoscopic control, and the mechanical containment is obtained by working under water.
4,5
Laser parameters
By the appropriate selection of wavelength, pulse duration and energy fluence, a precise biological target can be thermally damaged. 7
Wavelength
The effect of light on tissue depends on the wavelength of the light.
Light in the UV region (100–400 nm), invisible to the human eye, is known to cause erythema, hyperpigmentation and cutaneous cancer. Light energy in the visible spectrum (380–700 nm) is mostly innocuous but can be absorbed and cause thermal damage when delivered to the skin at high intensity. Light in the near-infrared (IR) region of the spectrum (780–3000 nm), invisible to the human eye, causes skin and retinal injury. 8
The degree of absorption and its thermal effect on tissue vary with the amount and type of chromophores present. Different chromophores have different absorbtion coefficients. Because laser light is monochromatic and has narrow bandwidth, it permits selective targeting of chromophores. 9
Fluence and irradiance
Irradiance is the intensity (power density) of the laser beam measured in W/cm2 and is inversely proportional to the square of the radius of spot size.

It is important to note that for a given wavelength, the larger the laser beam diameter (spot size), the deeper the penetration. The larger the spot size, the less associated the scattering and the less the loss of energy with depth of penetration. 10
Fluence
The fluence is the energy (in Joules) delivered per unit area.

Therefore, fluence is the product of irradiance and exposure time:

Pulse duration (pulse width)
The pulse width is the time during which the laser output power remains continuously above half its maximum value. By modulating a continuous-wave light source pulse duration can be altered. Pulsed laser systems may be either long-pulsed such as PDL with pulse durations ranging from 450 ms to 40 ms, or very short-pulsed (5–100 ns) such as the quality-switched lasers.
The pulse duration governs the spatial confinement of heat and should match the thermal relaxation time of the target. The thermal relaxation time is a measure of the cooling time of the target and is the time taken for the target to dissipate half of the incident thermal energy. This cooling time is primarily related to the physical size of the target: the larger the target, the longer the thermal relaxation time.
If pulse duration is equal to or less than the thermal relaxation time of the target, then unwanted heat diffusion to adjacent tissue is reduced. 11
The utilization of extended pulse durations allows the delivery of higher fluences of energy in a more gentle fashion. These greater fluences enable treatment of veins that are larger and deeper in location. In addition, the ability to deliver higher fluences in the management of lower extremity vessels has produced more consistent pan-endothelial destruction of vessels, translating into more consistent results. 12
Pulse durations recommended for 1064 Nd:YAG short enough to efficiently heat the target but long enough to provide minimal heating of the epidermis are: microvasculature: 0.3 ms; fine telangiectasia: 10–20 ms; spider veins: 20–30 ms; reticular leg veins: 40–60 ms. 13,14
Pulse repetition rate
Pulse repetition rate or pulse repetition frequency is defined as the number of emitted pulses per second (Hz).
Thermal effects depend on the type of tissue and the temperature achieved inside the tissue. Heat conduction is the mechanism by which heat is transferred to adjacent tissue structures. If the subsequent laser pulse arrives before sufficient thermal diffusion into the surrounding tissues occurs, a pronounced temperature rise and thermal damage can occur. Even ultrashort laser pulses with pulse durations shorter than 100 ps, each of them having no thermal effect, may add up to a measurable increase in temperature if applied at repetition rates higher than about 10–20 Hz. 11
Treatment principles
The main criterion in choosing pulse duration is the size of the vessels to be treated. Shorter pulse durations are best for small diameter vessels, and longer pulse durations are best for larger diameter vessels.
The deeper the blood vessel is located in the dermis, the larger the spot size, the longer the wavelength and the longer the pulse duration should be, combined with cooling to protect the epidermis. Darker skin types need longer pulses and longer pulse intervals. Stacking of pulses, rapid applications of adjacent pulses, may cause excess collateral thermal damage beyond the vasculature itself.
Practical application
There are several types of lasers used in phlebology. Older laser technologies such as continuous wave (CW) lasers of CO2 and argon have been largely replaced with quasi-CW mode lasers and pulsed laser systems. CW lasers are pumped continuously inducing a steady state of population inversion and a true continuous output. The power output per unit area is referred to as power density/irradiance (W/cm2). Pulsed lasers (flash lamp pulsed, dye lasers) emit a train of pulses and output is expressed as energy in Joules. The average power can be calculated by multiplying the pulse energy by the repetition rate.
Q switching
In Q-switched lasers a photo-optical shutter is placed within the resonating cavity, which allows turning the beam on or off very rapidly to create short pulses, in the nanoseconds domain, creating very short but very powerful pulses.
Vascular lesions
Lasers have been used successfully to treat vascular lesions, including vascular malformations and facial telangectasia. Lasers used to treat these conditions include argon, potassium-titanyl-phosphate (KTP), copper vapour, copper bromide, pulsed dye lasers (PDLs) and Nd:YAG.
The first cutaneous lasers used continuous beams of laser light. Even when wavelengths relatively specific for a particular chromophore were used, their continuous output dictated that the tissue dwell time depended on the speed of the surgeon's hand – typically long enough to cause a buildup of thermal energy that diffused to non-targeted adjacent tissue. This led to undesirable rates of adverse effects and complications (notably, scarring) that limited the use of cutaneous lasers. Pulsed laser systems, such as the 585 or 595 nm PDL, were developed and have become the mainstays of therapy for vascular lesions. These lasers offer excellent clinical improvement with a low risk of adverse sequelae. Technological improvements, such as dynamic surface cooling and extended pulse duration, enhance clinical results and minimize adverse effects.
The laser systems
In the case of vascular-specific laser systems, the intended target is intravascular oxyhaemoglobin. Although there is absorption over a broad range of wavelengths, absorption peaks for oxyhaemoglobin are in the visible range of the electromagnetic spectrum: 418, 542 and 577 nm. By targeting oxyhaemoglobin, energy is transferred to the surrounding vessel wall. Currently, the most common light devices used for vascular lesions are the 532 nm KTP, the 595 nm PDL, the 755 nm alexandrite and the 1064 nm Nd:YAG lasers and the visible/near-IR intense pulsed light (IPL) devices. 12
Argon laser
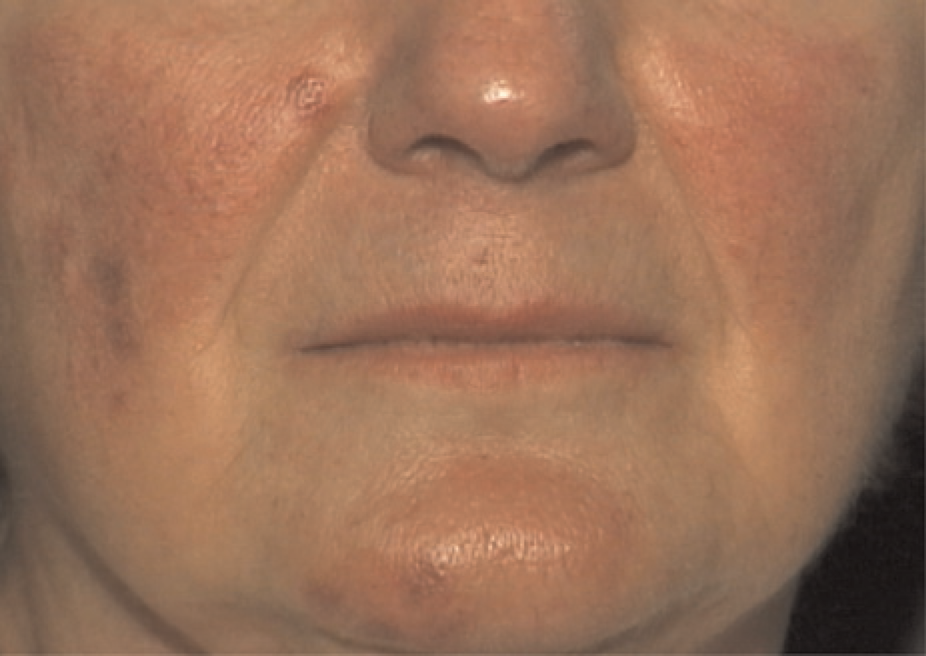
The CW argon laser was the first laser system used to treat telangiectasia (Figure 10).
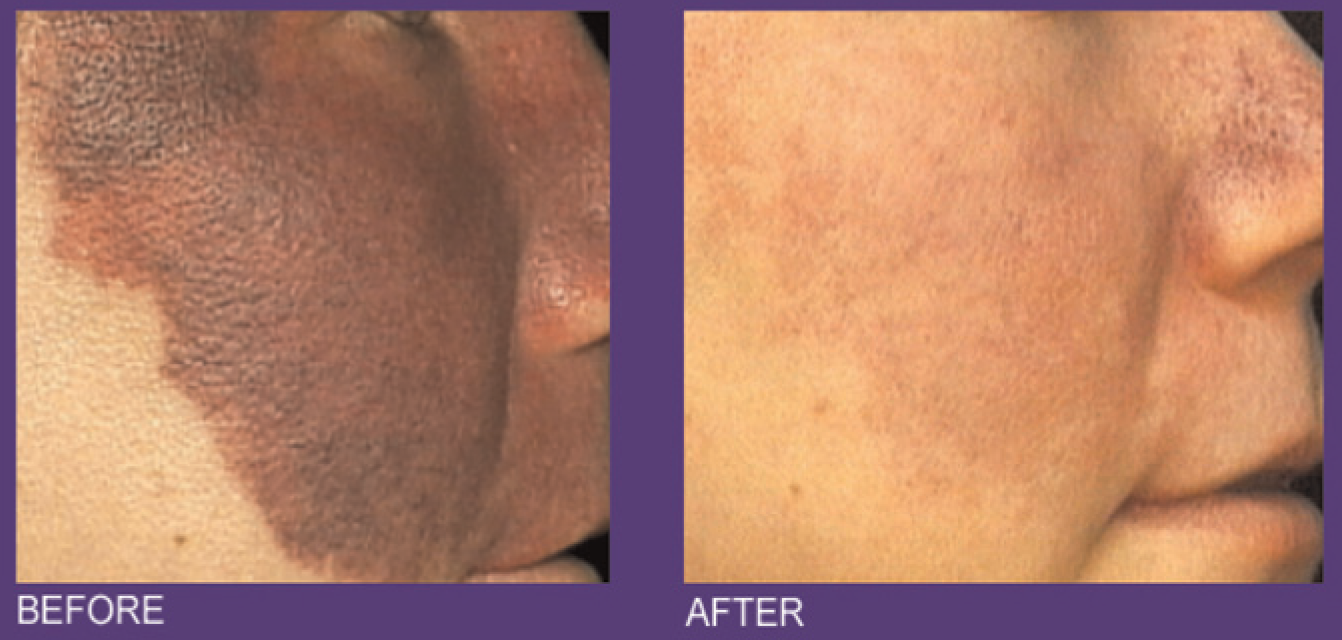
Telangiectasias on the nose and medial cheeks before and after argon-pumped tunable dye laser treatment. (
It emits blue-green light, and 80% of its emission falls within the 488–514 nm portion of the electromagnetic spectrum. Spot sizes range from 0.1 to 1 mm, reaching tissue penetration depths of 1–2 mm.
Although argon's energy is predominantly absorbed by oxyhaemoglobin, it is also absorbed to some degree by melanin because of its shorter wavelength, and it is not considered useful in darker-skinned individuals. In addition, the laser's continuous mode of operation exceeds the thermal relaxation time of the vascular target. 15 In a report of 38 patients treated by Apfelberg 16 , 49% had either poor or no results from treatment. In addition, almost half of the patients had haemosiderin bruising.
Flashlamp pumped-PDL
The traditional PDL (585 nm, 450 µs pulse duration) is highly effective in treating a variety of cutaneous vascular lesions, including PWS and facial telangectasia (Figures 11 and 12). It is less effective in the treatment of leg veins. While 585 nm light can penetrate 1.2 mm to reach the typical depth of leg telangectasia, the pulse duration is inadequate to effectively damage all but very superficial vessels, 0.1 mm in diameter or smaller. Polla et al. 17 treated 35 leg telangectasia with traditional PDL; 73% of treated vessels showed little or no response to treatment. The only lesions that responded were red-pink tiny telangectasia. Almost 50% of the treated patients developed persistent hypo- or hyperpigmentation.
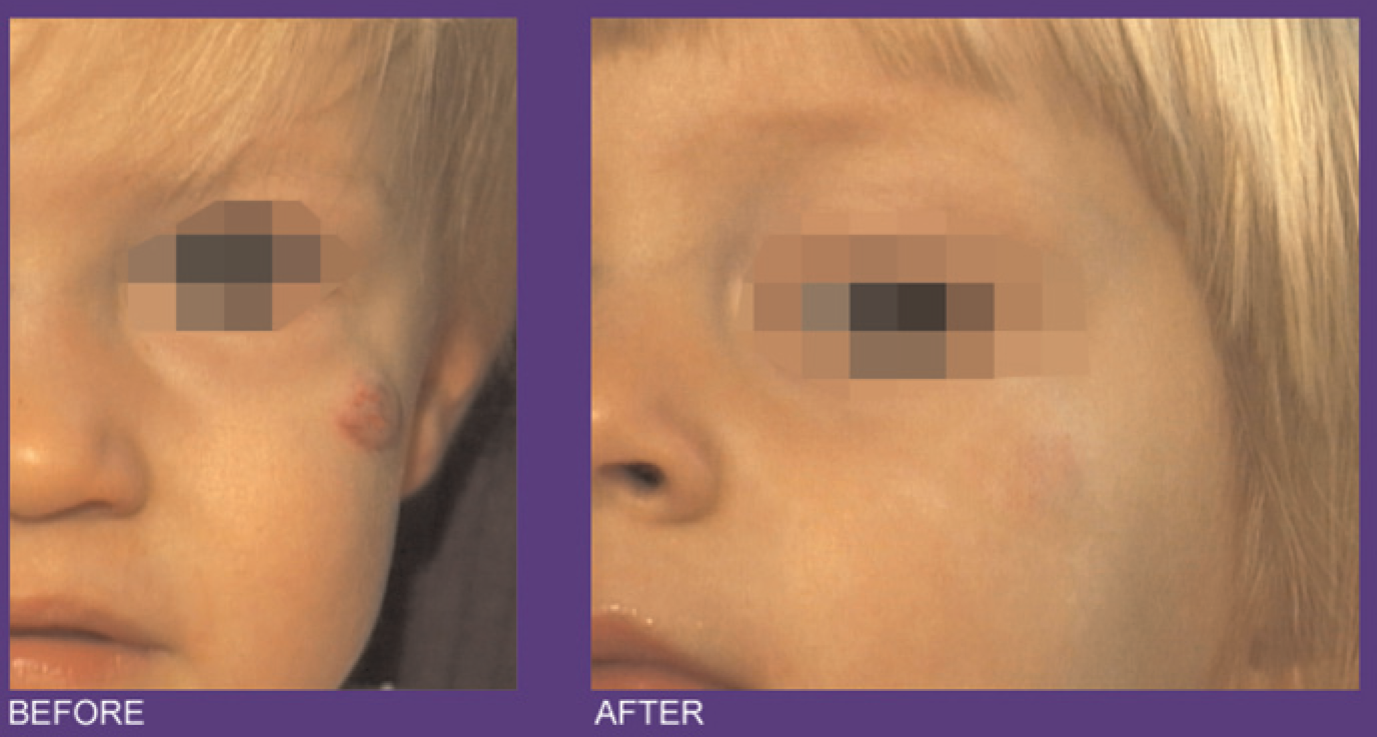
Port-wine stain on the cheek and nose with 90% improvement after nine 585 nm pulsed dye laser treatments

Haemangioma on the left cheek with clearing after three 585 nm pulsed dye laser treatments. (
KTP crystal laser
The KTP laser uses a 1064-nm Nd:YAG source passed through a KTP crystal to emit light that is frequency doubled with a wavelength of 532 nm. This quasi-CW laser system uses nanosecond pulses to destroy vascular targets. The KTP laser's 532 nm wavelength corresponds with the 542 nm absorption peak of oxyhaemoglobin, which makes it relatively specific for cutaneous blood vessels. Although the short wavelength does not allow for deep tissue penetration, extended pulse durations up to 50 ms improve its effectiveness. The KTP laser is often used to treat telangiectasia, small telangiectatic leg veins in fair-skinned patients.
For leg vessels smaller than 1 mm in diameter KTP laser requires using fluences of 12–20 J/cm2 delivered with a spot size of 3–5 mm in diameter; a train of pulses is delivered over the vessel until spasm or thrombosis occurs. Patients with darker or tanned skin have a relatively high risk of temporary hyperpigmentation or hypopigmentation. 18,19
Nathan et al. 19 treated 15 patients using a 595 nm PDL on one side of the face and a pulsed 532 nm KTP laser on the other. Both devices improved telangiectasia. The 532 nm device was at least as effective or more effective than the 595 nm laser in all subjects. On average, the KTP laser achieved 62% clearing after the first treatment and 85% clearing three weeks after the third treatment, compared with 49% and 75% for the PDL, respectively (Figure 13).

Angioma on the frontal hairline before and after several potassium titanyl phosphate laser sessions (
Copper vapour and copper bromide lasers
Copper vapour and copper bromide lasers emit yellow light with a wavelength of 578 nm. These quasi-CW mode lasers deliver rapid, 20 ns pulses at a repetition rate of 6000–15,000 pulses per second.
Facial and leg telangiectasias have been eradicated successfully with copper vapour and copper bromide systems. 20,21 A yellow light laser utilizing a copper bromide medium has shown efficacy in the treatment of red lower extremity telangiectasia of <2 mm. An average of 1.7 patient treatment sessions produced significant clearing of 75–100% in 71.8% of patients. Positive results are confined to the treatment of red vessels (1 mm). 20
Absorption of energy by melanin also occurs, making postoperative pigmentary alterations common. Thus, the use of either laser should be restricted to patients with Fitzpatrick skin phototypes I–II. 22,23
Long-pulse alexandrite lasers
Alexandrite lasers (755 nm) have been modified to allow pulse durations of up to 20 ms or longer. This wavelength theoretically penetrates to a depth of 2–3 mm. Optimal treatment parameters for long-pulse alexandrite lasers appear to be 20 J/cm2, double-pulsed at a repetition rate of 1 Hz. 24 In one study, medium-diameter vessels (0.4–1 mm) responded best and small-diameter vessels responded poorly. 25
Diode lasers
Diode lasers generate coherent monochromatic light (in the range of 800–900 nm) through excitation of small diodes. A group of 810 nm diode lasers (5–250 ms pulse duration) have been used with encouraging results in the treatment of superficial and deep small- to medium-sized leg telangiectasias.
The concept behind using near-IR wavelengths lies not only in the deeper penetration of this wavelength and in the decreased melanin absorption but also, and most importantly, in the tertiary haemoglobin absorption peak that occurs at 915 nm, for which deoxygenated haemoglobin is the target. By choosing these longer wavelengths, even deeper vessels up to 3 mm below the surface (e.g. feeder, reticular veins) can theoretically be treated, and, by varying the pulse width from a few milliseconds to several hundred milliseconds, a variety of different-sized vessels can also be targeted.
Kaudewitz et al. 26 treated 20 patients with a 940 nm diode laser, 300–350 J/cm2, 40–70 ms, 1 mm spot, single pass. At 12 months follow-up, clearing rates were greater than 75% in 15 patients (75%) and 50–75% in five patients.
The significant adverse effect of pain may limit use of this wavelength, and this characteristic of pain is shared by many of the near-IR lasers.
Nd:YAG laser (1064 nm)
The long pulsed 1064-nm Nd:YAG laser is effective for the treatment of telangiectasia, small-to-medium vessels of leg veins (up to 4 mm in diameter) and reticular veins below lower eyelids.
The advantage of the 1064-nm Nd:YAG laser over other shorter-wavelength lasers is that with equivalent absorption of blood, the 1064 nm laser has weaker melanin absorption and can penetrate deeper. It also has a high absorption coefficient of methaemoglobin and deoxyhaemoglobin, which are the main components of blue veins.
For superficial vessels less than 1 mm in diameter, the optimal parameters include small spot sizes of 2 mm, short pulse durations of 15–30 ms and high fluences of 350–600 J/cm2. For reticular veins, 1–4 mm in diameter, larger spot sizes (2–8 mm), longer pulse durations (30–60 ms) and moderate fluences (100–370 J/cm2) should yield successful results. 27 In a study of eight patients with facial telangectasia Avery et al. 28 demonstrated average mean vessel clearance of 26–50% in half of the patients and 51–75% in the other half (as evaluated by three unbiased dermatologists). Eight male patients underwent a single treatment session using a variable pulse 1.5 mm spot size Nd:YAG laser with epidermal cooling. Adverse effects are minimal and include crusting that lasts 2–3 weeks, with or without transient pigmentary alteration. 18,28
Intense pulsed non-coherent light
A non-coherent pulsed-light source that emits light within the 500–1200 nm portion of the electromagnetic spectrum can also be used to treat a variety of cutaneous vascular disorders. Depending on lesion type and size, filters of varying wavelengths (515, 550, 570, 590 nm) are used to eliminate shorter wavelengths. Light is delivered in a train of single, double or triple pulses (2–25 ms each) with varying time intervals between pulses (10–500 ms). This system is highly operator dependent and allows treatment parameters (i.e. wavelength, pulse duration, delays between pulses) to be tailored for each use.
Schroeter et al. 29 reported immediate clearing in 73.6% of patients and in 84.3% of patients after four weeks. With respect to the immediate response, 82% clearing was seen in the group with veins up to 0–2 mm, 78.9% was seen in the group from 0.2 up to 0.5 mm and 59.7% was seen in the groups from 0.5 to 1.0 mm.
The vascular application of IPL is primarily associated with the treatment of facial telangiectasia. Smaller vessels respond best to treatment with lower cut-off filters (515 or 550 nm); larger vessels require longer-wavelength filters to effect deeper tissue penetration. Because shorter-wavelength filters interact more readily with epidermal and dermal melanin, these filters should be reserved for treating fair-skinned individuals (Fitzpatrick skin phototypes I–II). Smaller vessels are usually treated with single 2.5–5 ms pulses and a fluence ranging from 25 to 45 J/cm2.
Higher energy densities (50–75 J/cm2) are used on larger vessels because the energy is administered as a train of pulses with long (40–60 ms) delays between pulses. Higher energy densities permit adequate coagulation while simultaneously protecting the overlying epidermis from excessive thermal damage. Adverse effects are mild and include transient erythema and purpura. 18,29 (Figure 14).
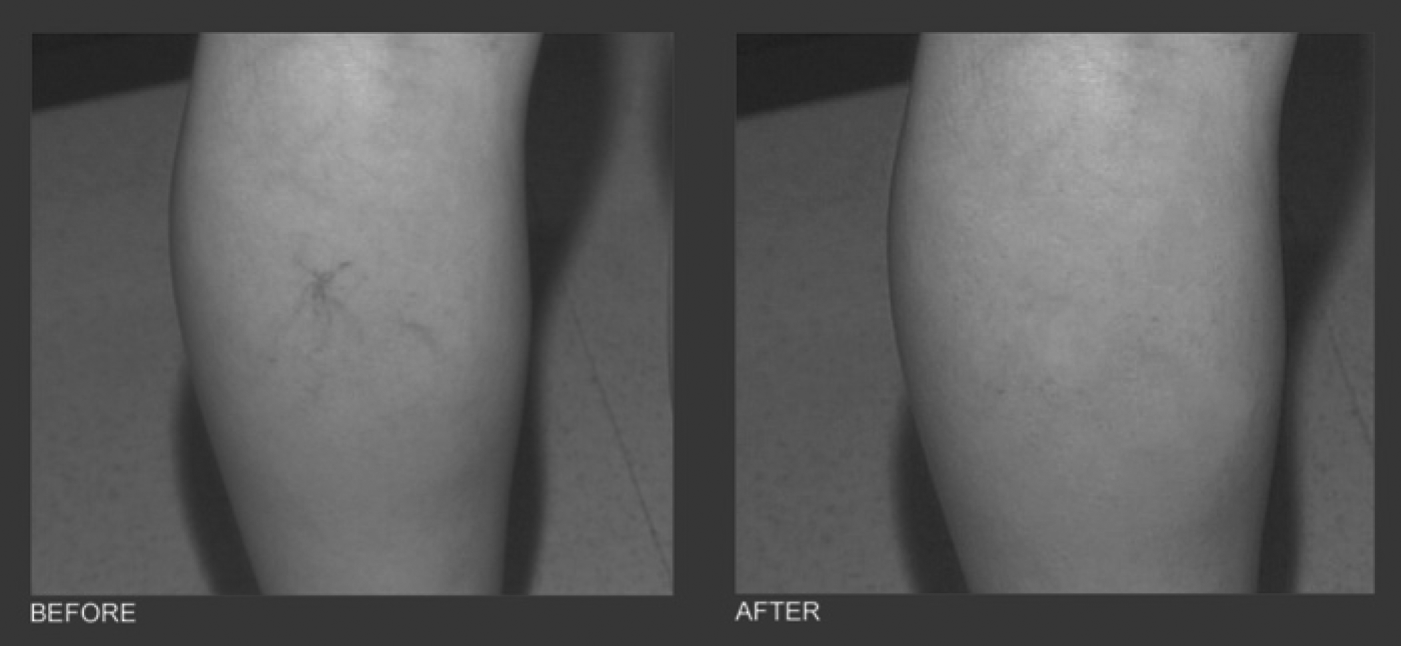
Telangectasia on the calf before and after intense pulsed-light treatment (
Treatment of different vascular lesions
Facial telangiectasias
First choice: FPDL, KTP (532 nm), IPLS.
Second choice (use with maximal care): pulsed dye laser/flashlamp pumped (APDL), argon, copper vapour.
The size and configuration of the telangiectasia will determine the optimal treatment laser. The pain associated with laser treatment of telangiectasias varies according to the laser used and the size of the area treated. Epidermal cooling can reduce the epidermal surface temperature, thereby reducing treatment discomfort and protecting the epidermis from thermal injury.
Rosacea
First choice: FPDL, KTP (532 nm), IPLS.
Second choice (use with maximal care): APDL, argon, copper vapour.
The erythema (first stadium of rosacea) can only be treated with FPDL, KTP or IPLS.
Spider angioma
First choice: KTP, FPDL, IPLS, Nd:YAG.
Second choice: argon, copper vapour.
Cherry angioma
First choice: KTP, Nd:YAG, IPLS, FPDL. 30
Leg veins and telangiectasias
In the past, the use of lasers and light sources in treating lower extremity blood vessels has not been as successful as laser treatment of facial telangiectasia. 31 Among various reasons for this partial success are increased hydrostatic pressure on the lower extremities and occasionally association with underlying venous disease.
The variation in size, blood flow, depth and type of vessel make this procedure more difficult to manage with a laser. In comparison with facial telangiectasia, leg veins have thick surrounding adventitial tissue and increased basal lamina. Lasers and IPL sources are most efficiently employed for residual vessels that do not respond to sclerotherapy, are too small to be injected or remain after feeding vessels are treated.
The longer the wavelengths (e.g. the 1064 nm Nd:YAG laser), the better the advantage of deeper penetration, the better the absorption in deoxyhaemoglobin and the greater the sparing of the epidermis. An additional benefit of the longer wavelength laser is a decreased melanin coefficient absorption.
To thermocoagulate leg veins of deeper location and of greater diameter, the laser systems should be able to deliver very high-energy pulses through large spot sizes to enhance scattering into dermis. Pulse duration has been demonstrated to be in the millisecond domain for intradermal vessel treatment. The longer pulse duration is closer to the thermal relaxation time of larger vessels (1–50 ms), thus being able to target larger diameter vessels (0.1–2 mm), including leg telangiectasia. 31 Over the last few years, Nd:YAG laser systems have became the lasers of choice for leg vein treatment.
Other choices
For isolated, relatively small diameter (<1 mm) leg telangiectasias: KTP, FPDL (long pulse), IPL. For larger diameter, moderately deep leg vessels: alexandrite, diode, IPL. 30
Laser complications
Ocular complications
These may occur via direct or indirect ocular exposure to laser irradiation. Potential damage is wavelength specific. Wavelength-specific eyewear must be worn by both operators and patients.
Fire and electric shock
With high enough energy and absorption, laser beams can ignite clothing, hair or paper products. The risk increases in the presence of oxygen and methane. Precautions (e.g. removing or protecting hair and clothing within the treatment areas) must be taken to prevent this. Electric shock due to the high voltage required by lasers can also occur. Proper wiring during installation is critical. 32
Dermal complications
Pain
The snapping and burning sensation of each laser pulse can produce a minimal to moderate amount of discomfort. An anaesthetic cream or injection can be used to block the pain. However, pain is an important marker of possible side-effects occurring (Figures 15 and 16).
Purpura immediately after pulsed dye laser treatment of facial telangiectasias (

Hypopigmented scar within a port-wine stain after test treatment with a continuous-wave argon laser (
Purpura, bruising
Immediately after the laser treatment the area will in some cases appear grey or blue-black in colour. The discolouration will fade over the next 7–10 days.
Bleeding, haematoma and disruption can be caused by inadequate treatment parameters (e.g. pulse duration too short combined with fluences that are too high).
Swelling
Within a few minutes after the laser treatment, an erythema and oedema will occur over the treatment area. Areas most likely to swell are under the eyes and the neck. The swelling subsides within 3–5 days if ice is regularly applied. Parallel and post-cooling will diminish the amount of oedema.
Discolouration, blisters or scabs
Develop rarely (mostly caused by overtreatment).
Grey or pale white discolouration of the epidermis is a sign of early dermal damage indicating inappropriately high fluences. This sign will last only a few seconds.
Blister formation, epidermal disruption and epidermis necrosis (and dermis necrosis in severe cases) will follow. Intense cooling, reduction of the fluence and prolongation of the pulse duration are consequent reactions.
Infection
Increasing (instead of decreasing) swelling, redness, crusting, pain and fever can be an indication for an infection. Topical antiseptics or oral antibiotics should be used.
Reactivation of herpes simplex
On the face (when the face is treated) or genitals (when legs are treated).
Preventive oral virostatic therapy (acyclovir, valcyclovir, famcyclovir) is recommended when the patient has frequent herpetic episodes (more than six per year), starting the day before laser treatment.
Skin darkening (hyperpigmentation)
This reaction is more common in patients with darker skin types (Fitzpatrick III–V). The darkening worsens if the laser-treated area is exposed to the sun. Eventually fades within 2–6 months.
Skin lightening (hypopigmentation)
Mostly caused by overtreatment. Pale areas usually darken or repigment within 3–6 months. Could be persistent.
Scarring
Mostly caused by overtreatment. Occur when either excessive fluences or overlapping laser spots are used. 30,32
Endovenous laser ablation
EVLA is a new minimally invasive treatment for varicose veins employing laser ablation of the incompetent truncal vein under tumescent local anaesthesia. Laser energy is delivered to the desired incompetent segment inside the vein through a laser 400–1000 µm, bare-tipped laser fibre. A variety of wavelengths are in use for this procedure, including 810, 940, 980, 1064 and 1320 nm. The main chromophore of 1320 nm lasers, at least initially, is water while other wavelengths target haemoglobin.
When the laser is fired, it deposits thermal energy into the blood and venous tissues, causing irreversible localized tissue damage. The laser is most commonly delivered continuously as the laser fibre is withdrawn along the vein. 33,34
For treatment using CW delivery, the energy delivery is set to 12–14 J/s (12–14 W) and the laser fibre is withdrawn at a steady rate of approximately 1 mm/s. 18,33
Despite the clinical efficacy of EVLA, its mode of action is incompletely understood.
Vein wall injury has been postulated to be mediated both by direct effect and indirectly via laser-induced steam generated by heating small amounts of blood within the vein. It was reported by Proebstle et al. 35 that intravascular blood plays a key role for this homogeneously distributed thermal damage to the inner vein wall during EVLA. Histopathological studies showed that in saline-filled veins, EVLA-induced vessel wall injury was confined to the site of direct laser impact. In contrast, blood-filled veins exhibited thermal damage in more remote areas including the vein wall opposite to the laser impact. Laser energy from different diode lasers (810, 940 and 980 nm) generated steam bubbles in haemolytic blood, while no bubbles could be produced in normal saline or plasma.
Others believe that the combined effects of vein spasm, compression by perivenous tumescent anaesthesia and ablation in the Trendelenberg position results in an ‘empty’ vein and direct thermal damage to the vein wall. This is supported by several histological studies that show intimal damage combined with discrete full thickness perforations and relatively ‘normal’ intervening veins. 36,37 The likely mechanism of action in EVLA involves initial energy absorbtion by the small amount of residual blood (the chromophore) in the target vein and this sets off a sequence of events that leads to carbonization along the vein wall. 36–38
Special consideration must be given to EVLA with a 1320 nm Nd:YAG laser and 1470 nm diode laser. At this wavelength, the dominant chromophore is water, and the absorption is limited to water that is present in the endothelial cells. As biological tissue is mostly composed of water, deeper penetration and thermal effect can be achieved at lower power settings, typically 5 W.
This technique has not been complicated by postoperative pain or ecchymosis, as occurs with lower laser wavelengths used for intravascular treatment of the great saphenous vein (GSV). 39,40
Fluence
The ‘dose’ of laser energy delivered can be expressed as joules (J)/cm vein, sometimes called linear endovenous energy density or as fluence, which is laser energy delivered for a given surface area (J/cm2). Optimum occlusion rates are achieved with a minimum laser energy of >60 J/cm (810 diode laser [pulsed] at 12 W power). 37,41,42
Lasers using water-specific wavelengths (1320 nm, 1470 nm) allows the use of a lower laser fluence. 39,40,43
Major complications following EVLA are rare and studies report rates of deep vein thrombosis <1%, parasthesia 2% and skin burns 0.4%. 18,34,44 Pain, haematoma and phlebitis are common adverse events associated with endovenous laser therapy, but in most cases are self-limiting.
EVLA has a successful closure rate of 95–100%. The outcomes appear durable with a persistent closure rate of 95–100% 33,34,44,45 (Figure 17).

One week after EVLA with 810 nm diode laser (
Training and qualification
While current guidelines on appropriate cutaneous laser training and delegation are not detailed and comprehensive, some recommendations occur repeatedly in guidelines proposed by various national professional organizations. In particular, it is apparent that:
Optimal laser use occurs when a physician who is trained in a relevant specialty, with additional training for the specific laser to be used, directly performs laser services on an appropriately selected patient; Laser training of non-physician providers should be comprehensive and not limited to merely delivering a technical service, but should include theoretical and practical training, and should encompass an understanding of patient selection, adverse events and appreciation of the limits of this training; Even when non-physician personnel are appropriately trained, delegation of laser use should occur in the context of adequate physician oversight under ideally direct, on-site supervision.
46
Compliance with these recommendations is not universally mandated in legislation and state laws are now needed to address this new technology.
Setting up a laser practice use
The decision to use medical lasers in a health-care facility should be followed by a commitment to establish a viable Laser Safety Program for the institution. Policies and procedures for laser safety should be developed with regard to individual practice settings, acceptable standards and state regulations.
All persons should be aware of area of use and controlled access to these areas must be maintained.
The nominal hazard zone (NHZ) should be identified to prevent unintentional exposure to laser beam; The NHZ should be occupied by authorized personnel; Personnel in the NHZ should be aware of all laser safety precautions; Regulation laser signs should be placed in all entrances to warn on-lookers of potential hazard; Doors in the NHZ should remain closed and windows and reflective services covered.
Everyone in the NHZ should wear appropriate eyewear approved by Laser Safety Officer (LSO). The protective eyewear should be appropriate to wavelength used and labelled with appropriate optical density.
Patients' eyes and eyelids should be protected by wet eyepads, laser protective eyewear, eye shields, etc.
All persons in laser treatment area should be protected from laser beam exposures to their skin and other non-targeted tissues. Exposed tissues around the operative site should be protected with saline-saturated fire/flame retardant materials.
Anodized, dull, non-reflective or matte-finished instruments should be near the laser site. All persons in laser treatment area should be protected from flammability hazards associated with laser usage.
Fire is one of the significant hazards of laser use. The intense heat of laser beams can ignite combustible/flammable solids, liquids and gases. Free flow of high oxygen can lead to rapid spread of flames. Appropriate fire extinguishers and water/saline should be immediately available.
All personnel should be protected from electrical hazards associated with laser use.
Visual inspection of laser equipment should be done after setup for use. Laser service and preventive maintenance should be documented. A LSO should review records and approve equipment use after service.
Personnel working in the NHZ should demonstrate competency commensurate with their responsibilities. Education and training programmes should be specific to laser systems and procedure used in the facility. 47
Conclusion
Facial telangiectasias are a common source of cosmetic concern for patients. Many light-based modalities have proven effective in their treatment, including KTP, PDLs, Nd:YAG lasers, as well as IPL. 18,48,49,50
The role of lasers in treating lower-extremity blood vessels has not been as successful as in treatment of facial telangiectasia to date. There are several reasons for this disparity. Increased hydrostatic pressure on the lower extremities may lead to less effective photothermal destructive coagulation. Anatomic considerations are also important, in that lower extremity blood vessels are in a deeper location, have thick surrounding adventitial tissue and increased basal lamina as compared with facial telangiectasia.
Although laser technology continues to evolve and improve, optimal results for leg telangiectasias may often be achieved with sclerotherapy or sclerotherapy followed by laser or IPL therapy for small, difficult-to-cannulize vessels. 31
There have been several large case series describing outcomes for EVLA. Most report GSV ablation rates of over 90%, with associated improvement in symptoms.
Lasers with wavelengths from 808 to 1320 nm have been used for EVLA. New developments in laser technology are currently being assessed. In particular, a 1470 nm diode laser (absorption wavelength of water) has recently become available.
Available data indicate that optimum occlusion rates are achieved with minimum laser energy of 60 J/cm. 42
However, there seems to be no consensus as to the optimum treatment protocol for EVLA. The literature describes considerable variation not only in the laser system used but also in patient selection, adjunctive procedures used (phlebectomies or sclerotherapy [foam or liquid]), compression following treatment, thromboprophylaxis, analgesia, anaesthesia and patient follow-up.
Standardization of EVLA technique, continued evaluation of different laser systems and their mode of action, and of course long-term follow-up are needed to further define the role of endovenous laser.