
Abstract
Objectives
The relationship between venous thrombosis (VT) and atherosclerosis is controversial in recent studies. Aortic elastic properties have a predictive value in detecting early stages of atherosclerosis. The aim of this study is to evaluate the relationship between aortic elastic properties and VT.
Methods
Elastic properties of aorta in patients with spontaneous VT, without history of known cardiovascular disease and cardiovascular risk factors (n: 31), and in healthy subjects without cardiovascular risk factors (n: 30) were compared. Elastic properties of the aorta were assessed with transthoracic echocardiography.
Results
A significant increase in aortic stiffness index (6.5 ± 1.0 versus 6 ± 0.7, P = 0.03) and a significant decrease in aortic strain and aortic distensibility were found in patients with VT compared with healthy subjects (8.4 ± 7 versus 13 ± 8, P = 0.01, 4.9 ± 4.8 versus 6.5 ± 4.4, P = 0.03, respectively).
Conclusions
Elastic properties of aorta in patients with spontaneous VT were impaired. These results may support the role of endothelial dysfunction in the pathogenesis of VT.
Introduction
Although venous thromboembolism and cardiovascular disease are commonly classified as two different disorders, the relationship between venous thrombosis (VT) and atherosclerosis is controversial in recent studies. 1–5 While there is a substantial improvement in the treatment and diagnosis of VT, its pathogenesis is still obscure. Inflammation and thrombosis are interrelated. It is shown that inflammation increases tissue factors, platelet reactivity and fibrinogen while decreasing thrombomodulin and inhibiting fibrinolysis. 6 In the literature, there are studies showing the relationship between VT and inflammation. 7–9 Systemic inflammation is also an important factor in the initiation and progression of atherosclerosis. 10 Atherosclerosis is associated with activation of both platelets and blood coagulation as well as an increase in fibrin turnover, which can lead to thrombotic complications. 11
In recent years, association with aortic elastic parameters (aortic stiffness index, aortic strain and aortic distensibility) and cardiovascular diseases has been evaluated. 12 Aortic stiffness is defined as the arterial rigidity caused by the loss of elastic tissue in the arterial wall that decreases the widening capacity of the artery. Damage to the arterial wall due to inflammation and atherosclerosis causes a decrease in arterial distensibility, compliance and elasticity. 13 Furthermore, non-invasive assessment of elastic properties of the aorta has a predictive value in the determination of atherosclerosis at early stages. 12 This study aimed to investigate association with atherosclerosis and VT by evaluating aortic elastic properties in patients with VT.
Methods
Study populations
Elastic properties of the aorta in patients with spontaneous VT, presented with pain or swelling in the leg, and documented thrombosis with venous Doppler ultrasonography without any history of cardiovascular disease and cardiovascular risk factors (n: 31; 16 M, 15 F) were compared with healthy subjects without any cardiovascular risk factors (n: 30; 17 M, 13 F). Elastic properties of the aorta were assessed with transthoracic echocardiography. Routine biochemical analysis, body mass indexes (BMIs) and waist circumferences were measured and left ventricular mass (LVM) was calculated.
Exclusion criteria
Exclusion criteria were determined as follows: secondary VT (cancer, pregnancy, leg trauma, immobilization for more than 1 week or current users of oral estrogen with or without concomitant progestin use), resting blood pressure >140/90 mmHg or those taking antihypertensive medications, diabetes mellitus, statin use, smoking, heart valve disease, atrial fibrillation, left ventricular (LV) systolic dysfunction, heart failure, renal disease, aortic disease such as aneurysm, previous aortic surgery, congenital heart disease and insufficient echocardiographic evaluation due to poor echocardiographic windows. Informed consent was given by all participants and the local ethics committee approved the study protocol.
Echocardiographic measurements
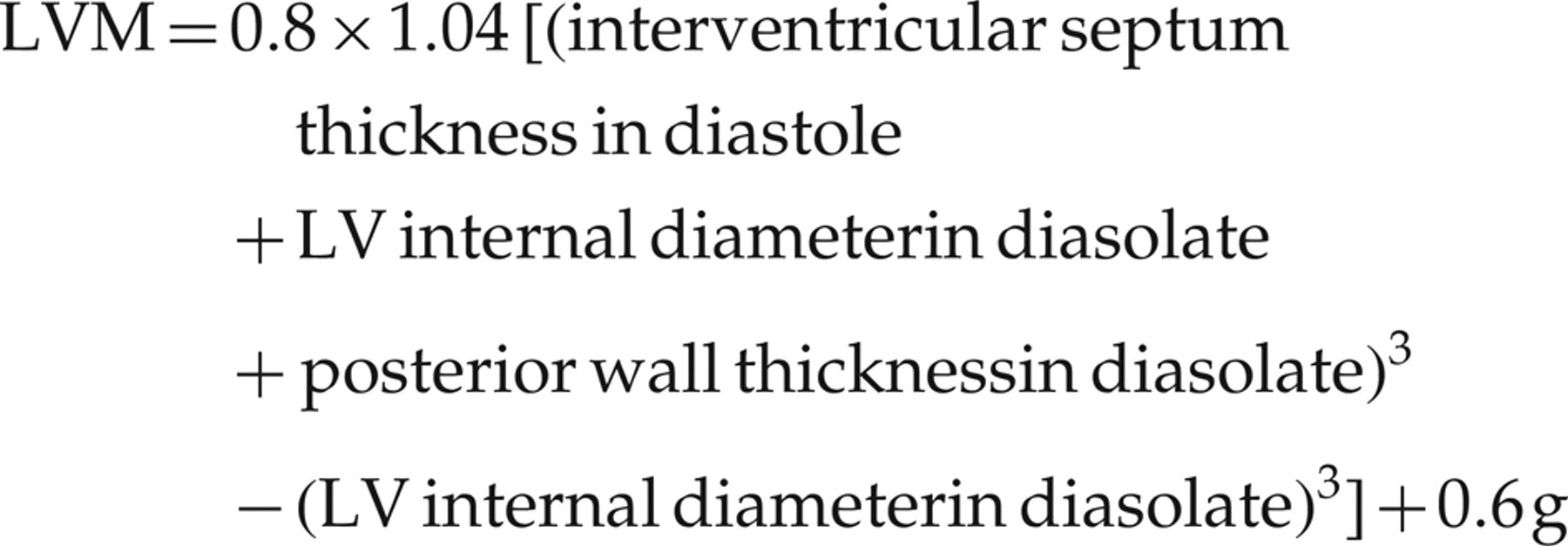
Transthoracic echocardiography was performed by an experienced echocardiographer, using a System-Five Performance instrument (General Electric, Vingmed, Norway) with a 2.5 MHz phased-array transducer. Recordings were taken with patients positioned in the left lateral decubitus position. The M-mode traces were recorded at a speed of 50 mm/second and the Doppler signals were also recorded at a speed of 100 mm/second. M-mode echocardiographic measurements were obtained based on the standards of the American Society of Echocardiography. 14 Left atrial diameter, LV end-systolic and end-diastolic diameters, end-diastolic interventricular septal thickness and end-diastolic LV posterior wall thickness were measured. LV ejection fraction was determined by the Teichholz method. 15
The LVM was calculated using the Devereux formula
16
:
Blood pressure measurements
Blood pressure measurements used in the study were taken with a mercury sphygmomanometer at the time of echocardiography. Korotkoff phases I and V were used to determine the systolic and diastolic pressure, respectively, and at least three consecutive measurements were obtained and the results were averaged.
Calculation of the elastic parameters of the aorta
The diameter of the ascending aorta was measured from the same view on the M-mode tracing at 3 cm above the aortic valve. The systolic diameter was measured at the maximal anterior motion of the aorta, whereas the diastolic diameter was measured at the peak of the QRS complex on the simultaneously recorded electrocardiogram. As the reviewer mentioned, echocardiographic measurements were made according to the average of three consecutive measurements. The aortic stiffness index, aortic distensibility and aortic strain were determined as aortic elasticity properties.
The formulas used in the calculation of these parameters were as follows:
17–20
Aortic stiffness index = ln (systolic pressure/diastolic pressure)/aortic strain; Aortic strain (%) = (aortic systolic diameter − diastolic diameter) × 100/diastolic diameter; Aort distensibility (cm2/dyn) = (2 × aortic strain)/(systolic pressure − diastolic pressure).
BMI and waist measurement
BMI was calculated by dividing body weight (in kg) by the square of body height (in m). Waist circumference was measured at the midpoint between the bottom of the rib cage and the top of the iliac crest from patients at minimal respirations.
Biochemical analysis
Fasting blood samples were obtained from all subjects and serum glucose, total cholesterol, triglyceride, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) levels were immediately measured by an autoanalyser (Beckman Coulter, Syncron LX20PRO, Brea, CA, USA).
Statistical analysis
Statistical analysis was performed with SPSS for Windows version 10.0 (SPSS Inc, Chicago, IL, USA). Data are presented as mean ± SD. For continuous variables, the Mann-Whitney U test was used and for categorical changes, the chi-square test was used.
Relationships between various variables were examined with Pearson correlation coefficients. A P value <0.05 was considered as statistically significant.
Results
Baseline demographical and biochemical properties were similar in both groups (Table 1). A significant increase in aortic stiffness index (6.5 ± 1 versus 6 ± 0.7, P = 0.03) and a decrease in aortic strain and aortic distensibility were established in VT patients compared with the control group (8.4 ± 7 versus 13 ± 8, P = 0.01, 4.9 ± 4.8 versus 6.5 ± 4.4, P = 0.03, respectively) (Table 2). LV septum and posterior wall thickness of VT patients were higher than those of the control group (1 ± 0.2 versus 0.9 ± 0.2, P = 0.003, 1 ± 0.1 versus 0.8 ± 0.1, P < 0.001 respectively). The LVM of these patients were also higher than those of the control group (152 ± 46 versus 118 ± 39, P = 0.007). Transthoracic echocardiographic parameters and aortic elastic properties are shown in Table 2. While a positive correlation between age (r = 0.36, P = 0.005), waist circumference (r = 0.30, P = 0.02) and LVM (r = 0.35, P = 0.008) with aortic stiffness index was detected in patients with VT, there was a negative correlation between aortic distensibility and these parameters (age: r = −0.39, P = 0.003; waist circumference: r = −0.28, P = 0.03; LVM: r = −0.2.8, P = 0.03, respectively) (Table 3).
Baseline demographical and biochemical properties in both groups
NS = not significant; BMI = body mass index; SBP = systolic blood pressure; DBP = diastolic blood pressure; TC = total cholesterol; LDL = low-density lipoprotein-cholesterol; TG = triglycerides; HDL = high-density lipoprotein-cholesterol
Comparison of transthorasic echocardiographic parameters and aortic elastic properties in both groups
LA = left atrial diameter; EF = ejection fraction; LV = left ventricular
Correlation between aortic elastic properties and other parameters
WC = waist circumference; LA = left atrial diameter; LVSD = LV systolic diameter; LVDD = LV diastolic diameter; EF = ejection fraction; LVM = LV mass; BMI = body mass index; SBP = systolic blood pressure; DBP = diastolic blood pressure; TC = total cholesterol; LDL = low-density lipoprotein-cholesterol; TG = triglycerides; HDL = high-density lipoprotein-cholesterol
Discussion
Impairment of elastic properties of aorta in patients with VT is established in this study. The principal findings of this study are as follows: (1) Increase in aortic stiffness, decrease in aortic strain and distensibility in patients with VT compared with the control group; (2) significant increase in LVM in patients with VT; and (3) a positive correlation between LVM, age and waist circumference in patients with aortic stiffness but a negative correlation with aortic distensibility in patients with VT.
Stasis, damage to the vessel wall and hypercoagulability, known as Virchow's triad, are responsible for the pathogenesis of the VT. 21 However, in about a third of patients with VT, the cause of the disorder is unexplained. Several factors other than Virchow's triad have been studied especially in the pathogenesis of idiopathic VT, and inflammation is a highlighted topic in the pathogenesis of VT. The role of inflammation in the pathogenesis of VT is established in several studies. 7–9 Inflammation is associated with neutrophil infiltration into the vessel wall and the cytokine tumour necrosis factor-alpha, chemokines and adhesion molecules were shown to be associated with thrombogenic process. 7 Furthermore, inflammation mediates a key role in the pathogenesis of atherosclerosis 6 and causes an increase in arterial stiffness through deteriorating vascular function. 22,23 Atherosclerosis, like inflammation, potentiates a risk for procoagulant state. 24,25
Although according to the concept that VT and atherosclerosis are two completely distinct entities, increased cardiovascular events in patients with VT were reported. Recent studies support the relationship between atherosclerosis and VT, but it is still controversial. Atherosclerosis was reported to be a potential risk factor in the pathogenesis of VT. 3 According to another scenario, these two distinct pathological conditions are simultaneously triggered by the same biological stimuli that are responsible for activating coagulation and inflammatory pathways in both arterial and venous system. Non-invasive ultrasound techniques are widely used to evaluate the vascular system and assess cardiovascular function. In order to evaluate the relationship between VT and endothelial dysfunction, carotid arteries were evaluated with Doppler ultrasonography in patients with spontaneous VT without cardiovascular disease by Prandoni et al. 4 , and the prevalence of carotid plaques were significantly higher in patients with spontaneous VT.
However, another study, designed with the same method, did not reveal a significant relationship between VT and atherosclerosis. 2 Finally, recent studies have shown that the use of statin reduces the risk of VT, but non-statin lipid-lowering agents did not show the same effect. 26 Interestingly, the improvement in aortic stiffness related with regression of atherosclerosis by long-term statin usage was reported. 27 Regulatory effect of statins on endothelial function was concluded to be the possible mechanism for these results.
In this study, we evaluated the endothelial function in patients with VT with aortic elastic properties as a non-invasive measurement method. Aortic elastic properties in patients with VT have never been studied before. In order to eliminate the negative effects of cardiovascular risk factors on aortic compliance, patients with cardiovascular risk factors were excluded and demographical properties of both groups were similar. The relationship between increase in aortic stiffness and cardiovascular mortality and morbidity has been shown in recent studies. 28,29 Furthermore, a close relationship between increased arterial stiffness and atherosclerosis has been reported. 30 Evaluation of elastic properties of aorta has an important role in the early diagnosis of atherosclerosis and an increase in arterial stiffness could be an early predictor of coronary artery disease. 12 In conclusion, an increase in aortic stiffness in this study may support the role of inflammation and endothelial dysfunction in the pathogenesis of VT.
Relationship between age, hypertension, diabetes and abdominal fat with aortic stiffness is a well-known issue. 31,32 In this study, although a positive correlation between age and waist circumference with aortic stiffness index was detected, there was a negative correlation with aortic distensibility. Although a significant correlation between aortic stiffness and waist circumference, a measure of abdominal obesity, was reported in former studies, the same correlation was not detected with BMI, a measure of obesity, as in this study. 32 Physiopathology that links abdominal adiposity to stiffening is still unknown. In abdominal obesity, especially visceral fat tissue has a role in the secretion of bioactive substances like inflammatory proteins and leptin. Indeed, high levels of leptin have been documented in individuals with obesity and found to be correlated with reduction in arterial distensibility. 33 We detected significant increase in LVM in patients with VT and there was a positive correlation between LVM and aortic stiffness index. Although hypertensive patients were excluded in this study, a significant increase in LVM may be related to an increase in aortic stiffness. Increase in aortic stiffness was reported to be associated with LV concentric remodelling in both hypertensive and normotensive population. 34
Limitations
Biochemical markers showing endothelial dysfunction and inflammation were not studied in this study. Although deterioration of aortic elastic properties in patients with VT supports the role of endothelial dysfunction in this study, it must be reinforced with different methods. Although the study groups were small, they are quite homogeneous. We took great care to exclude subjects with known cardiovascular disease and/or risk factors.
Conclusion
In this study, we revealed deterioration of elastic properties of aorta in patients with spontaneous VT. These findings may support the role of inflammation and endothelial dysfunction in the pathogenesis of VT. In conclusion, showing the role of endothelial dysfunction in the pathogenesis of VT may open a new horizon for different treatment modalities; hence prospective studies should further investigate the underlying mechanism of this relationship.