
Abstract
Objective
We present two cases of a unilateral leg swelling of unusual aetiology as a reminder to the physician to consider causes of unilateral leg swelling other than deep vein thrombosis, lymphoedema and infectious diseases.
Case reports
Both of our patients developed progressive leg swelling. Subsequent investigation revealed a lesion compressing the femoral vein. At exploration this was found to be a ganglion cyst. In one patient surgical removal of the cyst and in the other puncture of the cyst and instillation of steroid resulted in prompt resolution of the swelling.
Conclusion
Venous compression due to external cystic lesions, although rare, is recognized. In strange cases this differential diagnosis should also be taken into account. Therapeutic options are the surgical removal or puncture of the cyst.
Keywords
Introduction
Unilateral leg swelling is a common presentation to the specialized physician and to the vascular surgeon. Common causes include chronic venous insufficiency, lymphoedema and, more acutely, infectious diseases and deep vein thrombosis (DVT).
Leg swelling because of venous insufficiency appears over a time period of months or even years. Patients’ history often shows a previous deep venous thrombosis or a longstanding insufficiency of superficial veins. A pimary or secondary lymphoedema is presenting with a painless, initially smooth swelling, including foot and toes. Lymphoedema is frequently seen after minor trauma or infection of the interstitium. Recurrent infections with bacteria (Streptococcus, Staphylococcus) worsen the oedema eventually until elephantiasis.
DVT affects the deep leg venous system and leads to a more acute onset of the unilateral swelling. Oedema of the entire leg and a feeling of tension are the most common clinical signs of an acute DVT of the leg. The annual incidence of DVT is about 1–2/1000 of overall population, but rarely occurs in children. 1 The Wells score was introduced as a clinical probability tool to estimate the risk for a thrombosis (Table 1). 2 The most commonly used tests for the diagnosis of DVT are venous compression ultrasound (CUS) and D-dimers.
Wells clinical probability tool
Each positive response is 1 point, except if an alternative diagnosis is as likely as or greater than DVT, where 2 points are deducted. 0 or fewer points: low probability; 1–2 points: moderate probability; 3 or more points: high probability
However, rarer causes of unilateral leg swelling should not be forgotten. Extrinsic vein compression by tumours or lymphatic nodes is simulating the clinical signs of thrombosis as well as some typical signs in duplex ultrasound. Dilated deep femoral and popliteal veins, and cessation of blood flow tend to result in the wrong diagnosis. Only compressibility of the deep veins may confirm the absence of a DVT. By chronic friction of the iliopsoas muscle in its relation to the pecten ossis pubis an inflammatory enlargement of the corresponding bursa ileopectinea can lead to a compression of the common femoral vein. We report two unusual cases of extrinsic femoral vein compression secondary to such ganglion cyst.
Case report 1
A 74-year-old woman came to our department because of recurrent swelling of the left leg for 2–3 months. Under compression stocking and acetylsalicylamide (Aspirin®) the discomfort of the patient improved for some weeks. After a four-hour walk she complained about a huge swelling of the left leg with little pain. No history of thrombosis is reported. Further she suffered from spinal cord stenosis. With the strong suspicion of a DVT we began further investigations.
Characteristics of the patients
On clinical presentation we saw a distinct swelling of the left leg. Except of diffusely distributed purple telangiectasias, the patient had no clinical signs of venous insufficiency and no accessory truncal varicose veins were found. No clinical signs of phlebitis could be found. Hohman's and Payr signs were negative.
In CUS investigation of the right side we found all superficial and deep veins with normal compressibility and flow variability corresponding with the respiration and the arterial pulsations.
In contrast on the left side the femoral and popliteal deep vein system showed a continuous slow venous flow. Although the examination of the deep vein segments cleared out a normal compressibility, the red cell aggregates could hardly be moved upwards by distal compression of the calf muscles. No flow variation could be registrated neither according to respiration nor to arterial pulsations. No evidence could be found for venous reflux under provocation.
Subsequent computer tomography of the pelvis demonstrated a low attenuation lesion posteromedial to the common femoral artery, displacing the artery ventrally and compressing the common femoral vein. The lesion was defined as highly suspicious to be an enlarged bursa iliopectinea. More detailed clinical examination revealed that an ill-defined swelling was palpable just below the medial half of the inguinal ligament.
On the basis of these findings, the left groin was surgically explored. Intraoperatively a cyst posterior to the common femoral vein and artery was found. Surgical decompression and cyst removal lead to an improvement of the venous flow and also to a resolution of the swelling. Histology showed a cyst wall composed of fibrous connective tissue and devoid of an epithelial lining (pseudocyst), consistent with an iliopectineal eminence.
Case report 2
A 91-year-old woman presented with right leg swelling of recent onset. She claimed about tenseness without pain. Her medical history included chronic back pain after spondylodesis of L4/S1 and known bilateral varicose veins. On clinical view unchanged grotesque swelling of the right leg with an unsharp demarkated erythema came across. Groin polycyclic tumour mass was palpable. Her regular medication consisted of acetylsalicylamide 100 mg/day as well as zaleplone (a hypnoticum). The clinical investigation of both legs in the standing position showed morphological clearly different leg silhouettes and a livide discoloration of the right leg, no temperature differences were observed (Figure 1).

A 92-year-old lady with a swollen right leg and larger circumference in contrast to the left
In CUS of the right leg, subligamentary region the femoral vein had a standing not breathtone modulated flow. Behind the inguinal ligament a hypoechoic fluidlike tumour mass was compressing the femoral vein. Distally to this mass the deep veins of the groin and crural region, as well as the superficial venous system, were fully compressible. Valsalva manoeuvre and peripheral decompression of the calf muscles showed no reflux. Initially the patient was not compliant to take part in further clarifying investigations to define the cause of obstruction in the groin region. In the mean time we treated with compression bandages and low molecular heparin to avoid thrombogenesis. Subsequent investigation after a delay of two weeks with computer tomography revealed a bursa iliopectinea with an axial diameter of 47 × 31 mm and a coronar diameter of 36 × 90 mm, responsible for the compression of the right femoral vein (Figure 2). The patient denied any surgical intervention. Because of poor general health condition, we decided for a computer tomography-assisted puncture of the cyst. Fifty millilitres of serum-like fluid could be relieved and 40 mg triamcinolone acetonide was injected. In the first three days after evacuation of the cyst content, the swelling of the leg regressed completely. A clinical control after one year showed a regular venous flow in the right leg and a stable leg silhouette (Figure 3).
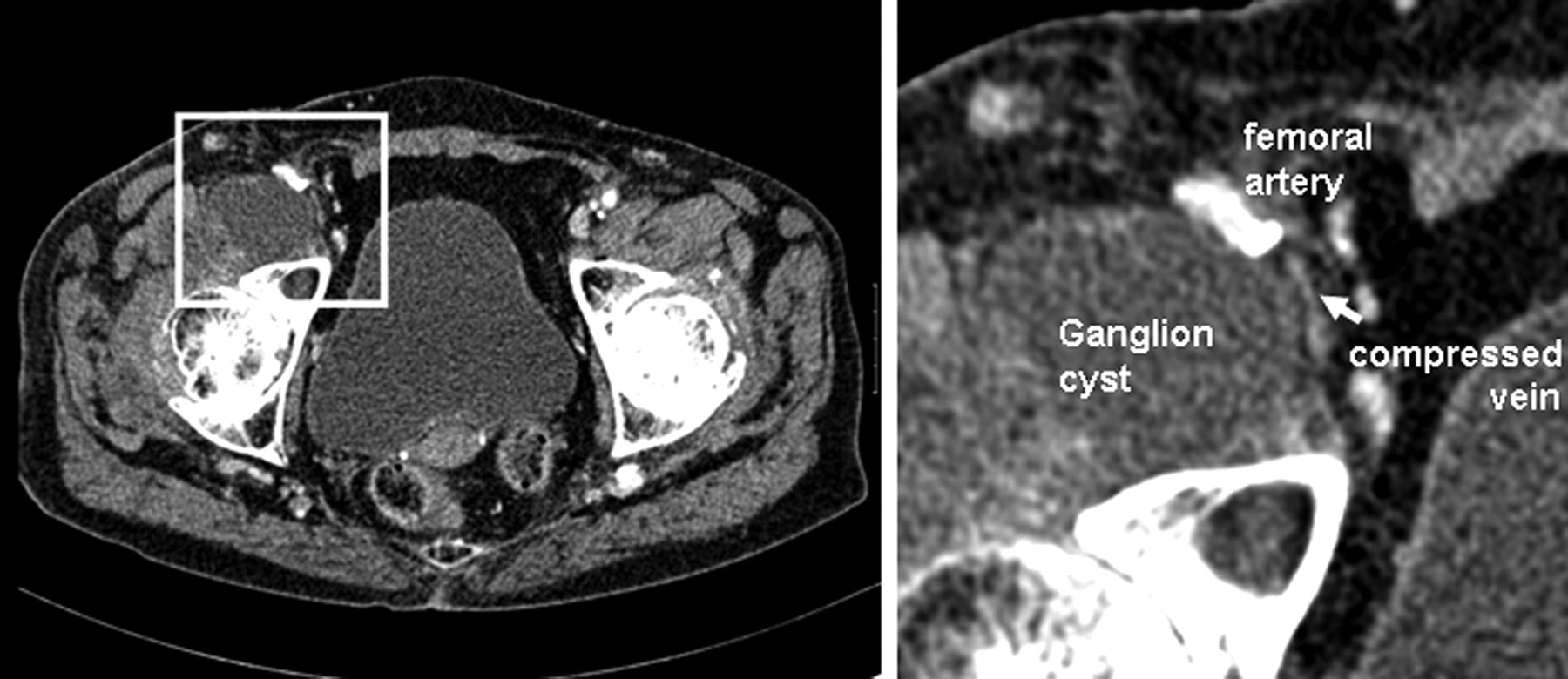
Computer tomography of the inguinal region. On the right side a tumour with an axial diameter of 47 × 31 mm and a coronar diameter of 36 × 90 mm, hypodense, with a flat wall, compressing the common femoral vein

A 92-year-old lady 12 months after treatment, with leg silhouettes being symmetrical
Discussion
Physical examination findings, clinical suspicion and established clinical prediction rules can accurately dictate the appropriate referral action necessary for making a diagnosis of DVT. The standard diagnostic approach to suspected DVT is lower limb CUS of proximal and distal deep veins. 3 In both of our patients we initially had a suspected DVT (Table 2). In the investigations ganglion cysts were suspected found. In one case surgical removal of the cyst and in the second case computer tomography-assisted puncture of the cyst and injection of triamcinolone acetonide were performed. After treatment the patients recovered and had no relapse after 12 months evaluation.
The unilateral leg swelling is highly suspicious of DVT. Even if the clinical Score (Wells Score) is high, other reasons have to be considered. One must think about other factors for such acute or subacute swelling, as in the presented two cases an extrinsic compression impeded the venous flow. Most frequently a ruptured Baker's cyst at the level of the popliteal vein is responsible for unilateral distal leg oedema. The presence of Baker's cyst is quite common. Rarely the cysts clinically demonstrate a compression syndrome of the vessels and nervous system in the popliteal fossa. Ruptured Baker's cyst can imitate a deep venous thrombosis. 4,5 Further, unilateral leg oedema can be caused through suprainguinal congestion because of various benign and maligne tumours. In literature, cases of leg oedema through arterial adventitial cystic disease, 6 unilateral lymphoma, 7 cavernous lymphangioma, 8 abdominal aortic aneurysm with aortoiliacal fistula, 9 retroperitoneal ganglioneuroma 10 and prostate cancer 11 have been described. Even in autoimmune diseases like linear morphea, 12 and in metabolic disease with liver cirrhosis 13 or in glomerulonephritis an unilateral leg oedema can occur.
Extrinsic femoral vein compression due to joint-related cysts have been previously reported. Five cases of compression due to synovial cyst from the hip joint and one case of compression secondary to a postoperative lymphocoele have been observed. 14 In the area of the hip joints 14 bursae are described. Bursa iliopectinea is the largest bursa between the iliopsoas tendon and the iliopubic eminence (Figure 4). The ganglion of the hip is a benign disease, a synovial protuberance as a result of high pressure in the joint. The size of the bursa iliopectinea is usually larger than its size described in textbooks of anatomy. Proximally the synovial bursa lies on the pectineal eminence of the superior pubic ramus, passes across the front of the capsule of the hip joint and extends distally downwards almost as far as to the lesser trochanter. Only the tendon of the psoas major muscle normally has an immediate relation to the bursa. With regard to modern diagnostic techniques (CUS, computer tomography, magnetic resonance tomography) the results are important for the differential diagnosis of tumours and inflammatory processes in hip joints. 15 A study of 80 anatomical preparations and CT scans of 130 patients has shown that the ilio-pectineal bursa may be non-communicating, communicating to the joint and/or septated. 16 In 14% the bursa iliopectinea communicates with the hip joint. Ganglia can be pulsating while being next to the arteries. When patients complain about pain in the inguinal region, besides degenerative, infectious or rheumatic joint diseases, conditions such as abscess, hernia, pseudoaneurysm, lymphocele, an iliopectineal bursitis should also be considered. The underlying disease of the hip joint plays a key role in the aetiopathogenesis of iliopectineal bursitis. Both of our patients had signs of degenerative joint disease and back pain. Iliopectineal bursitis is associated with chronic hip synovitis present in degenerative, infectious or rheumatic joint diseases.

Image of the bursa iliopectinea between the iliopsoas tendon and the iliopubic eminence
The treatment of the enlarged bursa iliopectinea is not sufficiently established because of the rare occurrence. Treatment options include watchful waiting, non-operative aspiration/injection and surgical removal. Both therapeutic options, the surgical or the interventional decompression seem to be promising. The surgical treatment of iliopectineal bursitis includes comprehensible excision or resection of the bursa, because of the important structures adjacent and a possible communication to the hip joint must be eradicated. 17 In addition to bursa resection, treatment of the affected joint should be taken into account. 18 Surgery generally results in lower rates of recurrence, but a higher incidence of complications. Inadequate excision can lead to recurrence. Cyst aspiration/injection is fraught with a high incidence of recurrence. All current interventional treatment options are aspiration with multiple punctures and injection of a sclerosant, like steroids, sodium morrhuate, ethanolamine, 19 iodine or carbolic acid, 20 have led to different outcomes. Mackie et al. report a recurrence of 93% in 1985 and McEvedy had a 82% success rate. Potential causes of the different outcomes may be a small collection of patients, short and incomplete follow-up times, with statistical error. Enhancing inflammation by injection of a sclerosing agent can have limited success because the wall of the ganglion is essentially acellular, and thus possesses limited potential to produce any mediators of inflammation. Also considering the natural history of a ganglion, that can also have a spontaneous regression.
Conclusion
Leg swelling is a common presenting complaint in the emergency department and may involve a variety of aetiologies. In a situation with low risk for DVT and a negative CUS, phlebologists should also think about further differential diagnosis and uncommon causes. Treatment depends on the size, location of the ganglion, the compression symptoms and the constitution of the patient with his comorbidities.